Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
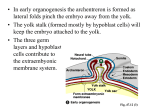
Yeasting 11-16 Review: Epiblastic cells migrate and take up residency in original hypoblastic cells (now called intraembryonic endoderm); those that stay btw epiblast (ectoderm) and endoderm mesoderm Neural crest—specialized tissue; multipotential; give rise to melanocytes and peripheral portion of nervous system (primary sensory neurons, post ganglionic autonomic neurons, Schwann cells) Also gives rise to CT in the head and neck region, some of this is carried down into thorax to give rise to portions of the heart **Ectoderm and endoderm tell mesoderm that they will protect and sustain (nourish) it if it supports (physiologically and physically) them Mesoderm- skeletal and muscular system (physical support), cardiovascular system (physiologic support through circulation); ectoderm protects in on the outside (protection) ; endoderm nourishes it (protective and nourishing) 3 germ layers (trilaminar) cooperate to form the organs which become the organism Intraembryonic mesoderm: regions in lateral plate meso where intracellular spaces develop; these coalese to form intraembryonic coelom (in some spots this is continuous with extraembryonic coelom); this is within the embryo proper ** participates in formation of coelom, other types of mesoderm do not. Paraxial mesdoderm: gives rise to somites; does not participate in coelom formation Intermediate mesoderm does not participate in coelom formation 2ndary yolk sac (lined with endoderm at this point) becomes known as splanchnic mesoderm; mesoderm of lateral plate origin related to overlying ectodermsomatic mesoderm Figure 5-1 bi trilaminar disc: start out as a disc and a third layer develops Now, the formation of the cylinder comes next!! intraembryonic coelom develops and this partially separates yolk sac from the rest of the disc; this 2ndary umbilical vesicle will be ultimately connected to the major portion of the embryo’s body through tissue in the midline and becomes known as a mesentery As this happens, cells related to developing nervous system (axial structure) and tissue relating to developing somites (para axial) proliferate rapidly/massively and are organized into the stages of the early nervous system, which gives rise to muscles and skeletal system of the body All of this takes place near/in the longitudinal axis of the developing embryo. -Creates growth pressures, such that axial region is adding cells much more rapidly than the periphery which causes the disc to BUCKLE…disc will rise up and overflow the margin like a cupcake. This folding occurs both longitudinally AND transversely. Cranial structures change their orientation, caudal changes their orientation and lateral change theirs. BOTH longitudinal and lateral foldings occur simulataneously. Orropharyngeal membrane-- between here and leading edge of embryonic disc is cardiogenic area is where the heart will develop. Intraembryonic coelom will cross the midline in this area. There is also additional tissue in this region. At the edge of the disc, branch out into the amnion and the 2ndary yolk sac. In caudal area, there is the area for the primitive groove/streak (not shown) btw here and edge of disc, where connecting stalk is attached, is another specialized area where the cloacal membrane is. Mesoderm does not go between these 2 areas, oropharyngeal and cloacal these membranes are weak and should break down relatively early) ** these areas are the beginning of the digestive system (oropharyngeal) and the terminal end of the digestive system (claocal) With the folding process (created by excessive growth), the edge of the embryo is displaced inferiorly (edge is not moving inferiorly, middle region is just rising up over edge) This shifts the relative position of the edge of the disc, shifts intrambyronic coelom and connective stalk bc of this folding process, a portion of the 2ndary yolk sac is now taken up into the embryo’s body. This portion of the 2ndary yolk sac (DEFINITIVE) will become the primitive digestive system; another portion of yolk sac will remain outside the embryo (will ultimately be pinched off) RECAP: As longitudinal folding is taking place, what was a flat disc now with developing somites, etc. (paraxial), amnion taking off from edge and going around (along with yolk), intraembryonic coelom separating what will become body wall from digestive system. With further development, somites proliferate increasing axial tissue more rapidly than adding cells to the edge of disc. Disc is overflowing cranially and caudally, and also rising up, so that the edge of the disc moves inferiorly (relatively); as this happens, the edge of the disc (circumference) gets relatively smaller and smaller as more and more tissue develops in the axial region. What becomes body wall is the edge of the embryo (continuous with amnion), hanging through this area is a portion of yolk sac not incorportated into embryonic body What was the connective stalk (caudal end) has now been carried around to the ventral aspect as the tail fold develops. As amnionic membrane proliferates and amnionic cavity enlarges we can see how it can shrink wrap down around the connective stalk and other things that extend from the ventral aspect of cylindrical body (encircles these structures) Diverticulum out of yolk sac going into connective stalk = ALANTOIS Intraembryonic coelom crosses the midline at the cardiogenic area *Periphery of embryonic disc becomes the umbilicus (the naval) -early on this primitive naval is relatively large; as the rest of the disc develops (more centrally) and periphery of disc lags behind a bit, with the folding processes the umbilical ring gets progressively relatively smaller (bc it’s not growing as rapidly as center of embryo). -As central region proliferates , will create growth pressures to cause embryo to rise up from peripherylongitudinal growth related to NS will force cranial region out over the edge of cranial disc creates head fold. Resulting in a change in orientation in the cardiogenic area, in such a way that they are now on ventral aspect of a cylinder. Yolk sac is incorporated into the head fold process and extends out into oropharyngeal membrane. Now the nervous system has become most cranial (head fold is now cranial to cardiogenic area). Oropharyngeal membrane ends up in back of mouth (where oral cavity merges with pharyngeal cavity); Cardiogenic area ends up in thorax as heart develops; umbilical ring at edge of disc becomes the naval (umbilicus); this area ultimately gets stretched out! -At posterior end there is a tail fold developing; edge of disc does not actively move ventrally, but excess tissue pushes out; cloacal membrane that was in disc now ends up in ventral aspect of cylindrical embryo (temporarily) -Connective stalk with alantois which was extending from edge of disc, now has moved relatively ventrally; still associated with primitive umbilical ring, but now not most caudal part of the embryo; part of this will be incorporated into the embryo’s body (becomes pad of fat in deep aspect of anterior abdominal wall). The yolk sac that was hanging underneath the portion that relates to embryonic disc has now been incorporated into the cylinder (making a lumen); portion of yolk sac remains outside and will ultimately be pinched off. **Emphasize longitudinal folding (hard to grasp), also foldings occur laterally. Coelom is caught within the folding process. Lateral folding can see edge of disc on 5-1 B3. Rise up from the edge of the disc; continues to rise up and gets larger so that original umbilical ring gets relatively smaller; part of yolk sac goes into cylindrical embryo and some stays outside (what is umbilical ring??) Connective stalk and yolk sac become components of the umbilical cord! Lining of 2ndary yolk sac definitive intraembryonic endoderm derived from epiblast; these pushed hypoblast out of the way (hypoblastic cells make primary yolk sac) See fig 5-2. Tissue near original cranially edge of embryonic disc, cranial region of umbilical ring SEPTUM TRANSVERSUM This is a major player in the formation of the thoraco-abdominal diaphragm which separates thoracic from abdominal cavity; connective tissue in diaphragm is largely of septum transversum origin See fig 5-4 Mesenchyme of the connective tissue… Proximal portion of the connective stalk gets incorporated into the body, allantois becomes a portion of urinary bladder that’s inside the body wall; tissue immediately surrounding this is incorporated into the body wall. Triangular region of abdominal region this contains remnant of the allantois. See fig 4-12-With folding process and heart developing, there are BVs developing within the embryo proper. Connect to BVs developing within the yolk sac (both intra and extraembryonic portions), these connect to BVs that have developed within the connecting stalk (now the umbilical cord), which further connect to fetal embryonic BVs that have developed within the placenta Fetal heart starts beating at 4th wk and moves blood throughout system; yolk sac gives rise to fetal RBCs (important in hemopoietic tissuegives rise to RBCs), and perhaps some leukocytes ; also within yolk sac are “primordial germ cells” See pic from slides Primordial germ cells (distinct, have their own identity) are within bi and trilaminar discs near caudal end; during epiblastic migration, nature moves these into yolk sac wall (where they reside temporarily) to help get them out of all the traffic dealing with primitive streak/groove area; this greatly decreases their potential to migrate to somewhere that they shouldn’t be; they migrate back into embryo proper (from yolk sac) while the gonads are developing. Yolk sac does not provide any direct nourishment to embryo (only may participate in indirect nourishment bc before vasc. system develops, embryo is surrounded by amnionic fluid, chorionic fluid, both of which originally are derived from maternal tissue fluid (extracellular fluid, nutrients are found in here) Yolk sac provides a large entrée area for nutrients diffusing through fluids to reach the inneraspect of developing embryo body to the ventral aspect; other nutrients come in through the dorsal aspect bc integument hasn’t become waterproof yet, eventually yolk sac may participate in allowing nutrients to diffuse up into the embryo’s body. See fig 5-9, 5-12 appreciate SIZE= teeny weeny!! @ 16 mm looks somewhat human. _____________________________________________________________________________________ Intro to what’s to come…. Coelom= cavity Extraembryonic coelom (chorionic cavity), intraembryonic coelom (develops within intraembryonic mesoderm) gives rise to cavities within our body 1. pericardical cavity (1) 2. pleural cavity (2) 3. peritoneal cavity (1) Pericardial cavity related to the heart Pleural cavities related to the lungs Peritoneal cavities related to abdominal viscera In us, these are separate. BUT originally, they were all from same cavity These body cavities develop from mesoderm Cavities are lined with mesothelium (have special properties, these are lined with “serous membrane” which consists of CT and mesothelium); epithelial in function, mesodermal in origin Membrane that lines cavity onto the body wall (see pic in slides, anatomy of thorax) serous membrane lining lungs in contact with Body cavities have tissue next to the body wall, reflects onto organs that stick into cavity “Parietal” plura= serous membrane not in direct contact with the organ; more related to body wall surrounding/supporting structures (ex. surrounds supporting structure of lungs) “Visceral” plura= surrounds the organ (ex. surrounds the lungs) In general…. If serous membrane is in contact with organs covering them= “Visceral”(plura/pericardium/peritoneal) If not in contact with organ, then “Parietal”… Pleural cavity opened up (picture in slides); see where BVs and other ducts/structures leave plura Visceral and parietal plura (closed spaces ) will go out and join/merge; see picture of thorax and organs Cross section through thorax, see lung tissue and parietal plura (next to body wall), membrane then is on surface of lung (visceral plura), follows the contour of the lung, back to the root where it reflects off and becomes parietal plura again. Can see similar coverings of heart (serous (visceral) and parietal pericardium) does serrous pericardium= visceral pericardium?? Inferior aspect of thoracic cavity, formed of diaphragm. Composed of muscle tissue and a central tendon; muscle tissue is radially arranged headed toward the central tendonous area. Abdominal aspect, see branches of aorta, muscles are innervated by left and right phrenic nerves (come out of cervical cord through C3, 4, 5 spinal nerves) Diaphragm= dome shaped (normally); muscle fibers contract from a stable base of vertebrae or ribs, radial muscle fibers pull central tendonous area inferiorly, reduces outside air pressure, forces are in (INSPIRATION); as diaphragm relaxes along with elastic recoil from lungs, air is pushed back out (EXPIRATION) Within abdominal cavity, there is a peritoneal cavity lined by serous membrane… Digestive tract (originally in embryo)is coiled in membrane and suspended from the dorsal body by original connection that didn’t break down when intraembryonic coelom formed; this original connection is now called the mesentery. “MESO”= relates to supporting structures (has nerves in it). “ENTERY”= relates to gut; mesentery supporting structure to the gut; carries BVs, nerves from body wall to the gut structures How all of this has come about… Intraembryonic coelom- develops within lateral plate mesoderm; cells lining this are of mesodermal origin; in mid region of embryonic disc, this intraembryonic coelom is open to the sides of the embryonic disc (extraembryonic coelom); more cranially, coelom is tubular/cylinder/canal and not open directly to outside. See fig 8.1 Tubular coelom goes up cranially crosses midline in cardiogenic area, comes back to other side and opens into the wide coelom. This intraembryonic coelom is initially U-shaped. The ends of the U open widely in the mid region to the outside. Wide connection of coelom allows yolk sac to develop independently of the rest of the embryo; Our digestive tracts are ~ 20 ft., body is much shorter in relation. If yolk sac were bound to rest of body, we would have a very short digestive tract or a very long body (yolk sac is suspended from midline by a mesentery, develops independently) See Pic in slides-- Intrembryonic coelom is wide open to outside; tube within a tube develops how it wants to (yolk sac) independent from surrounding body See Fig 5.16 in slides. Things are folding over moving ventrally and caudally as the head grows out. See fig 8-3 U-shaped coelom has been bent upon itself, folding over (what was a unipolar U now gets bent); portion related to heart curves down ventrally and caudally, head portion moves over. Coelom related to developing heart (pericardial coelom), related to abdominal cavity (peritoneal coelom), connection of these ( temporarily called this; pericardial peritoneal canal along the digestive tract; lungs haven’t grown in yet) Septum transversum= original leading edge of embryonic disc; btw cardiogenic area and edge of disc becomes the 1) connective tissue of diaphragm, 2) connective tissue of liver, 3) tissue between liver and stomach With folding, septum transversum is carried ventrally and caudally so a portion of the gut is trapped within the embryo’s body; coelom that was coming forward now bends; spectrum transersum is at edge in contact with yolk sac and primitive gut that will go into embyro’s body See figure 8-4 Coelom is becoming tubular, crossing midline and opening back up; septum transversum, comes up and encroaches onto coelom to create a transverse septum with digestive tract, coelom, body wall going through the area. Septum transversum is brought around to form a ventral block of tissue See fig 5.6 slides ventral view with body wall of heart taken away Fig 14-20 slides—Coelom is bent around (U is bent), septum transversum intervenes btw pericardial coelom and gut, helps form inferior aspect of thoracic cavity (septum transversum), helps to form the connective tissue of the liver, and helps to form tissue of digestive tract See fig 8-5 see pericardial peritoneal canals or primitive pleural cavities; see pericardial cavity and small communication in btw; as BVs grow and move toward center (midline) pinch off communication btw pericardial cavity and pericardial peritoneal canals Pericardial cavity becomes separate and isolated space as will each of pericardial peritoneal canal As lungs grow into the pericardial peritoneal canals, they are called primitive pleural cavities. Btw pericardial coelom and the body wall is connective tissue surrounding the heart. This CT is broken into by the enlarging pleural cavities. They are dissecting lateral to the heart forward enlarging to give space for lungs to develop into. They will not fuse anteriorly, but they enlarge. Heart is essentially sitting there surrounded by a space (pericardial coelom and related serous membrane) and CT that was dissected free from body wall, this becomes fibrous pericardium (collagenous layer that holds heart in position) Diaphragm- develops from septum tranzversum; as this comes in (when cylindrical body forms) it is found in the cervical region bc developing head area is larger than caudal area; during the initial folding process the tissue known as septum transversum comes in at cervical levels C3, 4,5 and will later move caudally to its definitive location. When septum transversum CT is at C3,4, 5, myoblasts from C3,4,5 somites migrate into septum transversum and populate it, and attract a nerve supply from ventral primary rami C3,4,5 (see fig 8-9); As embryo develops more, diaphragm will move further and further caudally, pulling it’s nerve supply with it. Diaphragm will have tissue (in addition to septum transversum) also derived from mesentery of gut (gives rise to posterior midline of diaphragm); pleural cavity will open into peritoneal cavity. This area is closed by formation of membranes, separating pleural cavity from peritoneal cavity, known as pleural peritoneal membranes (see pic from slides). They will fuse with septum transversum and fuse with dorsal mesentery of the gut; then pleural cavities will excavate periphery of diaphragm away from body wall to become dome shaped. Diaphragm has for CT elements that merge together: 1) septum transversum 2) body wall 3) dorsal mesentery 4) pleura peritoneal membranes Muscles from C3, 4, 5 grow into these CTs, populate them and are innervated by C3, 4, 5 branches known as the phrenic nerve