Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Infection control wikipedia , lookup
Kawasaki disease wikipedia , lookup
Acute pancreatitis wikipedia , lookup
Gastroenteritis wikipedia , lookup
Traveler's diarrhea wikipedia , lookup
Rheumatic fever wikipedia , lookup
Neonatal infection wikipedia , lookup
Hepatitis B wikipedia , lookup
Immunosuppressive drug wikipedia , lookup
Sjögren syndrome wikipedia , lookup
Schistosomiasis wikipedia , lookup
Hospital-acquired infection wikipedia , lookup
Urinary tract infection wikipedia , lookup
Management of multiple sclerosis wikipedia , lookup
Childhood immunizations in the United States wikipedia , lookup
Coccidioidomycosis wikipedia , lookup
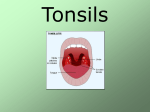
Diseases of the Oropharynx By 3D group 2 Melissa Ann Velasquez Sarah Velasquez Abelaine Venida Jennifer Jeanne Vicera Margaret Elaine Villamayor Paolo Villanueva Diogenes Villareal Cherisse Vinoya Emmerson Vista Eunice Wong •John Andrew Yam •Marie Lourdes Ynson •Mary Liezl Yu •Dianne Joyce Yusi •Aileen Zagala •Camille Zayco •Kaye Pamela Zozobrado •Darwin Salonga Anatomy of the Oropharynx Examination of the Oral Cavity Acute Pharyngitis Etiology and Pathology Varies depending on the causative organism Exudate = serous thicker or mucoid dry and may adhere to the pharyngeal wall. Hyperemia = pharyngeal wall blood vessels become dilated. Small white, yellow or gray plugs form in the follicles or lymphoid tissue. Lateral pharyngitis = lateral wall involvement - lymphoid follicles or plaques on the posterior pharyngeal wall, or localized more laterally, are inflamed and swollen. Can be due to a viral causative agent In acute pharyngitis associated with adenopathy in the absence of follicular pharyngitis membrane formation Vesicle formation on the mucous membrane, ex. Herpes. Signs and symptoms Onset Dryness and scratchiness of the throat (+) malaise and headache (+) slight fever Exudate in the pharynx invariably thickens Dysphagia Result of pain, referred pain to the ear, cervical adenopathy, tenderness Pharyngeal wall Difficult, with a rasping, hawking effort and cough Hoarseness Larynx Reddened Dry, glazed appearance Coating of a mucoid secretion Lymphoid tissue Red and swollen Normal Acute Pharyngitis Treatment Antimicrobials Shortened course of the disease, decreased incidence of complications Warm throat irrigations Supportive care Adequate fluid intake, light diet, aspirin when indicated Acute Tonsilitis Etiology Acute supppurative bacterial tonsillitis: ß- hemolytic Streptococcus Group A-most common Streptococcus viridans Pneumococci Staphylococci H. influenzae Viral pathogens Pathology General inflammation and swelling of the tonsil tissue with an accumulation of leukocytes, dead epithelial cells and pathogenic bacteria. Other pathologic phases that may occur depending on the virulence of organism: 1. 2. 3. A simple inflammation of the tonsil area Formation of exudate. Cellulitis of the tonsil and its surrounding area 4. Formation of peritonsillar abscess 5. Tissue necrosis Symptoms Sore throat Various degrees of dysphagia General malaise Fever- 104°F Fetid breath Otalgia Complications: otitis media Tender cervical adenopathy Acute Tonsillitis Treatment Bed rest, adequate fluid intake, light diet Oral analgesics – control discomfort GARGLES Adds to a patient’s comfort & influence course of the disease to some extent 3 glassfuls of gargling solution each time Every 2 hours Heat of gargling solution is probably more effective than its medicinal content Isotonic saline solution, sodium perborate powder which is especially useful in Vincent’s infections or trench mouth ANTIBIOTICS - - - - Treatment of choice Penicillin – DOC unless organism is resistant or patient is sensitive; erythromycin Treatment should be continued for a full clinical course, bet 5-10 days Grp A B-hemolytic strep – maintain adeq antibiotic therapy to reduce possibility of complications such as RHD & nephritis Lingual Tonsilitis 1. Pharyngeal Tonsil 2. Palatine Tonsil 3. Lingual Tonsil 4. Epiglottis LINGUAL TONSILS The lingual tonsils are at the back of the tongue and cannot be seen by looking in the mouth. Function: guard for infective agents. Composition: Crypts lining by stratified squamousnonkeratinizing epithelium infiltrated with small lymphocytes. Lymphatic nodules LINGUAL TONSILITIS Less common than infections of the faucial tonsils due to the absence of the complex crypt arrangement and not as large as the latter. Rarely, acutely inflamed along with the faucial tonsils. More common among tonsillectomized patients and adults. Diagnosis Examination with a laryngeal mirror or a fiberoptic rhinolaryngoscope will reveal the presence of acutely inflamed and tender tissue mass with white exudate at the base of the tongue is diagnostic of lingual tonsillitis. Lingual Tonsillitis Symptoms Lingual tonsillitis presents with fever, sore throat, dysphagia, muffled voice, and pain at the level of the hyoid bone during swallowing. The pharynx may appear normal or mildly hyperemic on physical examination. Lingual Tonsillitis The anterior neck may be tender at the level of the hyoid bone, and cervical and submandibular adenopathy may be observed. A patient's voice also may have the classic muffled quality characteristic of severe tonsillar enlargement, but in lingual tonsillitis the uvula and peritonsillar area show no deviation or edema. TREATMENT Culture followed by appropriate antibiotic therapy is required. Lingual tonsillectomy by CO2 laser is performed when medical mgt is not effective. Membranous Pharyngitis VINCENT’S OR PLAUT’S ANGINA An acute necrotizing infection of the pharynx and mouth caused by a combination of fusiform bacilli (Fusiformis fusiformis) and spirochetes (Borrelia vincentii) which are normally present in the oral cavity Encountered in a limited form without systemic reaction and may be associated with other throat inflammations CLINICAL MANIFESTATIONS Commonly seen in young adults Presents with a unilateral sore throat that increases in intensity over several days with an associated referred earache on the same side. In addition, the patient complains of tender cervical adenopathy and foul breath Vincent’s Angina A deep well circumscribed unilateral ulcer of one tonsil. The base of the ulcer is gray and bleeds easily when scraped with a swab. DIAGNOSIS Diagnosis is confirmed by using a gentian violet-stained smear of the pharyngeal exudate, which demonstrates the presence of fusiform bacteria and spirochetes TREATMENT Supportive measures Hydrogen peroxide mouthwash Penicillin or Clindamycin Surgical debridement Diphtheria Corynebacterium diphtheriae or C. ulcerans Pharynx is most common site of infection Occurs more in nonimmunized individuals Diphtheria Caused by the toxin produced by the organism Sore throat – most common initial complaint Nausea, vomiting, dysphagia Diagnosis Examination: membrane present over tonsillar area with spread to adjacent structures Membranes dirty or dark green May obstruct view of tonsils Bleeding occurs with elevation of the membrane Diagnosis Causative organisms: toxigenic strains of Corynebacterium diphtheriae or C. ulcerans Smears from nasopharynx and tonsil cultured on MacConkey agar or Loeffler medium Suspicious strains tested for toxigenicity Treatment Two phases Use of specific antitoxin Elimination of organism from oropharynx Antitoxin: test patient first for sensitivity to the serum 40,000-80,000 units antitoxin diluted in saline, administerd IV Treatment Antibiotic treatment: Penicillin or erythromycin Eliminates carrier state Repeat culture performed to make sure clearance of organism in the pharynx Persistent organisms: Long term treatment with erythromycin Complications Airway obstruction – tracheostomy Cardiac failure Muscle paralysis Inflammatory process may spread to ears (otitis media), lungs (pneumonia) Pharyngeal Manifestations of Blood Disorders Infectious Mononucleosis Acute Infectious Disease Fever, Malaise, Somnolence, LN enlargement, Lymphocytosis Viral (EBV or CMV) Signs and Symptoms: Sore Throat Tonsillitis Fever Chills Malaise Complaints of feeling tired LN becomes enlarged and often ulcerates May block postnasal space Signs and Symptoms: Macular Rash 40% Diffuse and short duration Increased in patients receiving ampicillin Splenomegaly in 30% Jaundice in 5% Examthem on palate Short duration of usually less than 48 hours; commonly at the junction of the hard and sof palate Diagnostics: CBC Elevated WBC prodominated by neutrophils Later followed by lymphocytic leukocytosis Smear with examination for atypical lymphocytes “Mono-spot” positive Heterophil antibody titer exceeds 1:60 Throat culture to rule-out coexisting beta-hemolytic streptococcal pharyngitis Treatment: Symptomatic Prednisone For severe obstructive disease To reduce the ancillary inflammatory process Patient’s activities should be substantially reduced during the acute phase, with gradual return to normal activities Complications: Ruptured Spleen Guillain-Barre ascending paralysis CN paralyses Acute Leukemia Acute Leukemia First manifestations may be oral lesions Signs and Symptoms: Enlarged tonsils with ulcerative lesions Petechiae within the oral cavity Bleeding in affected areas Gingival ulceration Low grade fever Cervical adenopathy Diagnosis may be by bone marrow aspiration and peripheral blood exam Peritonsillar Cellulitis and Abscess Etiology: Infections of the tonsil proceed to diffuse cellulitis that could lead to peritonsillar abscess May occur rapid or late Unilateral and more common in older children and young adults Symptoms: marked dysphagia, pain referred to the ear in the involved site, increased salivation, fever Symptoms: Swelling interferes with articulation and speech is difficult Inspection is difficult due inability to open mouth Tonsil may appear normal as it is pushed medially and swelling develops lateral to tonsil Palpation – distinguishes an abscess from cellulitis Pathology: Suppurative infiltration occurs most often in supratonsillar fossa Causes edema of soft palate and displacement of uvula across midline Swelling extends to adjacent soft tissues, causing painful swallowing Bacteriology: Throat cultures are ineffective Culture of the actual abscess is ideal More common bacteria – Streptoccocus pyogenes; less common – Staph. aureus Peritonsillar Abcess: Peritonsillar Abcess Treatment: 1. Surgical incision and drainage or needle aspiration technique When pus is collected – peritonsillar abcess When no pus is collected – peritonsillar cellulitis 2. Antibiotics and warm saline irrigation Treatment: Procedure for surgical incision: Pharynx is sprayed with topical anesthesia 2 mL of xylocaine with adrenaline are injected Incision through the mucosa near the superior pole of the tonsillar fossa Tonsil suction to collect the pus #in children and young adults drainage may be performed after the application of cocaine to the site of incision and to the sphenopalatine ganglion. #younger children require general anesthetics Treatment: Immediate tonsillectomy is advisable for complete drainage and alleviates the need for a planned tonsillectomy six weeks later, at which time there is frequent scarring and fibrosis present in the tonsillar capsule is less identified. Treatment: Pathogens with a selection of antimicrobials ETIOLOGY Streptococcus Bacteroides Haemophilus Fusobacterium Staphylococcus Peptococcus ANTIBIOTIC Penicillin Cephalosporin Clindamycin Treatment: Warm saline throat irrigation provides symptomatic relief from the pain of pharyngitis of peritonsillar abcess Atrophic Pharyngitis Mild Cases –Mucosa appears thin & glistening or glazed –Absence of all but a few of the lymphoid collections that are seen in an average pharynx –blanket of mucus thicker & semitransparent Advanced cases “Pharyngitis sicca” - Dry Mucous coating gluelike in consistensy Dry furrowed mucous membrane Usually associated with atrophic dematitis or rhinitis sicca Etiology Not known definitely Air not sufficiently warmed & humidified by the nasal mucosa Trophic mucosal changes hyposecretion of mucus Symptoms Sense of dryness and thickness in the upper pharynx. Patient’s frequently clear their throats by “hawking” in an attempt to dislodge the adherent secretions. Mild degree of hoarseness may be present due to irritation of the larynx from the frequent attempts to clear the throat. Treatment Local application of Mandl’s paint to the pharynx is beneficial to stimulate secretion. 10 drops of saturated solution of potassium iodide may be given three times daily with meal. Combination of both is desirable. Breathing of warm moist air for 20-30 minutes once or twice a day may be done to moisten the inspissated secretion. Pharyngitis Associated with Tobacco Smoking Causes dry troublesome throat Patients start with symptoms of mild soreness then eventually with marked pharyngitis sicca Throat of a heavy smoker = dry, shiny and hyperemic pharyngeal mucosa. Chronic Tonsilitis Chronic Tonsillitis Persistent infection of the tonsils Repeated infections may cause the formation of small pockets (crypts) in the tonsils which harbor bacteria Clinical Picture: 1. 2. Enlarged tonsils, with evident hypertrophy and scarring. Crypts seem partially stenosed, but an exudate, often purulent, can be expressed from them. In some cases, one or two crypts are enlarged, and a considerable amount of “cheesy” or “putty-like” material can be expressed from them Small tonsil, usually recessed and often referred to as “buried”, in which the margins are hyperemic, and a small amount of thin purulent secretion can often be expressed from the crypts Symptoms: Chronic sore throat Halitosis Tonsillitis Persistently tender cervical lymph nodes Breathing partially blocked by enlarged tonsils Cultures usually show several organisms of relatively low virulence and rarely demonstrate beta-hemolytic streptococci Treatment Prolonged courses of penicillin Daily throat irrigations Dental or oral irrigating device to cleanse the tonsillar crypts Tonsillectomy Surgical removal of tonsils Relative Indication: recurrent episodes of documented grp A beta-hemolytic streptococcal infection Tonsillectomy Absolute Indications: Development of cor pulmonale by chronic airway obstruction Tonsil or adenoid hypertrophy with sleep apnea syndrome Hypertrophy to the extent of causing dysphagia with associated weight loss Excisional biopsy for suspected malignancy (lymphoma) Recurrent peritonsillar abscess or abscess extending into adjacent tissue spaces Tonsillectomy in children: Indications: Documented recurrent bouts of tonsillitis (despite adequate medical management) Tonsillitis assoc w/ persistent & pathogenic streptococcal cultures (carrier state) Tonsil hyperplasia w/ functional obstruction Hyperplasia & obstruction remaining 6mos after infectious mononucleosis Rheumatic fever history w/ heart damage assoc w/ chronic recurrent tonsillitis & poor antibiotic control Tonsil & adenoid hypertrophy assoc w/ orofacial or dental abnormalities that narrow the upper airway Recurrent or chronic tonsillitis assoc w/ persistent cervical adenopathy Tonsillectomy Contraindications: Repeated upper respiratory infections Systemic or chronic infection Fevers of unknown origin Enlarged tonsils w/o obstructive symptoms Allergic rhinitis Asthma Blood dyscrasia General inability or failure to thrive Poor muscular tone Sinusitis