Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Coronary artery disease wikipedia , lookup
Aortic stenosis wikipedia , lookup
Myocardial infarction wikipedia , lookup
Cardiac surgery wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Artificial heart valve wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
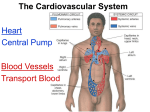
Hemodynamics Physics of Blood flow in the circulation Circulatory System • Heart: Has 2 collecting chambers - (Left, Right Atria) Has 2 Pumping chambers - (Left, Right Ventricles) Circulation Schematic Left Side of Heart Pulmonary Vein A Aorta V Aortic Valve Mitral Valve Tissues Lungs Tricuspid Valve Pulmonary Valve V Pulmonary Artery A Right Side of Heart Sup. & Inf. Vena Cava Heart Valves • Atrioventricular (A-V) valves - separate Atria from Ventricles • Bicuspid (Mitral) - Left Side • Tricuspid - Right Side • Semi-Lunar Valves - separate ventricles from Arteries Opening, Closing of Valves - Depends on Pressure differences between blood in adjacent areas Heart Sounds • ‘Lubb’ (1st sound) - Closure of A-V valves • ‘Dupp’ (2nd sound) - Closure of S-L valves Caused by Turbulence on closing. Anything extra ’Murmur’ (swishing of blood) Could be due to: Increases • Stenosis of Valves (calcification) Pressure on • Valves not closing properly heart (Incompetence, Insufficiency) Heart Sounds and Phonocardiography • Heart sounds are vibrations or sounds due to the acceleration or deceleration of blood during heart muscle contractions, whereas murmurs (a type of heart sounds) are considered vibrations or sounds due to blood turbulence. • Phonocardiographyis the recording of heart sounds. • Heart Sounds – The auscultation of the heart provides valuable information to the clinician concerning the functional integrity of the heart. Basic heart sounds • The first heart sound is generated at the termination of the atrial contractions, just at the onset of ventricular contraction. This sounds is generally attributed to movement of blood into the ventricles, the artioventricular (AV) valves closing, and the sudden cessation of blood flow in the atria. Splitting of the first heart sound is defined as an asynchronous closure of the tricuspid and the mitral valves. • The second heart sound is a low frequency vibration associated with the closing of the semilunar valves - the aortic and pulmonary valves. This sound is coincident with the completionof the T wave of the ECG. • The third heart sound corresponds to the sudden cessation of the ventricular rapidfilling. This low-amplitude, low frequency vibration is audible in children and in some adults. • The fourth heart sound occurs when the atria contracts and propel blood into the ventricles. This sound with very low amplitude and low frequency is not audible, but may be recorded by the phonocardiography (PCG). • The sources of most murmurs, developed by turbulence in rapidly moving blood, are known. Murmurs are common in children during early systolic phase; they are normally heard in nearly all adults after exercise. • Abnormal murmurs may caused by stenoses and insufficiencies (leaks) at the aortic, pulmonary, and mitral valves. They are detected by noting the time of their occurrence in the cardiac cycle and their location at the time of measurement. Auscultation and Stethoscopes • Heart sounds travel through the body from the heart and major blood vessels to the body surface. • The physician can hear those sounds with a stethoscope. • Basic heart sounds occur mostly in the frequency range of 20 to 200 Hz. • Certain heart murmurs produce sounds in the 1000-Hz region, and some frequency components exist down to 4 or 5 Hz. • Some researchers even reported that heart sounds and murmurs have small amplitudes with frequencies as low as 0.1 Hz and as high as 2000Hz. Stethoscopes: Historical and Current • Has been used for almost 200 years, and still being used nowadays for screening and diagnosis in primary health care. The typical frequency-response curve for a stethoscope • Many types of electronic stethoscopes have been proposed by engineers. These devices have selectable frequency-response characteristics ranging from the "ideal" flat-response case and selected bandpass to typical mechanicalstethoscope responses. • Physicians, however, have not generally accepted these electronic stethoscopes, mainly because they are unfamiliar with the sounds heard with them. Their size, portability, convenience, and resemblance to the mechanical one are other important considerations. Phonocardiography • Phonocardiography is an mechano-electronic recording technique of heart sounds and murmurs. • It is valuable in that it not only eliminates the subjective interpretation of these sounds, but also makes possible an evaluation of the heart sounds and murmurs with respect to the electrical (such as ECG) and mechanical (carotid pulse recorded in the midneck region) events in the cardiac cycle. • It is also valuable in locating the sources of various heart sounds. • A PCG machine is usually consist of four main parts: – – – – A microphone or PCG transducer, filtering (mechanical and electrical), processing unit, and display. • There are optimal recording sites for the various heart sounds or PCG signals. Because of the acoustical properties of the transmission path, heart sound waves are attenuated but not reflected. Figure shows four basic chest locations at which the intensity of sound from the four valves is maximized. • Auscultatory areas on the chest A, aortic; P, pulmonary; T, tricuspid; and M, mitral areas. Blood Vessels • Arteries • Capillaries • Veins Systemic Pathway: Left Ventricle of Heart Venules Aorta Arteries Arterioles Capillaries Veins Right Atrium of Heart Blood • Composition: – Approx 45% by Vol. Solid Components » Red Blood Cells (12m x 2 m) » White Cells » Platelets – Approx 55% Liquid (plasma) » 91.5% of which is water » 7% plasma proteins » 1.5% other solutes Blood Functions • Transportation of blood gases, nutrients, wastes • Homeostasis (regulation) of Ph, Body Temp, water content • Protection As a Result ……. • Blood behaves as a simple Newtonian Fluid when flowing in blood vessels i.e. Viscous stresses Viscosity, strain rate y du dy No slip at wall u(y) • Viscosity of Blood = 3 3.5 times of water • Blood acts as a non-newtonian fluid in smaller vessels (including capillaries) Cardiac Output • Flow of blood is usually measured in l/min • Total amount of blood flowing through the circulation = Cardiac Output (CO) Cardiac Ouput = Stroke Vol. x Heart Rate = 5 l/min Influenced by Blood Pressure & Resistance Force of blood against vessel wall with water retention with dehydration, hemorrage •Blood viscosity •Vessel Length •Vessel Elasticity •Vasconstriction / Vasodilation Overall • Greater Pressure Greater Blood Differences Flow • Greater Resistance Lesser Blood Flow Blood Pressure Driving force for blood flow is pressure created by ventricular contraction Elastic arterial walls expand and recoil continuous blood flow Blood pressure is highest in the arteries and falls continuously . . . Systolic pressure in Aorta: 120 mm Hg Diastolic pressure in Aorta: 80 mm Hg Typical values of circulatory pressures SP is the systolic pressure, DP the diastolic pressure, and MP the mean pressure. Ventricular pressure difficult to measure arterial blood pressure assumed to indicate driving pressure for blood flow Arterial pressure is pulsatile useful to have single value for driving pressure: Mean Arterial Pressure MAP = diastolic P + 1/3 pulse pressure Pulse Pressure = systolic pressure - ?? = measure of amplitude of blood pressure wave MAP influenced by • Cardiac output • Peripheral resistance MAP CO x Rarterioles • Blood volume – fairly constant due to homeostatic mechanisms (kidneys!!) BP too low: • Driving force for blood flow unable to overcome gravity O2 supply to brain Symptoms? BP too high: • Weakening of arterial walls - Aneurysm Risk of rupture & hemorrhage Cerebral hemorrhage: ? Rupture of major artery: BP estimated by Sphygmomanometry Auscultation of brachial artery with stethoscope Laminar flow vs. turbulent flow Typical indirect blood-pressure measurement system The sphygmomanometer cuff is inflated by a hand bulb to pressures above the systolic level. Pressure is then slowly released, and blood flow under the cuff is monitored by a microphone or stethoscope placed over a downstream artery. The first Korotkoff sound detected indicates systolic pressure, whereas the transition from muffling to silence brackets diastolic pressure. Principles of Sphygmomanometry Cuff inflated until brachial artery compressed and blood flow stopped what kind of sound? Slowly release pressure in cuff: turbulent flow Pressure at which . . . . . . sound (= blood flow) first heard: . . . sound disappeared: Ultrasonic determination of blood pressure A compression cuff is placed over the transmitting (8 MHz) and receiving (8 MHz ±D ƒ) crystals. The opening and closing of the blood vessel are detected as the applied cuff pressure is varied. • Pressure can be stated in terms of column of fluid. mm Hg 50 100 200 300 400 Pressure Units cm H2O PSI 68 136 272 408 544 0.9 1.9 3.8 5.7 7.6 ATM 0.065 0.13 0.26 0.39 0.52 Pressure = Height x Density or P = gh Density of blood = 1.035 that of water If Right Atrial pressure = 1 cm H2O in an open column of blood Pressure in feet = 140 cm H2O Rupture Incompetent venous valves Varicosities Venous Valves Actual Pressure in foot = 4-5 cm H2O Pressures in the circulation • Pressures in the arteries, veins and heart chambers are the result of the pumping action of the heart • The right and left ventricles have similar waveforms but different pressures • The right and left atria also have similar waveforms with pressures that are similar but not identical 3. As blood enters the aorta, the aortic pressure begins to rise to form the systolic pulse 4. As the LV pressure falls in late systole the aortic pressure falls until the LV pressure is below the aortic diastolic press. 2. Pressure rises until the LV pressure exceeds the aortic pressure 5. Then the aortic valve closes and LV pressure falls to LA pressure The blood begins to move from the ventricle to the aorta 1. The LV pressure begins to rise after the QRS wave of the ECG •The first wave of atrial pressure (the A wave) is due to atrial contraction •The second wave of atrial pressure (the V wave) is due to ventricular contraction Normal Pressures • RV and pulmonary systolic pressure are 12-15 mm Hg • Pulmonary diastolic pressure is 6-10 mm Hg • LA pressure is difficult to measure because access to the LA is not direct AS produces a pressure gradient between the aorta and LV i.e. For blood to move rapidly through a narrowed aortic valve orifice, the pressure must be higher in the ventricle • The severity of AS is determined by the pressure drop across the aortic valve or by the aortic valve area • The high velocity of blood flow through the narrowed valve causes turbulence and a characteristic murmur AS can be diagnosed with a stethoscope (a) Systolic pressure gradient (left ventricular-aortic pressure) across a stenotic aortic valve. (b) Marked decrease in systolic pressure gradient with insertion of an aortic ball valve. Pressure Measurement • Accurate pressure measurements are essential to understanding the status of the circulation • In 1733 Steven Hales connected a long glass tube directly to the left femoral artery of a horse and measured the height of a column of blood (8 feet, 3 inches) to determine mean BP • Direct pressure measurements are made frequently in the cardiac catheterization laboratory, the ICU and the OR • A tube is inserted into an artery and connected to an electrical strain gauge that converts pressure into force that is sensed electrically • The output of the transducer is an electrical signal that is amplified and recorded on a strip chart • For correct pressure measurements the cannula and transducer must be free of air, the cannula should be stiff and short Flush solution under pressure Sensing port Sample and transducer zero stopcock Roller clamp Electrical connector Disposable pressure transducer with an integral flush device Extravascular pressure-sensor system A catheter couples a flush solution (heparinized saline) through a disposable pressure sensor with an integral flush device to the sensing port. The three-way stopcock is used to take blood samples and zero the pressure sensor. Sensor (a) P Diaphragm Catheter Liquid Rc Lc Incremental length Rc Lc Rc DV Lc Rs Ls (b) Cc Cc Cc Cs C d= (a) Physical model of a catheter-sensor system. (b) Analogous electric system for this catheter-sensor system. Each segment of the catheter has its own resistance Rc, inertance Lc, and compliance Cc. In addition, the sensor has resistor Rs, inertance, Ls, and compliance Cs. The compliance of the diaphragm is Cd. DV DP