Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
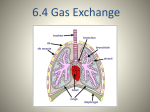
Station One: The Effect of Altitude on Respiration The effects of high altitude on humans are considerable. The amount of oxygen hemoglobin can carry directly affects the amount of oxygen in our blood. The higher the altitude the less oxygen hemoglobin can carry. After the human body reaches around 2,100 m (7,000 feet or 40kPa) above sea level, the saturation of oxyhemoglobin (hemoglobin +oxygen complex) begins to plummet. However, the human body has both short-term and long-term adaptations to altitude that allow it to partially compensate for the lack of oxygen. SHORT TERM adaptations include breathing faster and deeper (hyperventilates) at high altitude – it is necessary to do this in order to survive. The function of the lungs is to expose blood to fresh air, and breathing faster essentially increases the flow of oxygen past the blood. LONG TERM exposure to low oxygen levels results in the secretion of erythropoietin (EPO). EPO stimulates the production of red blood cells. Increasing the amount of red blood cells increases the amount of oxygen that can be absorbed from the air and delivered to the body cells. Athletes often train at high altitudes to increase their red blood cells from 5million/mL to 7million/mL. Red blood cells remain alive for 90 to 120 days so the benefits are long lasting. Synthetic EPO (used to treat anemia) is a banned substance for the Olympics. Detectable when urine is sampled. There is a limit to the level of adaptation: mountaineers refer to the altitudes above 8,000 metres (26,000 ft) as the "death zone", where no human body can acclimatize. The death zone, in mountaineering, refers to altitudes above a certain point where the amount of oxygen is not high enough to sustain human life. Symptoms of mild altitude sickness include dizziness, shortness of breath, headaches and nausea. High altitude pulmonary edema (HAPE) is a life-threatening form of a pulmonary edema (fluid accumulation in the lungs) that occurs in otherwise healthy mountaineers at altitudes typically above 2,500 meters (8,200 ft) 1. Why would mountaineers climbing Mount Everest require oxygen tanks near the summit (8840m). 2. How does the human body respond as you move to higher elevation? 3. Why do athletes train at high altitudes? 4. Why can long term exposure to high altitudes be dangerous for someone? 5. Explain the following image This bottle was photographed at 3600m (left) then again at sea level (right) Station 2: Pressure and Diffusion In addition to surface area, gas exchange occurs as a result of varying concentrations of gases on each side of the respiratory membranes. The SI unit for pressure is the pascal (Pa). A pascal is the force of one newton exerted on an area of one square meter. Since a pascal is a small unit, pressures are often measured in kilopascals. The atmospheric pressure of all gases at sea level is 101.3 kPa. At the top of mount Everest the pressure is 31kPa. The composition of gases does not change, but the densities do. Partial pressure: the pressure of each of the individual gases that make up the total pressure of a mixture of gases. Example: the percentage of oxygen in our atmosphere is 20.9%, so at sea level where the total pressure of gases is 101.3 kPa, 20.9% of that pressure is from oxygen. What is the partial pressure of oxygen? Analysis: 101.3kPa X 0.209 = 21.17kPa Therefore the pressure exerted by oxygen at sea level is 21.17kPa or PO2 =21.17 Application: Gases diffuse according to partial pressures. Gases will move from areas of high concentration/pressure to areas of low pressure. Low Partial pressure: Fewer gas molecules per volume High Partial Pressure: More gas molecules per volume 1. At higher altitudes the air is described as “thinner”. Explain what this means. 2. Why is it harder to breathe up in the mountain? Explain in terms of the partial pressure of oxygen. 3. If the percentage of carbon dioxide in our atmosphere 0.0397%, what is the partial pressure of carbon dioxide PCO2 at sea level? Hint: use atmospheric pressure 101.3 kPa. 4. Gas exchange occurs at two locations in the body, in the alveoli and in the body cells. If oxygen moves from the alveoli to the blood stream, where is the partial pressure of oxygen highest? Station 3: Oxygen transport Oxygen is transported from the air that we breathe to each cell in the body. In general, gases move from an area of high concentration (pressure) to areas of low concentration (pressure) By the time the oxygen has reached the alveoli the PO2 has fallen to about 13.3kPa. This is because the PO2 of the gas in the alveoli is affected by residual stale air still in the alveoli and by the presence of water vapour. Gases diffuse into the liquid component of blood called plasma. 98.5% of the oxygen found in plasma is picked up by a molecule called hemoglobin. Hemoglobin is an iron containing protein in red blood cells, that binds to oxygen forming the complex called oxyhemoglobin . Deoxygenated blood is dark red and oxygenated blood is bright red. Blood without hemoglobin can carry 0.3mL of oxygen per 100ml, but with it can carry 20mL of oxygen per 100mL, almost 20 times the amount. Transport happens via hemoglobin 98.5% or via plasma 1.5% When oxygen reaches the body cells, the oxygen dissolved in the plasma dissolves into the interstitial fluid first, then into the tissue cells. This change the pressure of oxygen in the blood so the oxygen bound to hemoglobin separates, diffuses into the plasma, then into the interstitial fluid and then into the cells. There is still oxygen in blood that is considered deoxygenated. 5.33kPa PO2 in alveoli 13.3 kPa PO2 in atmosphere 21.17 kPa PO2 in blood at alveoli 5.33 Pa 1. There is a significant pressure difference for oxygen in these locations. Since diffusion happens from high to low concentration describe how the movement of oxygen happens. 2. Label the diagram below with arrows showing the direction of oxygen and carbon dioxide diffusion. Include a legend and include partial pressures. 3. Describe the benefit of having hemoglobin in our blood. 4. People who are anemic suffer from low iron, which is the key component of hemoglobin. Explain how this might contribute to symptoms like feeling tired. 5. In your own words describe how oxygen diffuses into the body cells. Station 4: Carbon DioxideTransport Carbon dioxide is produced by cells as a by-product of aerobic cellular respirations Carbon dioxide accumulates in cells and diffuses from the cells into the interstitial fluid Under normal conditions the pressure of carbon dioxide PCO2 in the interstitial fluid is 5.6kPa The pressure gradient is large enough for diffusion to occur 7% of carbon dioxide remains in solution in the plasma, 20% binds to hemoglobin to form carbaminohemoglobin, 73% reacts with water in plasma to carbonic acid, which splits into bicarbonate ions HCO3- and hydrogen H+ ions. Accumulation of hydrogen ions increases acidity in the plasma and can become life threatening Hemoglobin solves this issue. When oxygen is released, it attaches to H+ so it does not accumulate in the plasma. Bicarbonate ions stay in solution. In the lungs hydrogen ions separate from the Hemoglobin, rejoining the bicarbonate ions to form carbon dioxide and water. The PCO2 in the capillaries surrounding the alveoli is now 5.6kPa, and in the alveoli it is 5.33kPa The difference in partial pressures is now sufficient to diffuse carbon dioxide into the alveoli from high to low pressure The process of ventilation moves the carbon dioxide-rich air from the alveoli to the external environment Questions: 1. Write out three chemical word equations to describe what happens to 73% of the carbon dioxide in our plasma. One for the reaction with water, one for the splitting of carbonic acid to the ions and one for the reformation of carbon dioxide and water. 2. How does carbon dioxide move through the respiratory system? 3. What happens if too many hydrogen ions build in the blood? 4. What happens when the bicarbonate ions reach the lungs? Station 5: The Control of Breathing Breathing is involuntary. It is controlled by the combined efforts of the respiratory and the circulatory systems. Normal rhythmic movements are controlled by a portion of the brain stem (medulla oblongata). The signals sent out tell the diaphragm to contract, and the intercostals muscles to contract causing inhalation. Stretch receptors in the lungs send signals to the brain that the lungs have expanded, and the brain then stops signaling the diaphragm and the intercostal muscles to contract. The muscles relax and exhalation occurs Under stress( physical exercise) the internal intercostal muscles begin to expand and contract more causing an increased rate of breathing We can consciously override these signals for a short period, like when we intentionally hold our breath, talk, or sing. Override is controlled by higher brain centers. The rate of breathing is determined by the demand for oxygen or the need to eliminate carbon dioxide Levels of oxygen and carbon dioxide are continuously monitored by chemical receptors in the brain, in the arteries leaving the heart and the arteries going to the brain An increase in cellular respiration increases the amount of CO2 , which turns into carbonic acid, that lowers pH in the blood. The brain then sends out signals that increase breathing rate and the volume of inhalation, by forcing the intercostals muscles to contract more rapidly and more forcefully. Heart rate also increases to more quickly deliver the oxygenated blood Oxygen levels are a secondary control mechanism and usually do not signal a response until oxygen levels are well below normal. Receptors in arteries leaving the heart and going to the brain monitor this. Carbon dioxide levels usually have triggered a response before oxygen does. 1. How is breathing regulated? How does the respiratory system respond? How does the circulatory system respond? 2. Since there are no carbon dioxide receptors in the brain and carbon dioxide levels are the main source of regulation, explain how levels are monitored. 3. Draw a flow chart for how carbon dioxide regulates breathing.