Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
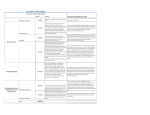
JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults April 22, 2016 Connie Tien Daniel Kim Jeffrey Hughes Michelle Di Fiore Ola Lafi Table of Contents • • • • • • • • • Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation Recommendation 1 Corollary Recommendation Recommendation 2 Recommendation 3 Recommendation 4 • • • • • • Recommendation 5 Recommendation 6 Recommendation 7 Recommendation 8 Recommendation 9 Evidence Based Dosing for Antihypertensive Drugs • Hypertension Guideline Management Algorithm • Sources Why Do We Treat Hypertension? • Hypertension can lead to: • • • • Myocardial infarction Stroke Renal failure Death Blood Pressure Treatment Goals • Persons 60 years or older without diabetes or CKD • BP < 150/90 (based on strong evidence) • Persons less than 60 years of age, with diabetes, and/or with CKD • BP <140/90 (based on expert opinion) Initial Therapy • Non-black persons • • • • Angiotensin-converting enzyme inhibitor (ACEI) Angiotensin receptor blocker (ARB) Calcium channel blocker (CCB) Thiazide-type diuretic • Black persons (including those with diabetes) • CCB • Thiazide-type diuretic • Chronic kidney disease (regardless of race or diabetes status) • ACEI or ARB as initial or add-on antihypertensive therapy Strength of Recommendation Recommendation 1 In the general population aged ≥60 years, initiate treatment at systolic blood pressure (SBP) ≥150 or diastolic blood pressure (DBP) ≥90 and treat to a goal SBP <150 and DBP <90. Strong Recommendation – Grade A Corollary Recommendation In the general population aged ≥60 years, if treatment results in lower achieved SBP (e.g. SBP <140) and treatment is well tolerated without adverse effects on health or quality of life, treatment does not need to be adjusted. Expert Opinion – Grade E Recommendation 2 In the general population <60 years, initiate treatment at DBP ≥90 and treat to a goal DBP <90. For ages 30-59 years, Strong Recommendation – Grade A For ages 18-29 years, Expert Opinion – Grade E Recommendation 3 In the general population <60 years, initiate treatment at SBP ≥140 and treat to a goal SBP<140. Expert Opinion – Grade E Recommendation 4 In the population aged ≥18 with chronic kidney disease (CKD), initiate treatment at SBP ≥140 or DBP ≥90 and treat to goal SBP <140 and DBP <90. Expert Opinion – Grade E Based on the inclusion criteria used in the randomized controlled trials (RCTs) reviewed by the panel, this recommendation applies to individuals <70 years with an estimated GFR or measured GFR <60 and in people of any age with albuminuria defined as >30 mg of albumin/g of creatinine at any level of GFR. Recommendation 5 In the population aged ≥18 years with diabetes, initiate treatment at SBP ≥140 or DBP ≥90 and treat to a goal SBP <140 and DBP <90. Expert Opinion – Grade E Recommendation 6 In the general nonblack population, including those with diabetes, initial antihypertensive treatment should include a thiazide-type diuretic, calcium channel blocker (CCB), angiotensin-converting enzyme inhibitor (ACEI), or angiotensin receptor blocker (ARB). Moderate Recommendation – Grade B RCTs that were limited to specific nonhypertensive populations, such as those with coronary artery disease (CAD) or heart failure (HF) were not reviewed for this recommendation. Therefore, recommendation 6 should be applied with caution to these populations. For more details regarding why other drug classes were not recommended for initial therapy please see the notes for this slide. Recommendation 7 In the general black population, including those with diabetes, initial antihypertensive treatment should include a thiazide-type diuretic or CCB. For general black population: Moderate Recommendation – Grade B For black patients with diabetes: Weak Recommendation – Grade C For more information regarding why the other drug classes were not recommended as initial therapy for black persons please see the notes for this slide. Recommendation 8 In the population aged ≥18 years with CKD, initial (or add-on) antihypertensive treatment should include an ACEI or ARB to improve kidney outcomes. This applies to all CKD patients with hypertension regardless of race or diabetes status. Moderate Recommendation – Grade B Recommendation 9 • The main objective of treatment is to attain and maintain goal BP. • If goal BP is not reached within a month of treatment, increase the dose of the initial drug or add a second drug from one of the classes in recommendation 6. • The clinician should continue to assess BP and adjust the treatment regimen until the goal BP is reached. • If goal BP cannot be reached with 2 drugs, add and titrate a third drug from the list provided in recommendation 6. • If goal BP cannot be reached using on the drugs in recommendation 6 because of a contraindication or the need to use more than 3 drugs to reach goal BP, antihypertensive drugs from other classes can be used. • Referral to a hypertension specialist may be indicated for patients in whom goal BP cannot be attained using the above strategy or for the management of complicated patients for whom additional clinical consultation is needed. Expert Opinion – Grade E Figure continued on following slide. Sources • James PA, Oparil S, Carter BL, et al. 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults: Report From the Panel Members Appointed to the Eighth Joint National Committee (JNC 8). JAMA. 2014;311(5):507-520. doi:10.1001/jama.2013.284427. Question #1 A 43 yo M is evaluated during a routine physical examination. He has no current symptoms and no PMH. FH is notable for DM and HTN in 2 1st degree relatives. He takes no meds. On physical exam, initial BP is 144/86; repeat measurement after 5 minutes of rest are 136/86 and 134/88. BMI is 32. The remainder of the exam is normal. Labs show normal Cr and plasma glucose levels. In addition to lifestyle modifications, which of the following is the most appropriate next step in the management of this patient’s blood pressure? A: Initiate a low dose ACE inhibitor B: Initiate low dose chlorthalidone C: Order ambulatory BP monitoring D: Recheck blood pressure in 1 year In addition to lifestyle modifications, which of the following is the most appropriate next step in the management of this patient’s blood pressure? A: Initiate a low dose ACE inhibitor B: Initiate low dose chlorthalidone C: Order ambulatory BP monitoring D: Recheck blood pressure in 1 year Answer • Although JNC 8 did not address pre-hypertension, JNC 7 defined it as SBP 120-139 or DBP 80-89 in the absence of pre existing disease • Lifestyle modifications: • Low salt diet, DASH diet, exercise regimen • Follow-up: annual visits. • Answer A &B: although there is increased risk of stroke, CV dx, and development of HTN, ACE inhibitor has not been shown to reduce the risk. • Answer C: Ambulatory BP monitoring records BP periodically during normal activities. Indicated for “white-coat” HTN, masked HTN, or confirm poor response to antihypertensive medications. Question 89 A 57 yo African American M is evaluated for treatment of newly diagnosed HTN. History is notable for HLD, which is treated with moderate-dose simvastatin. On exam, BP 151/94, HR 72, BMI 28. Remainder of exam is unremarkable. Labs show Cr 1.0, fasting glucose 104, and K+ 4.5. A urine dipstick demonstrates no blood or protein. In addition to recommending lifestyle modifications, which of the following is the most appropriate initial anti-hypertensive therapy for this patient? A: Amlodipine B: Diltiazem C: HCTZ D: Lisinopril In addition to recommending lifestyle modifications, which of the following is the most appropriate initial anti-hypertensive therapy for this patient? A: Amlodipine B: Diltiazem C: HCTZ D: Lisinopril Answer: • Patient is African American with stage 1 HTN. Thiazide diuretics and CCB alone or in combo are recommended by JNC 8. • Patient is on moderate dose statin that uses CYP3A4 pathway which can be inhibited by CCB and can cause increased statin myopathy, so thiazide diuretic would be more appropriate. • REMEMBER: African Americans have less BP response to reninangiotensin system agents despite similar plasma renin activity. • ACE inhibitor is not indicated Question 98 A 60 yo woman is evaluated during a follow-up visit for HTN. History is also notable for HLD. She tolerates her medications well except for minor pedal edema since starting her anti-hypertensive medication. She is active and plays tennis 3x/wk. Current medications are amlodipine 5mg/d and rosuvastatin. On exam, the average of 2 BP readings is 152/86 which is consistent with measurements she has obtained at home for 3 months. HR 64, BMI 22. Trace pedal edema is noted. Labs show normal chemistry panel and urine dipstick shows no protein. Which of the following is the most appropriate next step in management? A: Add Lisinopril B: Add metoprolol C: Increase amlodipine to 10mg/d D: Continue current regimen Which of the following is the most appropriate next step in management? A: Add Lisinopril B: Add metoprolol C: Increase amlodipine to 10mg/d D: Continue current regimen Answer • Patient has stage 1 hypertension and JNC 8 recommends BP goal <150/90 for patients >60 yo. • She has no evidence of CV or kidney dx and is not frail and has a longer expected lifetime than the general population of this age, cautious stepped care for lower blood pressure goals is reasonable. • Increasing dose of 1 agent is less effective in reducing BP then addition of 2nd agent at low dose, also avoids the risk of SIDE EFFECTS • Beta blocker is not indicated for the initial Rx of HTN • ACCOMPLISH trial demonstrated benefit of combo therapy with CCB and ACE inhibitor in reducing cardiovascular events compared to using a thiazide and ACE inhibitor Question 19 A 48 yo woman is evaluated during a follow up visit for newly diagnosed HTN, confirmed by multiple measurements at home and in the office. PMH of HLD for which she is taking atorvastatin. Lifestyle modifications have been recommended. On exam, BP 160/92, HR 64, BMI 32. Remainder of exam unremarkable. Labs show Cr 1.1mg/dL, fasting glucose 114 and K+ 4.0, urine dipstick demonstrates no blood or protein. Which of the following is most likely to be effective in controlling this patient’s HTN? A: Amlodipine B: Lisinopril C: Losartan D: Lisinopril and amlodipine E: Losartan and lisinopril Which of the following is most likely to be effective in controlling this patient’s HTN? A: Amlodipine B: Lisinopril C: Losartan D: Lisinopril and amlodipine E: Losartan and lisinopril Answer • Combination therapy with ACE inhibitor and amlodipine is appropriate with stage 2 HTN • Stage 2: SBP > 160 or DBP >100 • Single agent is unlikely to control BP who are >20/10mmg Hg above target BP. • Combo of 2 agents at moderate doses is more successful at achieving goal than 1 at maximal dose • Combos supported by JNC 8 • Thiazide w/ ACE inhibitor or ARB • CCB w/ ACE inhibitor or ARB • ACCOMPLISH trial demonstrated benefit of combo therapy with CCB and ACE inhibitor in reducing cardiovascular events compared to using a thiazide and ACE inhibitor • ACE and ARB should not be used in combination Question 10 A 51 yo M is evaluated during a follow up visit for management of newly diagnosed hypertension and diabetes. He started a program of lifestyle modifications for his DM, but hasn’t started anti-hypertensive medication. He currently takes no meds. On exam, BP 148/92, HR 76, BMI 33. The remainder of the exam was normal. Labs show Cr 1.5, K+4.2, urine dipstick with no hematuria or proteinuria and spot urine protein-creatinine ratio 50mg/g Which of the following is the most appropriate anti-hypertensive treatment for this patient? A: HCTZ B: Lisinopril C: Lisinopril and amlodipine D: Lisinopril and HCTZ E: Lisinopril and losartan Which of the following is the most appropriate anti-hypertensive treatment for this patient? A: HCTZ B: Lisinopril C: Lisinopril and amlodipine D: Lisinopril and HCTZ E: Lisinopril and losartan Answer: • Patient has Stage 1 HTN, DM, and CKD. • Regardless of DM status, ACEi/ARB have protective effect on kidney and is recommended by JNC8 with goal <140/90 • Recommendations for more aggressive BP goals <130/80 in this population have ben tempered by the lack of efficacy in reducing mortality and increase adverse events.