Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Drug discovery wikipedia , lookup
Discovery and development of beta-blockers wikipedia , lookup
Electronic prescribing wikipedia , lookup
Drug interaction wikipedia , lookup
Neuropharmacology wikipedia , lookup
Pharmacognosy wikipedia , lookup
Psychopharmacology wikipedia , lookup
Polysubstance dependence wikipedia , lookup
Prescription costs wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Psychedelic therapy wikipedia , lookup
Adherence (medicine) wikipedia , lookup
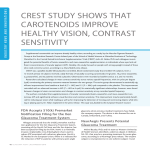
issue 3 2 010 Inside this issue: Special Focus: What’s New: Clinical Issues: Practical Tips: Quality Use of Fixed Combinations Mechanisms of Action of Fixed Combinations Fixed Combinations in Treatment Algorithms and Guidelines Fixed Combinations and Patient’s Perspective PAGE 2 PAGE 5 PAGE 9 PAGE 10 LEARNING OBJECTIVES •Special Focus: Action of components, limitations and additivity, effects and side effects, cost issues. •What’s New: Mechanisms of action, patient case study, choice of combination products •Clinical Issues: Fixed combinations in the treatment algorithm, reference in guidelines. Practical Tips: Patient perspective: factors influencing adherence, quality of life, costs. TARGET AUDIENCE This educational activity is aimed at general ophthalmologists, glaucoma specialists and ophthalmology residents. EDITORIAL BOARD Clive Migdal MD, FRCS, FRCOphth Western Eye Hospital, London, UK. Main topic issue No 3: Fixed Combinations – Concept of Use Glaucoma Now is a continuing medical education publication. Distributed worldwide to approximately 40,000 ophthalmologists, our goal is to educate and update general ophthalmologists, glaucoma specialists and ophthalmology residents. International leaders in the field of glaucoma are invited to contribute to this journal, sharing their most recent insights. Supported by an unrestricted educational grant, the publication is non-promotional and has a fully independent Editorial Board. Glaucoma Now is in the process of gaining accreditation for Continuing Medical Education (CME) by the European Accreditation Council for Continuing Medical Accreditation. Ivan Goldberg MD, FRANZCO, FRACS Sydney Eye Hospital, Sydney, NSW, Australia. Remo Susanna MD, Professor and Head of Department of Ophthalmology, University of São Paulo, Brazil. Glaucoma Now – No3. www.glaucomanow.com Glaucoma Now is published and administered by the editorial board and supported by an unrestricted educational grant from Allergan, Inc. Executive officer: Patricia Buchholz RPh, PhD Karlsruhe, Germany [email protected] Copyright 2010 Editorial Board. All rights reserved. No responsibility assumed for injury or damage to persons or property arising from the use of information or ideas contained in this publication. Production by Phosworks www.phosworks.se 1 Special Focus: Quality Use of Fixed Combinations Francisco Javier Goñi MD, PhD1. Mercè Guarro MD2 1. Chief of the Integrated Dept of Ophthalmology, Hospitals of Granollers, Mollet and Sant Celoni. Co-director of Barcelona Glaucoma Centre-IOB-USP 2. Coordinator of the Integrated Dept of Ophthalmology, Hospitals of Granollers, Mollet and Sant Celoni Core Concepts • Beta blockers (BBs) and alpha agonists (AAs) reduce aqueous formation by decreasing the rate of movement of water to the ciliary non-pigmented epithelial (NPE) aqueous surface. • Carbonic anhydrase inhibitors (CAIs) reduce aqueous production by decreasing bicarbonate formation, thus preventing sodium and water movement from the non pigmented epithelial cells. • Prostaglandin analogs (PGAs) increase uveoscleral outflow of aqueous. While all other PGAs activate the FP receptor, bimatoprost seems to act through a variant of this receptor. Action of components Mechanism of action: Ocular hypotensive FDCs are products that include two active agents in the same bottle. All currently available FDCs include timolol – a nonselective beta-blocker at the concentration of 5 mg per ml (0.5%). The other drug is a PGA, including bimatoprost, latanoprost or travoprost; the alpha-agonist brimonidine, a CAI, (brinzolamide or dorzolamide),; or the cholinergic agent pilocarpine at 2% or 4% concentrations (1). Although mechanisms of action of these drugs are different, all of them reduce IOP either by reducing aqueous production (AP) or by facilitating aqueous outflow (AO). (3,4,5). CAIs reversibly bind to the almost ubiquitous enzyme carbonic anhydrase II, hindering it from catalyzing its reaction (6). This reduces the production of bicarbonate and consequently aqueous humor formation. PGAs increase uveoscleral outflow, the alternative route for aqueous outflow, and can be classified as AO facilitators (8). Among the different PGAs available as fixed combinations, latanoprost 2 • PGAs are the most potent hypotensive drugs available, reducing IOP up to 31-33% from baseline. • PGAs reduce IOP for at least 24 hours, consistently flattening the circadian curve better than CAIs, AAs or BBs. • Fixed dose combinations (FDCs) have advantages such as reduced preservative exposure, wash out effects and drug interactions. • The non inferiority design of studies comparing FDCs with individual components might limit the evidence. • Cost effectiveness studies differ greatly in methodology and in selected outcomes measures, making interdrug comparison difficult. and travoprost activate the FP receptor. FP activation alters second messenger signaling, stimulating intracellular production of pro-metalloproteinase. These convert to metalloproteinase outside the cell, and degrade collagen fibres, making the ciliary extracellular matrix more porous and facilitating passage of aqueous. Bimatoprost could act through a variant of the FP receptor (9) Finally, cholinergic agents like pilocarpine stimulate ciliary muscle contraction, thus stretching and opening the trabecular meshwork (10). This facilitates aqueous passage through the conventional pathway. Cholinergics do not block the effect of PGAs, as might be expected from their respective mechanisms of action (11) Beyond these hypotensive effects, there may be IOP-independent actions for some agents: improvement in ocular hemodynamics by dorzolamide (12), or retinal neuroprotection with brimonidine (13). Further studies are needed to confirm the true added value of these compounds in glaucoma management. Efficacy: Efficacy varies between drugs; it is the amount of IOP reduction from an untreated baseline, expressed as a percentage and/or absolute values, depending on the design and methodology of studies for that particular drug. According to a meta-analysis (14), PGAs are the most powerful hypotensive drugs currently available, reducing IOP as much as 31–33% from baseline. Theoretically, FDCs containing PGA (PGAFDC) should be the most effective two-drug combination, as they bring together an AP reducer plus an AO facilitator. When latanoprost/timolol FDC once daily was compared with dorzolamide/timolol FDC bid there were no statistically significant differences in IOP reduction (15,16). Conversely, travoprost/timolol FDC once daily compared with dorzolamide/timolol bid demonstrated statistical significance favouring the PGAFDC, although the mean IOP differences between both FDCs was less than 1 mmHg (17). Studies comparing the efficacy of the different PGAFDCs, report statistically significant differences, in favour of bimatoprost/timolol FDC for IOP reduction, compared with latanoprost/timolol FDC (18) and travoprost/timolol FDC (19). While these differences are quantitatively small, even small amounts of IOP lowering could be relevant. A measurable direct relationship between IOP reduction and decreased risk of glaucoma progression has been estimated (20, 21). The clinical relevance for visual field preservation remains to be determined through adequately designed studies. Also relevant is the duration of a drug´s hypotensive effect. As monotherapy, PGAs show a sustained IOP reduction lasting at least 24 hours, consistently flattening the day and night IOP curve, superior to BBs or CAIs (22). Non-PGAFDCs, like dorzolamide/timolol FDC bid, have 24 hour IOP control comparable with latanoprost monotherapy daily and better than brimonidine monotherapy tid (23). Glaucoma Now – No3. www.glaucomanow.com Similarly, dorzolamide/timolol FDC bid performed equally to latanoprost/ timolol FDC daily. (24). One study has compared 24 hour-IOP efficacy of two different PGAFDCs. Travoprost/ timolol FDC qd showed statistically significant differences in 24 hour IOP lowering at some individual time points ahead of latanoprost/timolol FDC qd (25). With PGAFDCs, both morning and evening instillation are effective, but evening dosing might yield statistically significant better 24-hour IOP control (25-27). Limitations/additivity: FDCs have advantages and disadvantages. Benefits include: lower risk of a washout effect, less preservative-induced ocular damage and drug interactions, and increased compliance. (28,29) Regarding PGAFDC efficacy, concerns arise when studies are analyzed in depth. A recent meta-analysis (30), which included studies investigating the IOP lowering effect of PGA combined with BB therapy, has reported that differences in efficacy may relate to study design limitations such as the concept of non-inferiority of FDCs compared with the concomitant combination of their separate components as well as different dosing schedules (morning versus evening). Concomitant but separate use of timolol 0.5% bid and latanoprost daily appears to reduce IOP better than the FDC. However, morning dosing with latanoprost/timolol FDC obtained only IOP data up to 8 hours after administration thus underestimating the peak effect of the PGA component. Regarding non-PGAFDC efficacy, analysis of non-inferiority with the same dosing schedules for fixed and non-fixed treatment regimens (31-32), has shown comparable treatment arms for trough and peak effects; however, they evaluated only two time points, before and after drug instillation. A danger with FDCs is the simultaneous use of two of them: all include timolol (33), which would be doubledosed use in this way. A limitation is inability to adjust the concentration or timing of each component to individual patient requirements (34). Switching from timolol 0.5% bid to latanoprost/timolol FDC qd, results in a pooled change of –2.8 mmHg (30), or a range of change from –1.9 to –3.3 mmHg when switching from timolol 0.5% bid to travoprost/timolol FDC qd (35). Clinical equivalence studies estimate that switching from timolol 0.5% bid to dorzolamide/timolol FDC bid (36) or to brimonidine/timolol FDC bid (31) reduces IOP between 4.2 and 5.4 and between 4.4 and 5.3 mmHg respectively. Similarly, brinzolamide/timolol FDC has demonstrated equivalent efficacy to dorzolamide/timolol FDC (37). Recently, a study compared a threedrug, non-PGA non-FDC (timolol 0.5%, dorzolamide 2% and brimonidine 0.2%) with dorzolamide/timolol FDC (38); the multi-drug FDC lowered mean IOP more effectively from baseline throughout the six-month follow-up. Side effects: Several studies have reported a similar safety profile when different FDCs are compared with their separate components (36,31,39,40,41). As all FDCs include timolol, a specific cardiopulmonary history including asthma or bradyarrhythmias must be excluded (42). All PGA-FDCs have a reduced rate and severity of conjunctival hyperemia compared with each of the PGAs used alone (41, 43, 44). Similarly, the incidence of conjunctival allergy-like reaction from AAs, is lower for the brimonidine/ timolol FDC bid than in monotherapy with brimonidine tid (45,46). Over the long term, latanoprost/timolol FDC is safe and effective over five years; more than two third of patients treated with this FDC, did not show increased iris pigmentation.(48) Cost-effectiveness (CE): Some studies have addressed cost issues of glaucoma medical treatment with FDCs. Travoprost monotherapy was compared with a fixed combination of latanoprost/ timolol as first-line therapies for ocular hypertension or glaucoma. (49). The authors estimated a reduction around half of the mean daily costs in favor of travoprost. These results do not support FDCs as a cost-effective first-line therapy, compared with PGA monotherapy. Travoprost/timolol FDC was shown to compare favorably with latanoprost/timolol FDC through an algorithmic approach that converted IOP data into visual field progression (50). Two European studies have analyzed the efficacy and cost implications comparing the three PGA-FDCs (51) with two non-PGA-FDCs (52). The authors reported brimonidine/timolol FDC bid Glaucoma Now – No3. www.glaucomanow.com to be more cost-effective than dorzolamide/timolol bid, and bimatoprost/ timolol FDC the most effective and least costly PGA-FDC in most of the evaluated countries. However, CE analyses of glaucoma management has limitations: some patient concerns such as life expectancy or disease stage, outcome measures selected, as well as differences in design and methodology. Such factors significantly influence results. BIBLIOGRAPHY 1. Fixed combination drug preparations. In: Terminology and guidelines for glaucoma. 3rd edition. Ed Dogma, Savona,Italy. 2008; 141–143. 2. Ritch R, Shields MB, and Krupin T. Adrenergic and Dopaminergic drugs in glaucoma. In: The Glaucomas (2nd ed.),edited by Ritch R, Shields MB, and Krupin T. St. Louis, MO: Mosby, 1996, p. 1417. 3.Shahidullah M, Wilson WS, Yap M, To CH. Effects of ion transport and channel–blocking drugs on aqueous humor formation in isolated bovine eye.Invest Ophthalmol Vis Sci. 2003 Mar;44(3):1185–91. 4. Mc Laughlin 2001: McLaughlin, C.W., Peart, D., Purves, R.D., Carre, D.A., Peterson–Yantorno, K., Mitchell, C.H., Macknight, A.D., Civan, M.M. Timolol may inhibit aqueous humor secretion by cAMP–independent action on ciliary epithelial cells. American Journal of Physiology – Cell Physiology 2001 281:C865–75 5. Toris CB, Gleason ML, Camras CB, Yablonski ME. Effects of brimonidine on aqueous humor dynamics in human eyes. Arch Ophthalmol. 1995 Dec;113(12):1514–7 6. Mincione F, Scozzafava A, Supuran CT. The development of topically acting carbonic anhydrase inhibitors as antiglaucoma agents. Curr Pharm Des. 2008;14(7):649–54. 7. Wu Q, Delamere NA, Pierce W Jr. Membrane– associated carbonic anhydrase in cultured rabbit no pigmented ciliary epithelium. Invest Ophthalmol Vis Sci. 1997;38:2093–2102. 8.Schachtschabel U; Lindsey JD.; Weinreb RN. The mechanism of action of prostaglandins on uveoscleral outflow. Current Opinion in Ophthalmology: April 2000 – Volume 11 – Issue 2 – pp 112–115. 9. Dong CJ, Guo Y, Agey P, Wheeler L, Hare WA. Alpha2 adrenergic modulation of NMDA receptor function as a major mechanism of RGC protection in experimental glaucoma and retinal excitotoxicity. Invest Ophthalmol Vis Sci. 2008 Oct;49(10):4515–22 10.Ritch R, Shields MB, and Krupin T. Nervous system and intraocular pressure. In: The Glaucomas (2nd ed.),edited by Ritch R, Shields MB, and Krupin T. St. Louis, MO: Mosby, 1996, p. 369. 11.Toris CB, Alm A, Camras CB.Latanoprost and cholinergic agonists in combination. Surv Ophthalmol. 2002 Aug;47 Suppl 1:S141–7. 12.Martínez A, Sánchez–Salorio M.A comparison of the long–term effects of dorzolamide 2% and brinzolamide 1%, each added to timolol 0.5%, on retrobulbar hemodynamics and intraocular pressure in open–angle glaucoma patients. J Ocul Pharmacol Ther. 2009 Jun;25(3):239–48. 13.Saylor M, McLoon LK, Harrison AR, Lee MS.Experimental and clinical evidence for brimonidine as an optic nerve and retinal neuroprotec- 3 tive agent: an evidence–based review. Arch Ophthalmol. 2009 Apr;127(4):402–6. individual components. Ophthalmology. 2006 Jan;113(1):70–6. Epub 2005 Nov 2. 14.van der Valk R, Webers CA, Schouten JS, Zeegers MP, Hendrikse F, Prins MH. Intraocular pressure–lowering effects of all commonly used glaucoma drugs: a meta–analysis of randomized clinical trials.Ophthalmology. 2005 Jul;112(7):1177–85. 27.Konstas AG, Holló G, Mikropoulos D, Tsironi S, Haidich AB, Embeslidis T, Georgiadou I, Irkec M, Melamed S.Twenty–four–hour intraocular pressure control with bimatoprost and the bimatoprost/timolol fixed combination administered in the morning, or evening in exfoliative glaucoma. Br J Ophthalmol. 2010 Feb;94(2):209–13. 15.Miglior S, Grunden JW, Kwok K;Xalacom/Cosopt European Study Group. Efficacy and safety of fixed combinations of latanoprost/timolol and dorzolamide/timolol in open–angle glaucoma or ocular hypertension. Eye 2010 Jul;24(7):1234–42. 16.Cvenkel B, Stewart JA, Nelson LA, Stewart WC. Dorzolamide/timolol fixed combination versus latanoprost/timolol fixed combination in patients with primary open–angle glaucoma or ocular hypertension. Curr Eye Res. 2008 Feb;33(2):163–8. 28.Crichton ACS, Kee C, Craven R, Galloway P, Goñi FJ, Graham SL, Hartleben C, Katz LJ, Motolko M, Nixon D, Susanna R, Thygesen J A global view on fixed–combination therapy for glaucoma. Ophthalmology Times. 2007 march; 3–10 29.Tabet R, Stewart WC, Feldman R, Konstas AG. A review of additivity to prostaglandin analogs: fixed and unfixed combinations. Surv Ophthalmol. 2008 Nov;53 Suppl1:S85–92. 17.Teus MA, Miglior S, Laganovska G, Volksone L, Romanowska–Dixon B, Gos R, Holló G. Efficacy and safety of travoprost/timolol vs dorzolamide/timolol in patients with open–angle glaucoma or ocular hypertension. Clin Ophthalmol. 2009;3:629–36. Epub 2009 Nov 16. 30.Webers CA, Beckers HJ, Zeegers MP, Nuijts RM, Hendrikse F, Schouten JS. The Intraocular Pressure–Lowering Effect of Prostaglandin Analogs Combined with Topical beta–Blocker Therapy A Systematic Review and Meta–analysis. Ophthalmology. 2010 Jul 8. [Epub ahead of print] 18.Martinez A, Sanchez M. Bimatoprost/timolol fixed combination vs latanoprost/timolol fixed combination in open–angle glaucoma patients. Eye 2009;23(4):810–818 31.Goñi FJ; Brimonidine/Timolol Fixed Combination Study Group.12–week study comparing the fixed combination of brimonidine and timolol with concomitant use of the individual components in patients with glaucoma and ocular hypertension. Eur J Ophthalmol. 2005 Sep–Oct;15(5):581–90 19.Centofanti M, Oddone F, Gandolfi S, Hommer A, Boehm A, Tanga L, Sangermani, C, Sportelli V, Haustein M, Manni G, Rossetti L. Comparison of Travoprost and Bimatoprost plus Timolol Fixed Combinations in Open–Angle Glaucoma Patients Previously Treated with Latanoprost plus Timolol Fixed Combination. Am J Ophthalmol. 2010 Aug 3. [Epub ahead of print] 32.Francis BA, Du LT, Berke S, Ehrenhaus M, Minckler DS; Cosopt Study Group. Comparing the fixed combination dorzolamide–timolol (Cosopt) to concomitant administration of 2% dorzolamide (Trusopt) and 0.5% timolol – a randomized controlled trial and a replacement study. J Clin Pharm Ther. 2004 Aug;29(4):375–80. 20.Leske MC, Heijl A, Hyman L, Bengtsson B, Dong L, Yang Z; EMGT Group.Predictors of long– term progression in the early manifest glaucoma trial. Ophthalmology. 2007 Nov;114(11):1965–72. Epub 2007 Jul 12. 34.Khouri AS, Realini T, Fechtner RD.Use of fixed–dose combination drugs for the treatment of glaucoma. Drugs Aging. 2007;24(12):1007–16. 21.Peeters A, Webers CA, Prins MH, Zeegers MP, Hendrikse F, Schouten JS.Quantifying the effect of intraocular pressure reduction on the occurrence of glaucoma. Acta Ophthalmol. 2010 Feb;88(1):5–11. Epub 2009 Apr 27. 35.Barnebey HS, Orengo–Nania S, Flowers BE, Samples J, Mallick S, Landry TA, Bergamini MV. The safety and efficacy of travoprost 0.004%/ timolol 0.5% fixed combination ophthalmic solution. Am J Ophthalmol. 2005 Jul;140(1):1–7. 22.Orzalesi N, Rossetti L, Invernizzi T, Bottoli A, Autelitano A. Effect of timolol, latanoprost, and dorzolamide on circadian IOP in glaucoma or ocular hypertension. Invest Ophthalmol Vis Sci. 2000 Aug;41(9):2566–73. 36.Hutzelmann J, Owens S, Shedden A, Adamsons I, Vargas E. Comparison of the safety and efficacy of the fixed combination of dorzolamide/ timolol and the concomitant administration of dorzolamide and timolol: a clinical equivalence study. International Clinical Equivalence Study Group. Br J Ophthalmol. 1998 Nov;82(11):1249–53. 23.Orzalesi N, Rossetti L, Bottoli A, Fumagalli E, Fogagnolo P..The effect of latanoprost, brimonidine, and a fixed combination of timolol and dorzolamide on circadian intraocular pressure in patients with glaucoma or ocular hypertension. Arch Ophthalmol. 2003 Apr;121(4):453–7. 24.Konstas AG, Kozobolis VP, Lallos N, Christodoulakis E, Stewart JA, Stewart WC.Daytime diurnal curve comparison between the fixed combinations of latanoprost 0.005%/timolol maleate 0.5% and dorzolamide 2%/timolol maleate 0.5%. Eye (Lond). 2004 Dec;18(12):1264–9. 25.Konstas AG, Mikropoulos DG, Embeslidis TA, Dimopoulos AT, Papanastasiou A, Haidich AB, Stewart WC. 24–h Intraocular pressure control with evening–dosed travoprost/timolol, compared with latanoprost/timolol, fixed combinations in exfoliative glaucoma. Eye (Lond). 2010 Jul 23. [Epub ahead of print] 26.Diestelhorst M, Larsson LI; European–Canadian Latanoprost Fixed Combination Study Group. A 12–week, randomized, double–masked, multicenter study of the fixed combination of latanoprost and timolol in the evening versus the 4 33.EGS 37.Manni G, Denis P, Chew P, Sharpe ED, Orengo–Nania S, Coote MA, Laganovska G, Volksone L, Zeyen T, Filatori I, James J, Aung T.The safety and efficacy of brinzolamide 1%/timolol 0.5% fixed combination versus dorzolamide 2%/timolol 0.5% in patients with open–angle glaucoma or ocular hypertension. J Glaucoma. 2009 Apr– May;18(4):293–300. 38.Baiza–Durán LM, Alvarez–Delgado J, Contreras–Rubio AY, Medrano–Palafox J, De Luca– Brown A, Casab–Rueda H, Cortés–Gastélum MA, Garcidueñas–Mejía MJ, Gómez–Bastar P, Gil–Carrasco F, Hartleben–Matkin C, Jiménez– Román J, Moreno–Marín ML, Paczka–Zapata JA, Velasco–Gallegos G, Vergara–Sinta M.The efficacy and safety of two fixed combinations: timolol–dorzolamide–brimonidine versus timolol–dorzolamide. A prospective, randomized, double–masked, multi–center, 6–month clinical trial. Ann Ophthalmol (Skokie). 2009 Fall–Winter;41(3–4):174–8. 39.Higginbotham EJ, Diestelhorst M, Pfeiffer N, Rouland JF, Alm A. The efficacy and safety of un- fixed and fixed combinations of latanoprost and other antiglaucoma medications. Surv Ophthalmol. 2002 Aug;47 Suppl 1:S133–40. 40.Barnebey HS, Orengo–Nania S, Flowers BE, Samples J, Mallick S, Landry TA, Bergamini MVAm J Ophthalmol. The safety and efficacy of travoprost 0.004%/timolol 0.5% fixed combination ophthalmic solution. Am J Ophthalmol 2005 Jul;140(1):1–7. 41.Hommer A; Ganfort Investigators Group I.A double–masked, randomized, parallel comparison of a fixed combination of bimatoprost 0.03%/ timolol 0.5% with non–fixed combination use in patients with glaucoma or ocular hypertension. Eur J Ophthalmol. 2007 Jan–Feb;17(1):53–62. 42.Novack GD, O’Donnell MJ, Molloy DW. New glaucoma medications in the geriatric population: efficacy and safety. J Am Geriatr Soc. 2002 May;50(5):956–62. 43.Vinuesa–Silva JM, Vinuesa–Silva I, Pinazo– Durán MD, Soto–Alvarez J, Delgado–Ortega L, Díaz–Cerezo S.Development of conjunctival hyperemia with the use of a fixed combination of latanoprost/timolol: systematic review and meta– analysis of clinical trials. Arch Soc Esp Oftalmol. 2009 Apr;84(4):199–207. 44.Gross RL, Sullivan EK, Wells DT, Mallick S, Landry TA, Bergamini MV.Pooled results of two randomized clinical trials comparing the efficacy and safety of travoprost 0.004%/timolol 0.5% in fixed combination versus concomitant travoprost 0.004% and timolol 0.5%.Clin Ophthalmol. 2007 Sep;1(3):317–22. 45.Sherwood MB, Craven ER, Chou C, DuBiner HB, Batoosingh AL, Schiffman RM, Whitcup SM. Twice–daily 0.2% brimonidine–0.5% timolol fixed–combination therapy vs monotherapy with timolol or brimonidine in patients with glaucoma or ocular hypertension: a 12–month randomized trial. Arch Ophthalmol. 2006 Sep;124(9):1230–8. 46.Motolko MA. Comparison of allergy rates in glaucoma patients receiving brimonidine 0.2% monotherapy versus fixed–combination brimonidine 0.2%–timolol 0.5% therapy. Curr Med Res Opin. 2008 Sep;24(9):2663–7. 47.Alvarado JA. Reduced ocular allergy with fixed–combination 0.2% brimonidine–0.5% timolol. Arch Ophthalmol. 2007 May;125(5):717 48.Alm A, Grunden JW, Kwok KKFive–year, Multicenter Safety Study of Fixed–combination Latanoprost/Timolol (Xalacom) for Open–angle Glaucoma and Ocular Hypertension. J Glaucoma. 2010 May 29. [Epub ahead of print] 49.De Natale R, Lafuma A, Berdeaux G.Cost effectiveness of travoprost versus a fixed combination of latanoprost/timolol in patients with ocular hypertension or glaucoma: analysis based on the UK general practitioner research database. Clin Drug Investig. 2009;29(2):111–20 50.Schmier JK, Halpern MT, Covert DW, Robin AL. Travoprost versus latanoprost combinations in glaucoma: economic evaluation based on visual field deficit progression. Curr Med Res Opin. 2006 Sep;22(9):1737–43. 51.Hommer A, Wickstrøm J, Friis MM, Steeds C, Thygesen J, Ferreras A, Gouws P, Buchholz P. A cost–effectiveness analysis of fixed–combination therapies in patients with open–angle glaucoma: a European perspective. Curr Med Res Opin. 2008 Apr;24(4):1057–63. 52.Hommer A, Thygesen J, Ferreras A, Wickstrom J, Friis MM, Buchholz P, Walt JG. A European perspective on costs and cost effectiveness of ophthalmic combinations in the treatment of open–angle glaucoma. Eur J Ophthalmol. 2008 Sep–Oct;18(5):778–86. Glaucoma Now – No3. www.glaucomanow.com What’s New Mechanisms of Action of Fixed Combinations Stephen J Best FRANZCO Consultant Ophthalmologist at the Auckland District Health Board. He is also Senior Clinical Lecturer at the Ophthalmology Department of the University of Auckland, New Zealand. Core Concepts • Medications from the same pharmacological group should not be used in combination • Therapeutic agents should act synergistically e.g. a drug that increases uveoscleral outflow should be combined with one that decreases aqueous inflow • When initiating a combination therapy, attention needs to be given to the patient’s medical history • Prostaglandin monotherapies are considered best clinical practice and should be the basis for combination therapies • Fixed combinations may have the benefit of increased patient compliance and less exposure to preservative, potentially improving patients’ quality of life Introduction The major risk factor for glaucoma is elevated intraocular pressure. The only proven effective strategy for treating glaucoma is reducing intraocular pressure. In most clinical situations, significant reduction of intraocular pressure is achieved by the application of topical medication. The ideal treatment would be a single agent that is well tolerated, administered once daily with excellent efficacy. However in some routine cases adequate reduction of the intraocular pressure towards the desired target pressure can only be achieved with the use of more than one agent. The options of combination therapy are discussed centred on a typical glaucoma case history scenario. Case Study: JT, a 56 year old Caucasian with no family history of glaucoma, was referred by his optometrist. He was sys- temically well on no medications. His unaided visual acuity was 6/6 OU. His intra-ocular pressures (IOP) were 32 mmHg OD and 28 mmHg OS (CCT 554nm and 557nm) and he had open angles on gonioscopy without pigment dispersion or pseudo-exfoliation. The right optic disc had an inferior focal thinning of the neuro-retinal rim, and there was corresponding superior arcuate visual field loss. The diagnosis was primary open angle glaucoma. A target intraocular pressure of 14–16 mmHg was suggested. Best clinical practice is to use a topical prostaglandin analogue as initial therapy. These agents are used once daily, and have minimal side effects (initial hyperemia, eyelashes longer, darker, thicker, and possible iris darkening long term.) Daily treatment, often at night-time is presumed to improve compliance, as well reduce exposure to topical preservatives. A therapeutic trial of Gtt latanoprost at night time (1 drop) to the right eye was initiated. 6 weeks later the respective IOP meaurements were 26 mmHg OD and 27 mmHg OS. To reach target IOP, medical therapy needed to be changed: what are the options available? To switch within the same class of ocular hypotensive (prostaglandin) or to add an additional agent from another class? We switched “within same class of drug” to of Gtt brimatoprost, (1 drop) at bedtime only for the right eye. 8 weeks later IOP were 22 OD and 26 OS. As target IOP had not yet been reached, additional therapy is required. The clinical photos of the Humphrey Visual fields are depicted on page 6 (figure 1) and 7 (figure 2). The optic disc photographs are shown on page 8 (figure 3). This case history illustrates a common scenario in medical treatment of glaucoma: one hypotensive agent results in insufficient IOP lowering. While there are several options available, the treat- Glaucoma Now – No3. www.glaucomanow.com ing physician must tailor treatment to the individual accounting for multiple factors, including concurrent systemic medical conditions. When more than one topical ocular hypotensive agent is commonly required in glaucoma management, what are the options? Two agents can be combined together into one solution (“Fixed Combination”), or the two agents can be instilled simultaneously but separately (“Unfixed Combination”). All currently available fixed combination medications use timolol as the second agent Timolol + DorzolamideCosopt® MSD Timolol + Latanoprost Xalacom ® Pfizer Timolol + Travoprost Duotrav® Alcon Timolol + Bimatoprost Ganfort® Allergan Timolol + Brimonidine Combigan ® Allergan Timolol + Pilocarpine Only available in a few countries Add-on topical therapies fall into three categories: a) Beta blockers; b) Alpha agonists; c) Carbonic anhydrase inhibitors. Each of these medications has its own potential side effects and precautions; in particular topical beta blockers may exacerbate asthma/reactive airways disease, heart disease, and have other central nervous system side effects. Attention must be given to the patient’s past medical history. Topical alpha analogues are contraindicated in children, and their use may be limited by local allergic reactions. Topical carbonic anhydrase inhibitors have little systemic side effects (occasional after-taste), but may cause local discomfort. When a medication is added to an ongoing regimen, there are multiple options. The following overview lists advantages and disadvantages of fixed combination therapy with un-fixed combined therapy1: 5 Major advantages 1) Presumed improved compliance with reduced total daily instillation frequency; 2) Reduced exposure to topical preservatives; 3) Avoidance of the need to wait at least five minutes between drops from different bottles; 4) Reduced local side effects (especially hyperemia) when timolol is combined with brimonidine and any of the prostaglandin agents; 5) All this contributes to improved quality of life, an important often neglected factor in the treatment of glaucoma patients Major disadvantages 1) No avoidance of possible systemic and local side effects of component agents; 2) No avoidance of possible tachyphylaxis (especially with topical beta blockers); 3) The additive hypotensive effect may not meet target IOP; 4) The two agents might be slightly more effective if used in an unfixed combination (little evidence). Implementing a combination therapy General Principles Medications from the same pharmacological group should not be used in combination: There is a variably additive effect across all pharmacological groups of ocular hypotensive agents, which requires any combination to be tested for each patient. No patient should use a fixed combination unless they have been shown to have inadequate IOP reduction from each agent alone, and to have an additive effect from both together. Adherence Even though we cannot measure accurately true compliance in everyday treatment situations as opposed to carefully crafted randomized double masked trials, we suspect it to be reduced. Indirect measurements of drug purchased from the pharmacy demonstrate that even with single daily dosage regimen the adherence was found to be as low as 50%2 . These findings were confirmed by another study group that additionally found adherence further decreased if 2 medications were applied (32%)3. 6 Table 2.2 of the SEAGIG guidelines outlines the mechanisms of action of the different drug classes (reproduced with permission)5 Mechanism of action Increase in aqueous outflow Decrease in aqueous inflow Drug class PGAs Increase uveoscheral outflow Cholinergics Increase trabecular outflow β-Blockers α2 -adrenergic agonists CAIs Side Effects Fixed combination therapy brimonidine + timolol appears to have a reduced in- Preparations Latanoprost Travoprost Bimatoprost Unoprostone Pilocarpine Carbachol β1-Non-selective Timolol Levoburolol Carteolol β1-Selective Betaxolol Brimodininen Apracloridine Systemic Acetazolamide Methazolamide Dichlorphenamide Topical Dorzolamide Brinzolamide cidence of allergic reaction compared with unfixed combined therapy. Initial reports of this phenomena were anec- Figure 1: Case study – Humphrey Visual Field Test 24-2, right eye. Central 24-2 Threshold Test Fixation Monitor: Gaze/Bind Spot Stimulus: II, White Pupil Diameter: 7.9 mm Date:03-29-201 Fixation Target: Central Background: 31.5 ASB Visual Acuity: 20/25 Time: 9:17 AM Fixation Losses: 2/16 Strategy: SITA-Standard RX: +5.50 DS DC X Age: 59 False POS Errors: 0 % False NEG Errors: 3 % Test Duration: 05:50 Fovea: OFF GHT Outside normal limits MD –4.25 dB P <0.5 % PSD 6.37 dB P <0.5 % Total Pattern Deviation Deviation Glaucoma Now – No3. www.glaucomanow.com Figure 2: Case study – Humphrey Visual Field Test 24-2, left eye. Central 24-2 Threshold Test Fixation Monitor: Gaze/Bind Spot Stimulus: II, White Pupil Diameter: 4.1 mm Date:03-29-201 Fixation Target: Central Background: 31.5 ASB Visual Acuity: 20/25 Time: 9:24 AM Fixation Losses: 5/14 xx Strategy: SITA-Standard RX: +5.50 DS DC X Age: 59 False POS Errors: 0 % False NEG Errors: 0 % Test Duration: 04:51 Fovea: OFF and reflect differing methodologies for the studies..1 Having considered all above points the case history continued as follows: This patient was keen to keep therapy simple, so after further discussion treatment with a fixed combination prostaglandin analogue + timolol with evening dosing was prescribed. After instilling Gtt travoprost/timolol fixed combination ( 1 drop ) at night in the right eye for 8 weeks, IOP were right 17 mmHg on the right and 21 mmHg on the left. Subsequently both eyes were treated with the same medication. What is the best adjunctive therapy? ***Low Test Reliability*** GHT Within normal limits MD –0.73 dB PSD 1.53 dB Total Pattern Deviation Deviation dotal, but have been confirmed in 2008 by Motolko.4 Similarly the fixed prostaglandin + timolol preparations also appear to have a reduced incidence of hyperaemia.1 Theories of best treatment options Perhaps the unfixed combination of a prostaglandin analogue at night-time (to reduce nocturnal IOP) and day time agents that reduce aqueous production, might control IOP more effectively. However this increases the complexity of drug dosing with the risk of reduced compliance. Time of administration: Studies suggest that night-time dosing of fixed combinations of PGA is more effective than morning dosing for lowering IOP. However this effect night reflect the time of measurement of IOP Within the EGS 2008 guidelines, the table on page 139 (reproduced with permission) outlines the additive effects of drug combinations.6 Current Drug α2 agonists β-blockers Topical CAIs Cholinergic Prostaglandin/ Prostamides Drug Combinations- Additive Effect Additional Drug α2 agonists β-blockers Topical Cholinergic CAIs + + + + + + + + + + + + + + + Glaucoma Now – No3. www.glaucomanow.com +/– Prostaglandin/ Prostamide + + + +/– Additive medical decisions must be individualized to minimize side effects and maximize compliance. When one topical medication is combined with a second, the rationale underpinning the choice of drugs is based on the knowledge of the mechanism of actions. It would make sense to combine a drug, that increases aqueous outflow by increased uveoscleral outflow, (prostaglandin analogue) with a second drug that decreases aqueous inflow (a beta Blocker). Drugs of the same class would not be expected to have an additive or synergistic effect when used as a combined preparation. Another alternative is the combination of two drugs that both decrease aqueous inflow; the two available options representing this therapeutic approach combines a beta blocker either an alpha adrenergic agonist (Combigan), or with a carbonic anhydrase inhibitor (Cosopt). Conclusion The use of a typical glaucoma case history scenario provided the framework for discussion of the available options of combination therapy for reduction of intraocular pressure. One of the main principles is the concomitant use of therapeutic agents that act synergistically to reduce intraocular pressure. There are potential benefits from combination therapy that need to be balanced by the convenience of single agents as opposed to multiple agents, and must be tailored to the individual patient circumstances in order to achieve the desired target intraocular pressure. 7 Figure 3: Case study – Optic disc photographs (OD above, OS below). References 1 Tabet, R et al : A review of additivity of Prostaglandin Analogues : Fixed and unfixed combinations. Survey of Ophthalmology; 53 Supplement 1, Nov 2008. 2 Rait, LJ&Adena,AA Persistency rates for prostaglandin and other hypotensive eyedrops:population-based study using pharmacy claims data. CEO 2007; 35: 602–611. 3 Patel SC, Spaeth GL. Compliance in patients prescribed eye drops for glaucoma. Ophthalmic Surg 1995; 26: 234–236. 4 Motolko M, Curr Med Res Opin 2008; 24(9): 2663–2667. 5South East Asia Glaucoma Interest Group: Asia Pacific Glaucoma Guidelines. Second Edition, 2008. 6 European Glaucoma Society: Terminology and Guidelines for Glaucoma. Second Edition 2003. 8 Glaucoma Now – No3. www.glaucomanow.com Clinical Issues: Fixed Combinations in Treatment Algorithms and Guidelines Alessandro Bagnis1, Marina Papadia1, Carlo Enrico Traverso1 1 Centro di Ricerca Clinica e Laboratorio per il Glaucoma e la Cornea, Clinica Oculistica Di.N.O.G., University of Genova, Genova, Italy. Core Concepts • Glaucoma treatment should be started with a topical monotherapy • If the first choice monotherapy is not effective or tolerable, a switch to a different monotherapy is to be considered • If the first choice monotherapy is effective, but does not yield target IOP, an adjunctive therapy is to be considered • When two or more actives are neccessary a fixed combination should be considered. • Fixed combinations may offer several advantages, such as improved efficacy and tolerability – through less exposure to preservatives – as well as improved patient compliance and quality of life. There’s a general consensus to start glaucoma medical therapy with one topical intraocular pressure (IOP) lowering medication. If the first choice monotherapy alone is not effective to reduce IOP or is not tolerated, it is preferable to switch to another molecule that is initiated as monotherapy. Adjunctive therapy should be considered whenever a monotherapy does not reach target IOP or the target must be lowered as the disease is progressing (1,2) (Fig.1). Usually fixed-combinations are not ideal as a first choice product, unless an large reduction in IOP is needed quickly. In such cases, fixed-combination drug preparations may have advantages if compared with two separate instillations of the same agents (1) (Fig.1). Improved compliance. Compliance with any given medical therapy in glaucoma, like other chronic diseases, is better when regimens are simple rather than complex (3). In most patients it is not recommended to use more than two drugs in two separate bottles or to add more than one single drug to a fixed-combination. Besides complexity, the higher costs from more bottles seem to promote noncompliance and reduce persistence (4). Reduced daily amount of exposure to preservatives and side effects: There may be a direct correlation between the presence of preservatives and the surface symptoms provoked by anti-glaucoma therapy (5); reducing such exposure could improve the patient’s comfort and thus compliance. Long-term use of topical drugs may be detrimental as a dose- and time-dependent consequence to benzalkonium chloride exposure (5). Such changes may reduce the success rate of subsequent filtration surgery (6). Although no definitive data exist, at least some of the currently available fixed combination have shown a better safety profile and tolerability when compared with the same molecules used separately (1,7). Possibly more efficacy. Several openlabel replacement studies have suggested an additional IOP lowering effect when switching from dorzolamide and a betablocker to the fixed-combination dorzolamide/timolol, but no definitive data is available (7). Increased compliance and elimination of the dilution effect if drops are instilled from different bottles without sufficient time between, could explain such fixed-combination benefit. A substantial proportion of patients on a multiple drops regimen wait less than 3 minutes before instilling the second medication. The dilution effect occurs when patients consecutively instill multiple eye drops too closely, so that the first drop is washed away by the second drop before the first can achieve maximal ocular penetration and thus efficacy (8) Possible cost savings. The cost of a fixed combination is not necessarily less 1st CHOICE MONOTHERAPY NOT effective and/or not tolerated Effective, well tolerated Change monotherapy TARGET IOP NOT REACHED Add a 2nd drug Add a 2nd drug in a FIXED COMBINATION Figure 1. Treatment algorithm of OAG. Fixed combinations are a viable option when monotherapy fails in reaching the target IOP (1,2). Glaucoma Now – No3. www.glaucomanow.com 9 than the cost of the single components. However, fixed combinations reduce the number of purchased bottles, which may reduce costs for patients whose prescription drug coverage requires a co-payment for each prescription filled. Quality of life. The goal of glaucoma treatment is to maintain the patient’s visual function and related quality of life (1). Besides the functional loss and having the diagnosis of a potentially blinding disease, other factors alone or in combination may affect patients’ quality of life: inconvenience of the treatment, side effects and therapy costs. By reducing drops and bottles without losing efficacy, fixed combinations represent an important tool in order to maintain a good quality of life, which is one of the most important aspects for patients. Conclusions When two or more active molecules are necessary to obtain an adequate IOP, fixed-dose combination eye drops may offer advantages for patients, while maintaining at least the same effect on IOP than separate instillation of the same two products. Reducing the number of daily drops may improve compliance and quality of life, save costs and reduce detrimental effects to the ocular surface. References 1. Treatment principles and options. In: European Glaucoma Society, Terminology and Guidelines for Glaucoma (3rd ed.), DOGMA Srl, Savona, Italy; 2008. p. 117–169 2. Medical treatment. In: South East Asia Glaucoma Interest Group, Asia Pacific Glaucoma Guidelines (2nd ed.), SEAGIG, Sydney, Australia; 2008. p. 25–28. 3. Olthoff CM, Schouten JS, Van de Brne BW, Webers CA. Non compliance with ocular hypothensive treatment in patients with glaucoma or ocular hypertension: an evidence-based review. Ophthalmology. 2005;112(6):953–961. 4.Soumerai SB, Pierre-Jacques M, Zhang F, et al. Cost-related medication nonadherence among elderly and disabled Medicare beneficiaries: a national survey 1 year before the Medicare drug benefit. Arch Intern Med. 2006;166:1829–35. 5. Baudouin C, Labbé A, Liang H, Pauly A, Brignole-Baudouin F. Preservatives in eyedrops: the good, the bad and the ugly. Prog Retin Eye Res. 2010;29(4):312–34. Epub 2010 Mar 17. 6. Baudouin C . Side effects of antiglaucomatous drugs on the ocular surface. Curr Opin Ophthalmol 1996;7(2):80–6 7. Higginbothan EJ. Considerations in glaucoma therapy: fixed combinations vs their component medications. Clin Ophthalmol. 2010;4:1–9. 8.Sleath B, Robin AL, Covert D, et al. Patient-reported behavior and problems in using glaucoma medications. Ophthalmology. 2006;113:431–436. Practical Tips: Fixed Combinations and Patient’s Perspective Vital P. Costa, MD Director, Glaucoma Service, University of Campinas, Brazil, Professor of Ophthalmology, University of Campinas, Brazil Core concepts • Glaucoma is an asymptomatic disease and motivating patients to adhere to treatment is a well known issue • Studies have shown that only about 50% of patients adhere to monotherapy and even less patients adhere to a therapy scheme including to 2 medications; as a consequence this has a negative effect on drug efficacy and treatment success • In combination therapy use of multiple agents can lead to washout effects and increase exposure to toxic effects of preservatives • Use of fixed combinations decreases such issues and ultimately have a positive effect on patients’ quality of life. 10 Glaucoma is a chronic, asymptomatic disease that requires long-term, potentially costly treatment. Medical treatment often causes side effects, with no subjective improvement in visual function. Unsurprisingly, non-adherence is so frequent among our patients. One additional factor increasing non-adherence rates is the frequent need for more than one medication to control their intraocular pressure (IOP). Among the patients on medications in the Ocular Hypertension Treatment Study, 40 % required 2 or more medications to obtain a mean IOP reduction of 20 %1. When IOP reduction is greater, such as in the Collaborative Initial Glaucoma Treatment Study, where patients achieved a mean IOP reduction of 40 %, 75 % of those in the medical treatment group were using 2 or more agents2. One of the most important factors associated with non-adherence is the medical regimen. Patel & Spaeth3 demonstrated that while 49 % of patients using one medication for the treatment of glaucoma were compliant, only 32 % of those using two medications were. The more medications we prescribe for one patient, the higher the chances of nonadherence. Using multiple agents can also lead to an undesirable “washout effect”. Although we ask patients to wait at least 5 minutes between dosing different medications, few of them actually do. If a patient waits only 30 seconds between dosing medications, up to 45 % of the first medication can be washed out by the second4. The time interval between doses has also been found to affect IOP reduction significantly. In a small study, the mean IOP decreases were 17.2 % when 2 different topical eye medications were Glaucoma Now – No3. www.glaucomanow.com instilled at the same time, 24.5 % when they were instilled 2 minutes apart, and 27.3 % when the interval between drops was 5 minutes5. Recently, interest has increased concerning ocular surface disease in glaucoma patients on medical treatment. Several medications increase toxic effects to the ocular surface, which may be secondary to eye drop preservatives (especially benzalkonium chloride, BAK)6. In terms of efficacy, most randomized, clinical trials that compared fixed with unfixed combinations showed better IOP control with the latter. While randomized, controlled trials are the best way to assess efficacy and safety of medications, they do not provide insight into the impact on adherence, since all patients are closely monitored and encouraged to use their medications correctly. “Real-world” studies, in which glaucoma patients are switched from unfixed to fixed-combination therapy, demonstrate further reductions in IOP, probably as a consequence of increased adherence to therapy7,8. In conclusion, fixed combinations may increase adherence and improve the patient’s quality of life by decreasing the number of instillations required per day and by reducing the toxic effects induced by preservatives. Finally, they may even improve the IOP reduction compared Problems with multiple mediactions used separately and simultaneously Increased number of instillations per day Fixed combinations Negative impact on quality of life Less negative impact on quality of life Negative impact on adherence and efficacy Less negative impact on adherence and efficacy Ocular surface side-effects (BAK) Reduced ocular surface side-effects Wash-out between drugs No need for wash-out Decreased number of instillations per day with unfixed combinations, especially in non-adherent patients. These benefits have encouraged some ophthalmologists to use fixed combinations as first line therapy. We do not recommend this approach: patients should be started on monotherapy, with other medications being substituted or added in a stepwise fashion as needed to achieve target IOP. Before using a fixed combination, the ophthalmologist needs to confirm the efficacy and safety of each of its constituent compounds for the individual patient. tial Glaucoma Treatment Study comparing initial treatment randomized to medications or surgery. Ophthalmology 2001; 108:1943–53. References 7. Arend K-O, Raber T. Observational study results in glaucoma patients undergoing a regimen replacement to fixed combination travoprost 0.004%/timolol 0.5% in Germany. J Ocular Pharmacol Therapeut. 2008; 24:414-420. 1. Kass MA, Heuer DK, Higginbotham EJ, et al. The Ocular Hypertension Treatment Study: a randomized trial determines that topical ocular hypotensive medication delays or prevents the onset of primary open-angle glaucoma. Arch Ophthalmol. 2002; 120:701–713. 2. Lichter PR, Musch DC, Gillespie BW, Guire KE, Janz NK, Wren PA, Mills RP; CIGTS Study Group. Interim clinical outcomes in the Collaborative Ini- Glaucoma Now – No3. www.glaucomanow.com 3. Patel SC, Spaeth GL. Compliance in patients prescribed eye drops for glaucoma. Ophthalmic Surg. 1995; 26:234–236. 4. Chrai SS, Makoid MC, Eriksen SP, Robinson JR. Drop size and initial dosing frequency problems of topically applied ophthalmic drugs. J Pharm Sci. 1974; 63:333–338. 5. Serle J, Toor A, Fahim M, et al. The effect of varying dosing intervals on the efficacy of intraocular pressure lowering drugs. Invest. Ophthalmol Vis Sci. 2004;45: ARVO E-Abstract 974. 6. Leung EW, Medeiros FA, Weinreb RN. Prevalence of ocular surface disease in glaucoma patients. J Glaucoma 2008;17:350–5. 8. Choudhri S, Wand M, Shields MB. A comparison of dorzolamide-timolol combination versus the concomitant drugs. Am J Ophthalmol. 2000; 130:832–3. 11 CME credits can be obtained via the questions on the website very soon. The process of obtaining CME accreditation for the journal is currently ongoing. STATEMENT OF NEED AND PROGRAM DESCRIPTION Recent months and years have seen significant advances in our understanding of glaucoma. Much has been learned, not only about damage mechanisms and pathogenesis, but also about diagnosis and management. Treatment options – both medical and surgical – continue to expand. This program will review this new knowledge with an emphasis on incorporating recent insights into day-to-day practice. discussed or suggested in this activity should not be used by clinicians without evaluation of their patient’s conditions and possible contraindications or dangers in use, applicable manufacturer’s product information, and comparison with recommendations of other authorities. CONTRIBUTORS • DATE OF ORIGINAL RELEASE October 2010. Approved for a period of 12 months DISCLAIMER Participants have an implied responsibility to use newly acquired information to enhance patient outcomes and professional development. The information presented in this activity is not meant to serve as a guideline for patient care. Any procedures, medications, or other courses of diagnosis or treatment 12 • • Francisco Goñi is co-director of Barcelona Glaucoma Centre-IOBUSP. He is also chief of the Integrated Department of Ophthalmology at the Hospital of Granollers, Mollet and Sant Celoni. Mercè Guarro is his specialist co-worker. Stephen Best is Consultant Ophthalmologist at the Auckland District Health Board. He is also Senior Clinical Lecturer at the Ophthalmology Department of the University of Auckland, New Zealand. Carlo Enrico Traverso is Professor of Ophthalmology at the Centro di Ricerca Clinica e Laboratorio per il Glaucoma e la Cornea, Clinica Oculista Di.N.O.G at the University of Genova, Genova, Italy. Alessandro Bagnis and Marina Papadia are his specialist co-workers. • Vital P. Costa is Director of Glaucoma Services and Professor of Ophthalmology at the University of Campinas, Brazil DISCLOSURE STATEMENT EDITORIAL BOARD Clive Migdal serves on the Faculty and Advisory Boards of the following companies: Alcon, Allergan, Merck, Pfizer and Santen. Ivan Goldberg serves on the Faculty and Advisory Boards of the following companies: Alcon, Allergan, Merck and Pfizer. Remo Susanna serves on the Faculty and Advisory Boards of the following companies: Alcon, Allergan, Merck and Pfizer. Glaucoma Now – No3. www.glaucomanow.com