Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
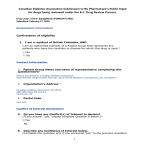
Journal Club Mingrone G, Panunzi S, De Gaetano A, Guidone C, Iaconelli A, Leccesi L, Nanni G, Pomp A, Castagneto M, Ghirlanda G, Rubino F. Bariatric Surgery versus Conventional Medical Therapy for Type 2 Diabetes. N Engl J Med. 2012 Mar 26. [Epub ahead of print] Wilding JP, Woo V, Soler NG, Pahor A, Sugg J, Rohwedder K, Parikh S; for the Dapagliflozin 006 Study Group. Long-Term Efficacy of Dapagliflozin in Patients With Type 2 Diabetes Mellitus Receiving High Doses of Insulin: A Randomized Trial. Ann Intern Med. 2012 Mar 20;156(6):405-415. 2012年4月5日 8:30-8:55 8階 医局 埼玉医科大学 総合医療センター 内分泌・糖尿病内科 Department of Endocrinology and Diabetes, Saitama Medical Center, Saitama Medical University 松田 昌文 Matsuda, Masafumi The authors evaluated the efficacy of intensive medical therapy alone versus medical therapy plus Roux-en-Y gastric bypass or sleeve gastrectomy in 150 (50 each) obese patients with uncontrolled type 2 diabetes. The mean (±SD) age of the patients was 49±8 years, and 66% were women. The average glycated hemoglobin level was 9.2±1.5%. Figure 1. Changes in Measures of Diabetes Control from Baseline. Values for change in glycated hemoglobin (Panel A), change in fasting plasma glucose (Panel B), the average number of diabetes medications (Panel C), and change in body-mass index (BMI) (Panel D) were plotted at 3, 6, 9, and 12 months. Least-square means and standard errors from a repeated measures model are plotted for glycated hemoglobin, average number of medications, and BMI; medians and interquartile ranges are plotted for fasting plasma glucose. P values are for the comparison between each surgical group and the medical-therapy group and were calculated from a repeated-measures model that considers data over time. 10.1056/nejmoa1200225 nejm.org the Departments of Internal Medicine (G.M., C.G., A.I., L.L., G.G.) and Surgery (G.N., M.C., F.R.), Università Cattolica S. Cuore; and National Research Council of Italy–Institute of Systems Analysis and Computer Science (IASI), BioMatLab (S.P., A.D.G.) 10.1056/nejmoa1200111 nejm.org Background Roux-en-Y gastric bypass and biliopancreatic diversion can markedly ameliorate diabetes in morbidly obese patients, often resulting in disease remission. Prospective, randomized trials comparing these procedures with medical therapy for the treatment of diabetes are needed. Methods In this single-center, nonblinded, randomized, controlled trial, 60 patients between the ages of 30 and 60 years with a body-mass index (BMI, the weight in kilograms divided by the square of the height in meters) of 35 or more, a history of at least 5 years of diabetes, and a glycated hemoglobin level of 7.0% or more were randomly assigned to receive conventional medical therapy or undergo either gastric bypass or biliopancreatic diversion. The primary end point was the rate of diabetes remission at 2 years (defined as a fasting glucose level of <100 mg per deciliter [5.6 mmol per liter] and a glycated hemoglobin level of <6.5% in the absence of pharmacologic therapy). Medical Therapy Patients in the medical-therapy group were assessed and treated by a multidisciplinary team that included a diabetologist, a dietitian, and a nurse, with planned visits at baseline and at 1, 3, 6, 9, 12, and 24 months after study entry. Oral hypoglycemic agents and insulin doses were optimized on an individual basis with the aim of reaching a glycated hemoglobin level of less than 7%. Programs for diet and lifestyle modification, including reduced overall energy and fat intake (<30% total fat, <10% saturated fat, and high fiber content) and increased physical exercise (≥30 minutes of brisk walking every day, possibly associated with moderateintensity aerobic activity twice a week), were designed by an experienced diabetologist with assistance from a dietitian. Bariatric Surgery Patients who were assigned to undergo either gastric bypass or biliopancreatic diversion were evaluated by a multidisciplinary team (including a diabetologist, a dietitian, and a nurse) at baseline and at 1, 3, 6, 9, 12, and 24 months after surgery. (A detailed description of the surgical procedures is provided in the Supplementary Appendix, available at NEJM.org.) Medical therapy was adjusted according to the seven-point glycemic profile during the first 3 months and according to glycated hemoglobin levels thereafter. Discontinuation of medical therapy was considered in cases of normalization of the glycemic profile, glycated hemoglobin levels, or both. Daily multivitamin and mineral supplementation was prescribed to the surgical groups; patients undergoing biliopancreatic diversion received additional vitamin D and calcium supplementation. Figure: RYGB. Copyright is retained by Cine-Med and has been kindly granted for publication. Figure: BPD. Copyright is retained by Cine-Med and has been kindly granted for publication. * Plus–minus values are means ±SD. † P values for the overall comparisons were calculated with the use of analysis of variance. P values for the comparisons between each of the two surgical procedures and medical therapy and for the comparison between the two types of surgery were calculated with the use of the Bonferroni method in post hoc analyses. There were no operative deaths among patients undergoing either gastric bypass or biliopancreatic diversion. An incisional hernia requiring reoperation 9 months after surgery developed in a patient undergoing biliopancreatic diversion, and one patient undergoing gastric bypass had an intestinal obstruction requiring reoperation 6 months after surgery. Two patients who were receiving medical therapy had persistent diarrhea associated with metformin, a condition that resolved when the drug was discontinued and another oral hypoglycemic agent was substituted. Results At 2 years, diabetes remission had occurred in no patients in the medical-therapy group versus 75% in the gastric-bypass group and 95% in the biliopancreaticdiversion group (P<0.001 for both comparisons). Age, sex, baseline BMI, duration of diabetes, and weight changes were not significant predictors of diabetes remission at 2 years or of improvement in glycemia at 1 and 3 months. At 2 years, the average baseline glycated hemoglobin level (8.65±1.45%) had decreased in all groups, but patients in the two surgical groups had the greatest degree of improvement (average glycated hemoglobin levels, 7.69±0.57% in the medical-therapy group, 6.35±1.42% in the gastric-bypass group, and 4.95±0.49% in the biliopancreatic-diversion group). Conclusions In severely obese patients with type 2 diabetes, bariatric surgery resulted in better glucose control than did medical therapy. Preoperative BMI and weight loss did not predict the improvement in hyperglycemia after these procedures. (Funded by Catholic University of Rome; ClinicalTrials.gov number, NCT00888836.) Message 手術による治療が肥満患者にはよさそうなのだ が... The success of various types of bariatric surgery suggests that they should not be seen as a last resort. Such procedures might well be considered earlier in the treatment of obese patients with type 2 diabetes. Message 体格指数35以上の高度肥満の2型糖尿病患者60人 を対象に、薬物療法と減量手術の血糖コント ロール改善効果を無作為化試験で比較。2年後の 糖尿病寛解率(空腹時血糖値<100mg/dLおよび HbA1c<6.5%)は薬物療法群の0%に対し、胃バ イパス術群で75%、胆膵路転換手術群で95% だった(それぞれP<0.001)。 New hypoglycemic drugs ● ● ● ● Amylin The 53rd Annual Meeting of the Japan Diabetes Society 27 May, 2010 Okayama Hydroxychloroquine Inhaled insulin SGLT-2 (sodium glucose transportor-2) inhibitors – ● Glucokinase activators – ● Prof. McGuill JB GPR 40 (G-protein coupled receptor 40) agonists – ● Dr. Eiki J PPARx – ● Prof. Ferrannini E Dr. Takeuchi K Bromocriptine – Prof. Matsuda 糖毒性の概念形成にフロリジンは重要な役割を果たした! Dapagliflozin Dapagliflozin (rINN/USAN) is an experimental drug being studied by BristolMyers Squibb in partnership with AstraZeneca as a potential treatment for type 1 and 2 diabetes. Although dapagliflozin's method of action would operate on either type of diabetes or other conditions resulting in hyperglycemia, the current clinical trials specifically exclude participants with Type 1 diabetes. In July 2011 an FDA committee recommended against approval until more data was available. The Prescription Drug User Fee Act (PDUFA) date for dapagliflozin for the treatment of Type 2 diabetes was extended three months by the FDA to January 28, 2012. (Dapagliflozin Declined by FDA) SGLT2 inhibitors: Canagliflozin Dapagliflozin Remogliflozin Sergliflozin http://en.wikipedia.org/wiki/Dapagliflozin Nonselective SGLT inhibitors block adenosine triphosphate– dependent, sodium-linked facilitated transport of glucose across the brush border cells of the small intestine (isoform SGLT1) and renal tubular epithelium (dominantly isoform SGLT2), leading to decreased intestinal absorption and renal tubular resorption of glucose http://img.medscape.com/fullsize/migrated/editorial/conferences/2008/15780/wilding.fig1.gif Austria: Hoppichler F, Luger A, Prager R, Roden M, Kotter T, and Schernthaner G. Bulgaria: Borisova A, Daskalova I, Hristozov K, Lazarova G, Orbetzova M, Petkova M, Slavcheva A, Stoykova Y, Tankova C, Veleva N, and Zaharieva S. Canada: Ardilouze J, Aronson R, Boucher P, Carthy J, Dzongowski P, Gaudet D, Godsell S, Goldenberg R, Hart R, Houlden R, Kaiser S, Khandwala H, Landry D, Lau D, O’Keefe D, Sigalas J, Tellier G, Twum-Barima Y, and Woo V. Finland: Alanko J, Kurl S, Ma¨kela¨ J, Niskanen L, Paul R, Perhonen M, Pihlman S, Rissanen A, Strand J, Valle T; Germany: Bieler T, Fuchs F, Go¨tze D, Hanefeld M, Mo¨lle A, Paschen B, Rose L, Schumacher M, Semmler S, Sehnert W, Tillenburg B, Wendisch U, and Winkelmann B. Great Britain: Bain S, Farmer I, Jassel GS, Owen D, Reed R, Simpson H, Strang C, and Wilding J. Hungary: Dea´k L, Gurzo´ M, Hegyi I, Kere´nyi Z, La´szlo´czky A´ , Pa´ll K, Pe´nzes J, Reiber I, Re´ve´sz K, Somogyi A, Tama´s G, and Va´ndorfi G. The Netherlands: Castro Cabezas M, de Koning E, Timmerman R, and van de Wiel A. Romania: Crisan C, Ferariu I, and Vlaiculescu M. Russian Federation: Arutyunov G, Dreval A, Grineva E, Karpova I, Kobalava Z, Krasilnikova E, Kukharchuk V, Lantseva O, Pavlova M, Privalov D, Strongin L, Tereschenko S, Vorokhobina N, and Zhelninova T. Slovakia: Belesova K, Fabry J, Kupcova T, Macko M, Paulovic V, Tomasova L, Truban J, and Vargova A. Spain: Calle Pascual A, De Teresa Parren˜o L, Dura´n Garcı´a S, Freixenet N, Gomis de Barbara´ R, Gonza´lez Albarra´n O, and Gonza´lez Clemente JM. United States: Bernstein R, Brusco O, Graf R, Freeman J, Hoekstra J, Khairi R, Lubin B, Norwood P, Reed J, Rosenstock J, Soler N, Sugimoto D, and Wahl T. Dr. Wilding: Diabetes and Endocrinology Research Group, Department of Obesity and Endocrinology, Clinical Sciences Center, University Hospital Aintree, Longmoor Lane, Liverpool L9 7AL, United Kingdom. Dr. Woo: Section of Endocrinology, Health Sciences Center, University of Manitoba, Winnipeg, Manitoba R3T 2N2, Canada. Dr. Soler: Springfield Diabetes and Endocrine Center, Hospital Sisters Health System Medical Group, 2501 Chatham Road, Suite 300, Springfield, IL 62704. Drs. Pahor and Rohwedder: AstraZeneca, Tinsdaler Weg 183, D-22880 Wedel, Germany. Ms. Sugg and Dr. Parikh: AstraZeneca, 1800 Concord Pike, Box 15437, Wilmington, DE 19850-5437. Ann Intern Med. 2012;156:405-415. Background: Dapagliflozin, a selective inhibitor of sodium–glucose cotransporter 2, may improve glycemic control with a lower dose of insulin and attenuate the associated weight gain in patients with inadequate control despite high doses of insulin. Objective: To evaluate the efficacy and safety of adding dapagliflozin therapy in patients whose type 2 diabetes mellitus is inadequately controlled with insulin with or without oral antidiabetic drugs. Design: A 24-week, randomized, placebo-controlled, multicenter trial followed by a 24-week extension period. An additional 56week extension period is ongoing. (ClinicalTrials.gov registration number: NCT00673231) Setting: 126 centers in Europe and North America from 30 April 2008 to 19 November 2009. Patients: 808 patients with inadequately controlled type 2 diabetes mellitus receiving at least 30 U of insulin daily, with or without up to 2 oral antidiabetic drugs. Intervention: Patients were randomly assigned in a 1:1:1:1 ratio and allocated with a computer-generated scheme to receive placebo or 2.5, 5, or 10 mg of dapagliflozin, once daily, for 48 weeks. Measurements: The primary outcome was change in hemoglobin A1c from baseline to 24 weeks. Secondary outcomes included changes in body weight, insulin dose, and fasting plasma glucose level at 24 weeks and during the 24-week extension period. Adverse events were evaluated throughout both 24-week periods. Figure 1. Study flow diagram. DAPA dapagliflozin; INS insulin; OAD oral antidiabetic drug; PLA placebo. * This patient received no study medication or postbaseline assessments. Table 1. Major Demographic and Baseline Characteristics BMI body mass index; HbA1c hemoglobin A1c; OAD oral antidiabetic drug. Appendix Figure 1. Adjusted mean changes in daily insulin dose over time. Appendix Figure 1. Adjusted mean changes in daily insulin dose at 48 weeks. Samples are patients in the full analysis set with nonmissing baseline values and nonmissing values for a given time point. Sample sizes at time 0 are 191, 200, 209, and 194 for the PLA, 2.5-mg DAPA, 5-mg DAPA, and 10-mg DAPA groups, respectively. Treatment group symbols are shifted horizontally to prevent the error bars from overlapping. DAPA = dapagliflozin; INS = insulin; PLA = placebo. Appendix Figure 2. Probability of insulin up-titration due to not achieving prespecified glycemic targets or of discontinuation due to poor glycemic control over time. Symbols represent censored observations. “Week” is the actual number of days from the first dose of double-blind study medication divided by 7, not the scheduled visit week. Values for patients at risk are for the beginning of the period. DAPA = dapagliflozin; INS = insulin; PLA = placebo. Figure 2. Adjusted mean changes in HbA1c level over time. Figure 2. Adjusted mean changes in HbA1c level at 48 weeks. Samples are patients in the full analysis set with nonmissing baseline values and nonmissing values for a given time point. Sample sizes at time 0 are 193, 202, 211, and 193 for the PLA, 2.5-mg DAPA, 5-mg DAPA, and 10-mg DAPA groups, respectively. Treatment group symbols are shifted horizontally to prevent the error bars from overlapping. DAPA = dapagliflozin; HbA1c = hemoglobin A1c; INS = insulin; PLA = placebo. Appendix Figure 4. Change in mean HbA1c level over time calculated by using the placebo group to impute missing data in the safety analysis set and analyzed by treatment group and discontinuation status. DAPA = dapagliflozin; INS = insulin; PLA = placebo. Figure 3. Adjusted mean changes in total body weight over. Figure 3. Adjusted mean changes in total body weight at 48 weeks. Samples are patients in the full analysis set with nonmissing baseline values and nonmissing values for a given time point. Sample sizes at time 0 are 193, 202, 211, and 193 for the PLA, 2.5-mg DAPA, 5-mg DAPA, and 10-mg DAPA groups, respectively. Treatment group symbols are shifted horizontally to prevent the error bars from overlapping. DAPA = dapagliflozin; INS = insulin; PLA = placebo. UTI = urinary tract infection. * From patients in the safety analysis set. Includes data from after insulin up-titration. † Based on definitive preferred terms from Medical Dictionary for Regulatory Activities, version 12.1. ‡ A major episode was defined as a symptomatic episode in which the patient required external assistance due to severe impairment in consciousness or behavior, had a capillary or plasma glucose level <3 mmol/L (<54 mg/dL), and promptly recovered after receiving glucose or glucagon. A minor episode was defined as a symptomatic episode in which the patient had a capillary or plasma glucose level <3.5 mmol/L (<63 mg/dL), regardless of the need for external assistance, or an asymptomatic capillary or plasma glucose level <3.5 mmol/L (<63 mg/dL) that did not qualify as a major episode. Other episodes were defined as reported suggestive episodes that did not meet the criteria for a major or minor episode. No episodes of hypoglycemia led to study discontinuation. § Identified in the database by using prespecified lists of preferred terms. These events included signs, symptoms, and other reports suggesting genital infection or UTI as well as definitive terms for genital infection obtained from spontaneous reporting and active questioning at each study visit. ¶ Identified in the database by using prespecified lists of preferred terms but also by other indicators, such as serum creatinine level. Appendix Figure 3. Patients with events suggesting genital infection (top) or urinary tract infection (bottom) at 24 and 48 weeks. DAPA = dapagliflozin; INS = insulin; PLA = placebo. Most missing data in longitudinal clinical trials result from patients discontinuing therapy at a particular time point and subsequent data being unavailable; this is known as monotone missing data. A small amount of missing data may result from patients who skip a visit but return for subsequent visits, known as nonmonotone missing data. Results: 800 patients were analyzed. After 24 weeks, mean hemoglobin A1c decreased by 0.79% to 0.96% with dapagliflozin compared with 0.39% with placebo (mean difference, -0.40% [95% CI, -0.54% to -0.25%] in the 2.5-mg group, -0.49% [CI, -0.65% to -0.34%] in the 5-mg group, and -0.57% [CI, -0.72% to - 0.42%] in the 10-mg group). Daily insulin dose decreased by 0.63 to 1.95 U with dapagliflozin and increased by 5.65 U with placebo (mean difference, -7.60 U [CI, -10.32 to -4.87 U] in the 2.5-mg group, -6.28 U [CI, -8.99 to -3.58 U] in the 5-mg group, and - 6.82 U [CI, -9.56 to -4.09 U] in the 10-mg group). Body weight decreased by 0.92 to 1.61 kg with dapagliflozin and increased by 0.43 kg with placebo (mean differences, -1.35 kg [CI, -1.90 to - 0.80 kg] in the 2.5-mg group, -1.42 kg [CI, -1.97 to -0.88 kg] in the 5-mg group, and -2.04 kg [CI, -2.59 to -1.48 kg] in the 10-mg group). These effects were maintained at 48 weeks. Compared with the placebo group, patients in the pooled dapagliflozin groups had a higher rate of hypoglycemic episodes (56.6% vs. 51.8%), events suggesting genital infection (9.0% vs. 2.5%), and events suggesting urinary tract infection (9.7% vs. 5.1%). Limitation: Insulin doses were not titrated to target, and the study was not designed to evaluate long-term safety. Conclusion: Dapagliflozin improves glycemic control, stabilizes insulin dosing, and reduces weight without increasing major hypoglycemic episodes in patients with inadequately controlled type 2 diabetes mellitus. Primary Funding Source: AstraZeneca and Bristol-Myers Squibb. Steven A. Smith, MD, Mayo College of Medicine, 200 First Street SE, Rochester, MN 55905; e-mail, smith [email protected]. In a recent commentary, Ferrannini stated that the SGLT2 story was closed and that “reduced SGLT2 activity— whether genetically or experimentally induced—is efficacious and relatively safe in lowering hyperglycemia and its toxicity with the added benefits of a degree of weight control and some natriuresis.” In truth, after 2 centuries of study, we remain uncertain of the appropriate use and long-term safety of SGLT2 inhibition in persons with diabetes. Ann Intern Med. 2012;156:466-467. Gastrointestinal side effects are more commonly reported with dapagliflozin than with metformin Clinical trials suggested that genitourinary infections were more prevalent in the first 24 weeks, but because of the risk for asymptomatic urinary tract infections in diabetes, repetitive surveillance will probably be important. Although no significant increases in pyelonephritis or other potentially lifethreatening renal infections have been shown in dapagliflozin clinical trials, continued postmarketing surveillance will be necessary. Dapagliflozin seems to be less effective in patients with renal disease. In contrast to plausible concerns about renal glycosuria induced by SGLT2 inhibition in diabetic patients, preventing sodium and glucose resorption in diabetes may prevent proximal tubular epithelial growth, increased glomerular filtration, and accelerated protein glycation Wilding and colleagues comment that dapagliflozin is highly selective for the SGLT2 receptor, which is not expressed in bladder or breast tissue; however, the potential influence of its metabolites or its expression in tissue known to have functional receptors, such as brain, liver, thyroid, muscle, or heart tissue, or in metastatic carcinoma is currently unknown. Message 高用量インスリン治療中で血糖コントロール不十分 な2型糖尿病患者800人を対象に、SGLT2選択的阻害薬 dapagliflozin併用の有効性を無作為化プラセボ対照試 験で検討。24週後、HbA1c値の低下率は併用群(用量 2.5、5.0、10.0mg/日の3群)で0.79-0.96%、プラセボ 群で0.39%だった。 Ferrannini先生はこのクラスの薬物が臨床応用に供 され一段落としている。長期的な使用で問題があるか は今後の課題。 で、FDAが2011年7月の諮問委員会の膀胱癌と乳癌の 発癌性の可能性から認可していない。(...)