Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
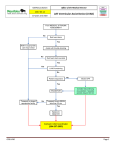
INTERNATIONAL SCHOOL OF CARDIAC SURGERY The management of postinfarction cardiogenic Shock John Pepper Royal Brompton Hospital London Erice, Friday 17th June 2011 Acute heart failure with cardiogenic shock ► Low output syndromes ► Acute decline of pre-existing heart failure ► Acute MI ► Mechanical complications of AMI ► Aortic valve disease: AS/AR ► Prosthetic valve failure ► Acute myocarditis ► Dissection Early Revascularisation in AMI with Cardiogenic Shock [Hochman JS. N.Engl.J.Med. 1999; 341: 625] <75yr >75yr Prior MI No prior MI Mortality: 46.7 vs. 56.0 Difference: -9.3%[95% CI= -20.5 – 1.9%] SHOCK Registry N=884 [ Webb JG. Am.Heart J. 2001; 141: 964] In-hospital mortality Medical PCI CABG P N 499 276 109 Overall 78% 46.4% 23.9% <0.001 1 VD 32.9 33.3 NS 2 VD 42.2 17.7 0.025 3 VD 59.4 29.6 <0.0001 Comparison of PCI and CBG after AMI + Cardiogenic Shock Kaplan-Meier survival estimates at: 96 hours p=0.07 30 days p=0.86 1 year p=0.71 [White HD. Circulation 2005; 112: 1992] Risk factors for CABG in CS [Rastan A. Circulation 2008] ► 2000-2007 ► 302 patients ► Age 69; 76% male ► 42% STEMI ► 30 day M=37.1% ► 1 year survival=50.7% ► Mean survival time 3.2years OR P MV Preop renal 2.3 0.004 * STEMI 1.8 0.013 Lactate >4 3.6 0.001 LVEF<30 % 1.7 0.032 Log EURO >20 19.2 0.004 * * AMI + CS PCI of culprit artery Multivessel PCI Inotropes and fluids IABP No mech.complications YES Adequate support? wean NO wean YES Percut. Short-term LVAD Recovery? Implantable LVAD NO Tx. Mech.complications Adequate support? NO Percut. Short-term LVAD Surgery YES Benefits of LV unloading ► ► ► LVEDP Cardiac work O2 demand ► NB: unload prior to revascularisation ► Pl. adrenaline Pl. Pl. Pl. Pl. Pl. noradrenaline angiotensin ll arg.vasopressin IL6 + IL8 TNFα Haemodynamic criteria LVAD RVAD Cardiac index l.min-1.m2 < 1.8 - 2.0 Systolic AoP mmHg < 90 LAP mmHg > 20 < 15 RAP mmHg < 15 > 25 Short Term Mechanical Circulatory Support Ventricular Assist Devices are very effective in the treatment of severe end-stage cardiac failure However it is particularly difficult to salvage: • Critically ill patients • Postcardiotomy cardiogenic shock LVAD for CS complicating AMI ► 17 studies ► Mean weaning rate = 58.5% ► Mean survival rate = 40% Contraindications to LVAD ► Anticoagulation ► Severe problems AR ► Terminal disease ► CNS injury ► RV failure ► Sepsis ► Severe PVD. Short Term Mechanical Circulatory Support ► Use as a rescue device ► for short term use ► to support one or both sides of the heart ► to treat patients in acute cardiogenic shock ► as a “bridge to decision” when it is unclear whether the patient’s heart will recover or whether the patient will need alternative, longer-term therapies. Short Term Mechanical Circulatory Support ► Reversal of renal and hepatic failure ► Treatment of infection ► Assesssment of neurological function ► Extubation ► Improvement of cardiac dysfunction if possible in moribund patients Short Term Mechanical Circulatory Support ► Bridge to recovery § Acute cardiogenic shock Postcardiotomy Acute myocarditis Right Heart Failure following transplantation ► Bridge to transplant ► Bridge to long term device in very moribund patients Randomised comparison of IABP and LVAD [Thiele H. Eur.Heart J. 2005; 26: 1276] Revascularised AMI with cardiogenic shock RCT in 41 patients Haemodynamic benefit with Tandem 30 day Mortality IABP Tandem LVAD P 45% 42% 0.86 Veno-arterial ECMO for cardiogenic shock [Bakhtiary F. JTCS 2008; 135: 382] Jan 2003 – Nov 2006 N= 45 of 5750 patients undergoing open heart surgery Mean age= 60 35 males Duration of ECMO= 6.4 (+/- 4.5 days) In-hospital Mortality 71% Discharge from Hospital 29% 3 year follow-up 22% Short Term Mechanical Circulatory Support CentriMag® Characteristics ► Magnetic levitation eliminates bearings and seals ► Large mechanical gaps in the pump allow low shear forces reducing haemolysis ► Flow up to 9.9 liters per minute ► Effective at high and low speeds ► Priming volume of 31 ml ► Approved for support for up to 28 days Levitronix: bearing and rotor function Pump Housing Bearingless Centrifugal Pump pump housing Inlet impeller outlet rotor winding stator Peripheral Cannulation Technology Comparison Medos approx. €15000 Thoratec approx € 25000 BVS5000 approx. €9000 IABP approx. €900 CentriMag approx. €5000 Anticoagulation Protocol • No anticoagulation for 6-12 hours • Attempt to normalize coagulation profile • Chest tube drainage < 50 cc/hr for 2 - 3 hrs. • Start heparin infusion, without bolus • Maintain ACT to 150 to 170 secs (PTT 50 secs) Management of LVAD patients Pre-op: LVAD Indications • Deteriorating NHYA Class IV heart failure - with low CO despite appropriate medical Rx (incl inotropes + IABP) - with evidence of secondary organ dysfunction • Early application of LVAD essential BRIDGE TO DECISION F De Robertis et al 2008 Patient demographics N=31 Male Gender 32.4% 37.9% Mean Age y 30 37.6 ± 14.2 IABP 15 Inotropes Ventilated 8 MOF 16 Infection 8 8 Uncertain CNS 3 29.7% RV failure post LVAD implantation OCTx primary failure 1st choice device as "bridge to decision" 100 90 18.9% 43.2% 10.8% 80 70 60 50 40 30 20 10 0 19% Dead Long-term VAD Ongoing survival, % 8.1% total OCTx primary failure RV failure post LVAD 1st choice device as "bridge to decision" TO Transplanted Recovered T1 T2 T3 T4 T5 T6 T7 time, months T8 T9 T10 T11 T12 TandemHeart pVAD ► Removes oxygenated blood from LA via transseptal cannula in the femoral vein ► Returns blood via femoral artery ► Reduces preload ► Increases MAP ► Continuous flow MECHANICAL ASSIST DEVICES DEVICE FLOW l/min REMARKS Impella (Abiomed) Tandem 2.5 Exact positioning 4.0 CC. trans-septal Centrifugal pumps (Biomedicus) 9-10 Rapid insert Centrifugal + ECMO IABP + ECMO 9-10 9-10 Surgery LevitronixCentrimag Up to 9.0 Surgery Acute mitral regurgitation ► Post-inferior myocardial infarct ► Endocarditis ► Trauma ► Acute on chronic Myocardial infarction Local LV remodelling contractility Ischemic mitral regurgitation LAp Pulmonary hypertension Pulmonary edema Volume overload stroke volume Heart failure Death LVEDP wall tension O2 consumption Subendocardial ischemia Mitral valve surgery for acute papillary muscle rupture Author N 30 day 1 year mortality survival % % 5 year survival % Chen Q. 2002 33 21 75 65 Tavakoli R. 2002 21 19 81 68 18.5 [67–8.7] 79 65 Russo A. 54 2008 Cancion System for Continuous Aortic Flow Augmentation (CAFA) Patient Prognosis in Heart Failure Axial impellor LVAD: continuous flow [Henein M.et al. Circulation 2002; 105: 2324] HeartMate II CentriMag® MagLev Ventricular Assist System: Pump Console Motor Clinical Advantages with CentriMag VAS Ø Versatile: LVAD, RVAD, BIVAD, ECMO Ø Easy device insertion - Can be inserted without cardiopulmonary bypass Ø Minimal anticoagulation requirement, (less vulnerable to thrombus & embolic complications) Ø Gives adequate flow Ø Maximizes potential for recovery Ø Minimal blood trauma, minimal haemolysis Ø Transportable Ø Costs acceptable Short Term Mechanical Circulatory Conclusions Support(1) ► Easy device insertion § Can be inserted without cardiopulmonary bypass ► Only requires moderate levels of anticoagulation ► Gives adequate flow ► Costs acceptable Allows ► Reversal of renal and hepatic failure ► Treatment of infection ► Assesssment of neurological function ► Extubation ► Improvement of cardiac dysfunction if possible In moribund patients to optimise them prior to insertion of a longer term device Short Term Mechanical Circulatory Support Conclusions (2) Useful for ► “Bridge to decision” § Acute cardiogenic shock ► Bridge to recovery - Postcardiotomy - Acute myocarditis - Right Heart Failure following transplantation ► Bridge to transplant What was this operation ? PVE: what are likely organisms? Thank you Levitronix for End Stage Cardiac Failure ® CentriMag ICU Support Transport on LVAD