Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Coronary artery disease wikipedia , lookup
Remote ischemic conditioning wikipedia , lookup
Myocardial infarction wikipedia , lookup
Heart failure wikipedia , lookup
Cardiac surgery wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
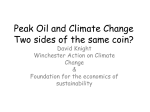
Relationship between right ventricular ejection fraction and maximum exercise oxygen consumption: A methodological study in chronic heart failure patients Marcus Hacker, MD,a Stefan Störk, MD, MSc,b Diana Stratakis, MD,c Christiane E. Angermann, MD,b Rudolf Huber, MD,c Klaus Hahn, MD,a and Andreas Tausig, MDa Background. Peak oxygen consumption at maximum exercise (peak VO2) predicts survival in chronic heart failure (CHF) patients. Right ventricular ejection fraction (RVEF) at rest has been reported to correlate with peak VO2. We evaluated the strength and consistency of the association between peak VO2 and RVEF measured by different radionuclide ventriculography (RNV) techniques in a prospective cohort study. Methods and Results. In 58 consecutive CHF patients (mean age, 53 years; 39 patients with dilated cardiomyopathy; 48 men), upright symptom-limited bicycle ergometry was performed. During exercise, ventilatory and gas exchange data were recorded and peak VO2 was calculated. RVEF was calculated by use of first-pass (FP) RNV with single and dual region of interest (ROI) acquisition and planar multigated acquisition (MUGA). Irrespective of the method used, RVEF showed no relevant correlation with the corresponding peak VO2 value (r ⴝ 0.11 for FP single ROI, r ⴝ 0.06 for FP dual ROI, r ⴝ 0.16 for MUGA). Peak VO2 or changes in peak VO2 after 6 and 12 months of follow-up were not determined by RVEF measurements. Conclusion. In CHF patients no association was found between peak VO2 at maximum exercise and RVEF at rest with different RNV techniques. Changes in exercise capacity are not reliably reflected by changes in RVEF measurements at rest. (J Nucl Cardiol 2003;10:644-9.) Key Words: Chronic heart failure • right ventricular ejection fraction • peak oxygen consumption • radionuclide ventriculography Chronic heart failure (CHF) remains a leading cause of morbidity and mortality, despite improved pharmacologic and surgical treatment options.1 Peak oxygen consumption at maximum exercise (peak VO2) or achieved percentage of predicted peak VO2 (%VO2) is an established tool for monitoring and guiding CHF therapy.2-9 Hemodynamic parameters at rest have also been shown to predict outcome in CHF patients. Besides left ventricular (LV) ejection fraction (EF), right ventricular (RV) EF seems to play an important role as a prognostic determinant and has been described as an independent From the Departments of Nuclear Medicinea, and Pulmonology, c University of Munich, Munich, and Department of Cardiology, b University of Würzburg, Würzburg, Germany Drs Hacker and Störk share the authorship of this article equally. Received for publication Sept 17, 2002; final revision accepted May 28, 2003. Reprint requests: Marcus Hacker, MD, Klinik und Poliklinik für Nuklearmedizin der LMU, Ziemssenstrasse 1, 80336 München, Germany; [email protected]. Copyright © 2003 by the American Society of Nuclear Cardiology. 1071-3581/2003/$30.00 ⫹ 0 doi:10.1016/S1071-3581(03)00659-7 644 predictor of survival in 205 patients with moderate CHF.10 In a small group of patients with advanced CHF, a close correlation between RVEF and peak VO2 has been reported,11 suggesting good agreement between RV function assessed at rest and a combined (RV and LV) measurement of functional exercise capacity. Radionuclide ventriculography (RNV) measures RVEF independently of RV geometry and is most commonly used for serial RVEF assessment in CHF patients. RNV acquisition in CHF patients is not standardized, mainly because it is unknown whether RVEF values measured with more sophisticated techniques will allow better patient management or whether standard techniques will suffice. The majority of studies calculated RVEF by multigated acquisition (MUGA). However, planar MUGA in the left anterior oblique projection tends to underestimate RVEF if there is major overlap of the right atrium and right ventricle, which is common in CHF. First-pass (FP) techniques in the 30° right anterior oblique projection avoid this limitation and are therefore assumed superior to planar MUGA in terms of calculating “true” RVEF.12,13 Moreover, FP RNV can be easily acquired without exposing the patient to additional radi- Journal of Nuclear Cardiology Volume 10, Number 6;644-9 Hacker et al Lack of correlation of right ventricular function and peak oxygen consumption in CHF ation if MUGA or technetium 99m– based myocardial scintigraphy is planned.14 This study aimed to evaluate, in cross-sectional and longitudinal analyses, the strength and consistency of the association between different techniques of radionuclide RVEF measurement at rest and peak VO2 at maximum exercise in a nonselected group of CHF patients. 645 Table 1. Baseline characteristics of study cohort (n ⫽ 58) Characteristic Data Consecutive CHF patients from our heart failure outpatient clinic who were hospitalized to optimize medical treatment and/or to assess the need for heart transplantation were eligible. Between January 1998 and November 2000, in 89 patients cardiopulmonary exercise testing and RNV (FP and MUGA) were performed on the same day. This report is restricted to 58 patients (65%) in whom baseline data were complete regarding three different RNV acquisition techniques and cardiopulmonary exercise testing. Follow-up was scheduled at 6 and 12 months. Age (y) Body mass index (kg/m2) Female gender NYHA class II III IV Cardiac diagnosis Ischemic heart disease Dilated cardiomyopathy Other (hypertrophic/valvular cardiomyopathy) ACE inhibitor Diuretic -blocking agent Digoxin Nitrate Cardiopulmonary Exercise Testing Values are mean (range) or No. (%). ACE, Angiotensin-converting enzyme. Spiroergometry was performed on an electronically braked ergometer in an air-conditioned room at 11:30 AM. Patients had taken their regular medication with a light breakfast at 8:00 AM. Patients started cycling at a workload of 10 W or 30 W depending on their clinical status, followed by a 10 W increase after each minute up to maximum physical exertion. Respiratory gas exchange and electrocardiographic changes were monitored continuously. Peak VO2 was defined as the highest VO2 during any stage that could be sustained for more than 1 minute. Respiratory threshold was documented but not used in the evaluation of exercise capacity and was reached in 96% of examinations. None of the 58 patients developed exercise-induced ischemia (ie, horizontal or downsloping STsegment depression ⬎1 mm) before reaching the point of maximum exertion or respiratory threshold. Blood pressure was recorded automatically every minute. and the end-systolic difference image. The phase image was used to identify the pulmonic valve and tricuspid valve planes. The end-systolic region was drawn from the end-systolic image as described previously.13 FP RVEF was calculated by use of a single end-diastolic frame (single ROI) and both end-diastolic and end-systolic frames (dual ROI). LVEF was calculated by the dual ROI method. After the FP acquisition, patients were positioned supine for planar MUGA. A Picker Prism 2000 gamma camera (Philips, Cleveland, Ohio) equipped with a low-energy high-resolution collimator was positioned at the 40° left anterior oblique projection (“best septal view”). LVEF and RVEF were calculated by the dual ROI method. The background ROI was placed adjacent to the free wall of the ventricle. METHODS CHF Patients 52.9 (28–76) 26.7 (17–35) 10 (17) 21 (36) 28 (48) 9 (16) 17 (29) 39 (67) 2 (4) 52 (90) 53 (91) 40 (69) 31 (53) 8 (14) Data Analysis RNV RVEF studies were performed at rest by in vivo red blood cell labeling. Sn-pyrophosphate was injected intravenously. After 20 minutes, patients were placed upright in front of a Picker SIM 400 multicrystal camera, equipped with a lowenergy, high-sensitivity, parallel-hole collimator in approximately 30° right anterior oblique projection. Then, 740 MBq Tc-99m pertechnetate was injected. The camera acquired a total of 1500 frames at 25 milliseconds per frame. An initial RV region of interest (ROI) was drawn and the time-activity curve generated. The start and stop of the RV phase and the first identifiable RV beat were defined and the ROI modified through iterative steps by the computer software. Borders of the RV end-diastolic region were determined from the phase image Results are presented as mean ⫾ SD and range, unless stated otherwise. Differences between groups at baseline and differences between follow-up examinations were assessed by use of the Wilcoxon test for unpaired and paired data as appropriate. The Spearman coefficient (r) is given when correlations are reported. Univariate determinants of peak VO2 were selected by means of linear regression analysis from baseline characteristics (Table 1), blood pressure variables, and heart rate, with a liberal ␣ of .15. In multivariate models statistical significance was accepted at an ␣ of .05. The identical approach was followed in building models with change in peak VO2, percent of predicted VO2, and O2 uptake per heart rate as dependent variables. All P values are reported 2-sided. 646 Hacker et al Lack of correlation of right ventricular function and peak oxygen consumption in CHF Journal of Nuclear Cardiology November/December 2003 Table 2. Descriptors of symptom-limited exercise test in baseline cohort (n ⫽ 58) Mean ⴞ SD (range) Descriptors Before exercise test Systolic blood pressure (mm Hg) Diastolic blood pressure (mm Hg) Heart rate (beats/min) O2 per heart rate (mL) At maximum exercise Systolic blood pressure (mm Hg) Diastolic blood pressure (mm Hg) Heart rate (beats/min) O2 per heart rate (mL) Peak VO2 (mL/min) Peak VO2 (mL · min–1 · kg–1) % Predicted VO2 Respiratory quotient Radionuclide measurements RVEF: MUGA (%) RVEF: FP single ROI (%) RVEF: FP dual ROI (%) LVEF: FP dual ROI (%) LVEF: MUGA (%) 116 ⫾ 20 (70–170) 79 ⫾ 14 (46–120) 77 ⫾ 15 (50–120) 3.89 ⫾ 0.90 (2.05–6.12) 150 ⫾ 37 (80–256) 84 ⫾ 11 (62–109) 130 ⫾ 29 (69–197) 9.92 ⫾ 2.61 (6.13–16.20) 1206 ⫾ 442 (542–2420) 15.2 ⫾ 5.1 (7.4–28.0) 56 ⫾ 15 (27–102) 1.05 ⫾ 0.09 (0.77–1.41) 39 ⫾ 13 (10–76) 43 ⫾ 9 (16–66) 48 ⫾ 11 (15–68) 32 ⫾ 9 (18–50) 29 ⫾ 11 (13–57) RESULTS Cross-Sectional Analysis at Baseline In this study 58 patients, 48 men and 10 women, met the requirements for analysis (as described in the “Methods” section). The characteristics of the study cohort are given in Table 1. All patients received at least 2 medications for CHF, predominantly a combination therapy of angiotensin-converting enzyme inhibitors, diuretics, and -blocking agents. No cardiac events were registered during exercise. The detailed descriptors of cardiopulmonary exercise tests and radionuclide assessments are given in Table 2. Mean peak VO2 and LVEF were severely compromised, and RVEF was moderately compromised, which is consistent with advanced CHF. Peak VO2 was 10 mL · kg⫺1 · min⫺1 or lower in 6 tests, and was between 10 and 14 mL · kg⫺1 · min⫺1 in 22 tests. FP RVEF (dual ROI) recorded the highest RVEF values, followed by FP RVEF (single ROI) and MUGA RVEF. The correlation in RVEF between the two FP methods was moderate (r ⫽ 0.75) but was worse between FP methods and MUGA (r ⫽ 0.61 for single ROI and r ⫽ Figure 1. Correlation between peak VO2 and RV function measured by 3 different radionuclide techniques at baseline (n ⫽ 58). 0.47 for dual ROI, respectively). No correlation was found between MUGA LVEF and MUGA RVEF (r ⫽ 0.03). In addition, no correlation was found between any RVEF method and peak VO2 (Figure 1). In univariate linear regression analysis, age, body mass index, New York Heart Association (NYHA) class, and therapy with -blocking agents showed inverse associations with peak VO2. In multivariate analysis only age and body mass index remained as independent determinants of peak VO2 (P ⬍ .001). RV measurements were not associated with peak VO2 in regression analysis, either univariately or after adjustment for age and body mass index (Table 3). LV measurements showed no association with peak VO2 in univariate analysis but showed a trend after adjustment for age and body mass index (Table 3). Journal of Nuclear Cardiology Volume 10, Number 6;644-9 Hacker et al Lack of correlation of right ventricular function and peak oxygen consumption in CHF Table 3. Multivariate linear regression analyses for peak VO2 at baseline  coefficient (95% confidence P interval)* value RVEF: RVEF: RVEF: LVEF: LVEF: MUGA (%) FP single ROI (%) FP dual ROI (%) MUGA (%) FP dual ROI (%) 0.07 0.16 0.03 0.10 0.08 (–0.07 (–0.08 (–0.10 (–0.01 (–0.01 to to to to to 0.15) 0.16) 0.14) 0.22) 0.18) .29 .31 .59 .08 .09 *Each  coefficient refers to a separate analysis, adjusted for age and body mass index. Serial Examinations at 6 and 12 Months Complete follow-up data (3 different RNV acquisitions and cardiopulmonary exercise testing) were available for 36 patients at 6 months and 25 patients at 12 months. Reasons for incomplete data at 6 and 12 months, respectively, were death (n ⫽ 6 and n ⫽ 9), inability to perform the exercise test because of the severity of CHF (n ⫽ 3 and n ⫽ 4), no follow-up visit (n ⫽ 2 and n ⫽ 5), invalid exercise test (n ⫽ 0 and n ⫽ 1), and incomplete RNV data (n ⫽ 11 and n ⫽ 14). Mean peak VO2, RV and LV measurements, and NYHA class were unchanged after 12 months of follow-up (Table 4). Multivariate regression coefficients at 6 and 12 months were unchanged compared with baseline (data not shown). We repeated all analyses using change in peak VO2, percent of predicted VO2, or O2 per heart rate, respectively, as the dependent variable. Finally, all analyses were repeated after excluding patients with an anaerobic threshold lower than 1.05, because this subgroup might be characterized by other unmeasured coexisting conditions. In none of these analyses were associations observed between measurements at rest and at maximum exercise. DISCUSSION The main finding of this investigation in CHF patients was that RVEF assessment at rest, independent of the radionuclide technique used, showed no correlation with peak VO2 measured at maximum exercise. Our findings support the view that changes in hemodynamics at rest and at maximum exercise occur independently of each other in CHF patients. It is therefore not possible to infer reliably the state of exercise capacity based on resting RNV in the same patient. Parallel monitoring of the resting and exercise state may be desirable in high-risk groups. The potential limitations of this investigation need to 647 be considered. Radionuclide assessment and ergospirometry are affected by age, hormonal changes, level of medication, conditioning status, and biologic variability, as well as by patient motivation in the case of exercise testing. In this investigation care was taken to minimize these influencing factors. RNV and ergospirometry were performed in a standardized fashion after recompensation and stabilization of decompensated CHF. Maximum exertion during ergospirometry was enforced, and peak VO2 at maximum exercise level rather than at the level of anaerobic threshold was used as our primary parameter of interest. Medication was found to be relatively homogeneously distributed among patients. Thus, although we cannot exclude that these effects distorted existent correlations, we consider it unlikely. This view is strengthened by the consistency of our null findings in all cross-sectional and serial analyses. We found a moderate correlation between single and dual ROI FP RVEF. However, the correlation between MUGA RVEF and the FP methods was only fair. This is in accordance with a study comparing different radionuclide methods with cine magnetic resonance imaging as the reference standard.13 In this study cine magnetic resonance imaging correlated well with FP methods but only weakly with MUGA. RVEF values and RVEF changes over time did not correlate with peak VO2 or changes in peak VO2 in any of the univariate or multivariate regression analyses. Our findings strongly suggest that hemodynamics at rest and at maximum exercise do not change simultaneously. Results from other studies are inconsistent. Baker et al15 found a correlation between FP RVEF (single ROI) and peak VO2 in 25 patients with severe heart failure. In a group of 24 patients with severe heart failure, Ben-Gal et al16 showed that RVEF values lower than 30% measured with FP and MUGA RVEF were associated with significantly lower VO2 values, suggesting a pathophysiologic relationship between RVEF and peak VO2. Conversely, Clark et al17 could not find such a correlation between MUGA RVEF and peak VO2 in 42 CHF patients. Similarly, Szlachcic et al18 were unable to detect a correlation between MUGA RVEF and VO2 in 27 patients. The comparability of all these studies is limited, however, because they were based on low patient numbers, major differences in the severity of CHF, and different RVEF calculation methods. Moreover, CHF may predominantly be due to RV or LV dysfunction or a combination of both, may respond differently to treatment over time, and may affect exercise capacity very differently despite uniformly lowered LVEF. In general, cardiomyopathy induces LV remodeling as an adaptive mechanism, leading to LV enlargement, hypertrophy, and distortion of regional and global geometry.19 However, compromised cardiac output is not 648 Hacker et al Lack of correlation of right ventricular function and peak oxygen consumption in CHF Journal of Nuclear Cardiology November/December 2003 Table 4. Paired differences of follow-up examinations after 6 and 12 months Paired differences between baseline and 6 mo follow-up, (n ⴝ 36) NYHA class Body mass index (kg/m2) Peak VO2 (mL · min–1 · Kg–1) RVEF: MUGA (%) RVEF: FP single ROI (%) RVEF: FP dual ROI (%) LVEF: MUGA (%) LVEF: FP dual ROI (%) Paired differences between baseline and 12 mo followup, (n ⴝ 25) Mean SD P value Mean SD P value 0.16 –0.62 –0.21 –3.20 –1.47 –3.73 –2.82 –1.84 0.64 2.88 3.80 8.59 10.61 12.62 6.81 9.03 NS NS NS .043 NS NS .008 NS 0.27 –0.84 –0.88 –3.44 –0.65 –3.25 –4.00 –4.07 0.70 1.66 2.72 7.98 11.50 17.09 10.15 10.03 NS .019 NS NS NS NS NS NS NS, Not significant. paralleled by compromised exercise capacity and NYHA functional class in all patients. Conversely, other reasons for a reduced exercise capacity include a diminished nutritive blood flow to skeletal muscles and abnormalities of skeletal muscle metabolism.20,21 These factors were not measured in this study but may, in part, explain our null findings. Moreover, deteriorating RV function is not solely a consequence of pulmonary hypertension due to LV dysfunction but may also be observed with normal pulmonary artery pressure.22 Inclusion of patients with primary RV dysfunction in our study may be another reason for the lack of correlation of RVEF and exercise capacity. To our knowledge, there are no studies that have systematically—in cross-sectional and longitudinal analyses— compared peak VO2 at maximum exercise with the different radionuclide modalities to calculate RVEF, and the FP (dual ROI) approach has not yet been used for this problem. For the clinical feasibility of serial RVEF measurements, the accuracy, precision, and practicalities of the methodology need to be considered. In patients with atypical heart-axis orientation, FP RVEF can hardly be obtained because it cuts off parts of the ventricle. In addition, using the dual ROI method delineation of end-diastolic and end-systolic expansion of the right ventricle, particularly at the valve plane area, can be difficult. From our analysis of serial measurements, we conclude that a decrease in peak VO2 values does not necessarily indicate a deterioration in RVEF. For serial measurements, it seems advisable to monitor CHF patients with the same method of RVEF calculation over time. This might be especially important in patients who are unable to perform exercise testing. Whether RVEF measurements in general and MUGA in particular represent independent predictors of clinical outcome in patients with advanced CHF is within the scope of an ongoing study at our institution. In conclusion, RVEF calculated by planar MUGA correlated moderately with FP RNV (single ROI) values. Regardless of the RNV technique applied, no association was found between RVEF at rest and peak VO2 at maximum exercise, and the change in peak VO2 was not reflected by the change in RV function. Peak VO2 and RVEF at rest may reflect different pathophysiologic aspects in moderate and severe CHF, thus justifying assessment of both parameters for optimal monitoring and risk evaluation in this group of patients. Acknowledgment The authors have indicated they have no financial conflicts of interest. References 1. Cowie MR, Mosterd A, Wood DA, et al. The epidemiology of heart failure. Eur Heart J 1997;18:208-25. 2. Pardaens K, Van Cleemput J, Vanhaecke J, Fagard RH. Peak oxygen uptake better predicts outcome than submaximal respiratory data in heart transplant candidates. Circulation 2000;101: 1152-7. 3. Florea VG, Henein MY, Anker SD, et al. Prognostic value of changes over time in exercise capacity and echocardiographic measurements in patients with chronic heart failure. Eur Heart J 2000;21:146-53. 4. Stelken AM, Younis LT, Jennison SH, et al. Prognostic value of cardiopulmonary exercise testing using percent achieved of predicted peak oxygen uptake for patients with ischemic and dilated cardiomyopathy. J Am Coll Cardiol 1996;27:345-52. Journal of Nuclear Cardiology Volume 10, Number 6;644-9 Hacker et al Lack of correlation of right ventricular function and peak oxygen consumption in CHF 5. Aaronson KD, Mancini DM. Is percentage of predicted maximal exercise oxygen consumption a better predictor of survival than peak exercise oxygen consumption for patients with severe heart failure? J Heart Lung Transplant 1995;14:981-9. 6. Roul G, Moulichon ME, Bareiss P, et al. Exercise peak VO2 determination in chronic heart failure: is it still of value? Eur Heart J 1994;15:495-502. 7. Cohn JN, Johnson GR, Shabetai R, et al. Ejection fraction, peak exercise oxygen consumption, cardiothoracic ratio, ventricular arrhythmias, and plasma norepinephrine as determinants of prognosis in heart failure. The V-HeFT VA Cooperative Studies Group. Circulation 1993;87(Suppl 6):VI5-16. 8. Parameshwar J, Keegan J, Sparrow J, Sutton GC, Poole-Wilson PA. Predictors of prognosis in severe chronic heart failure. Am Heart J 1992;123:421-6. 9. Mancini DM, Eisen H, Kussmaul W, et al. Value of peak exercise oxygen consumption for optimal timing of cardiac transplantation in ambulatory patients with heart failure. Circulation 1991;83:778-86. 10. De Groote P, Millaire A, Foucher-Hossein C, et al. Right ventricular ejection fraction is an independent predictor of survival in patients with moderate heart failure. J Am Coll Cardiol 1998;32:948-54. 11. Di Salvo TG, Mathier M, Semigran MJ, Dec GW. Preserved right ventricular ejection fraction predicts exercise capacity and survival in advanced heart failure. J Am Coll Cardiol 1995;25:1143-53. 12. Marving J, Hoilund-Carlsen PF, Chraemmer-Jorgensen B, Gadsboll N. Are right and left ventricular ejection fractions equal? Ejection fractions in normal subjects and in patients with first acute myocardial infarction. Circulation 1985;72:502-14. 13. Johnson LL, Lawson MA, Blackwell GG, et al. Optimizing the method to calculate right ventricular ejection fraction from first- 14. 15. 16. 17. 18. 19. 20. 21. 22. 649 pass data acquired with a multicrystal camera. J Nucl Cardiol 1995;2:372-9. Tausig A, Knesewitsch P, Brinkbaumer K, Tatsch K, Hahn K. Is a low-dose Tc-99m-MIBI protocol suitable for first-pass RNV? Nucl Med Commun 2000;21:965-70. Baker BJ, Wilen MM, Boyd CM, Dinh H, Franciosa JA. Relation of right ventricular ejection fraction to exercise capacity in chronic left ventricular failure. Am J Cardiol 1984;54:596-9. Ben-Gal T, Zafrir N, Pinchas A, et al. Correlation between maximal exercise capacity and right-ventricular function in candidates for heart transplantation. Transplant Proc 2000;32: 743-4. Clark AL, Swan JW, Laney R, et al. The role of right and left ventricular function in the ventilatory response to exercise in chronic heart failure. Circulation 1994;89:2062-9. Szlachcic J, Massie BM, Kramer BL, Topic N, Tubau J. Correlates and prognostic implication of exercise capacity in chronic congestive heart failure. Am J Cardiol 1985;55:1037-42. Maisch B. Ventricular remodeling. Cardiology 1996;87(Suppl 1):2-10. Massie B, Conway M, Yonge R, et al. Skeletal muscle metabolism in patients with congestive heart failure: relation to clinical severity and blood flow. Circulation 1987;76:1009-19. Sullivan MJ, Green HJ, Cobb FR. Skeletal muscle biochemistry and histology in ambulatory patients with long-term heart failure. Circulation 1990;81:518-27. Ghio S, Gavazzi A, Campana C, et al. Independent and additive prognostic value of right ventricular systolic function and pulmonary artery pressure in patients with chronic heart failure. J Am Coll Cardiol 2001;37:183-8.