Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
®
Leading the way in iron replacement therapy
There is no replacement for
experience.
Leading the way in iron
replacement therapy
There’s no replacement for options
Treatment options to meet the needs of your patients
A trusted name in iron replacement for 20 years
Millions of patients treated with American Regent iron replacement products
Single dose of 2 or
more doses
Broadly available for a range of patients in the outpatient and inpatient settings
Indication
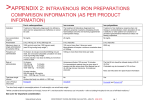
Injectafer®
(ferric carboxymaltose
injection)
Venofer®
(iron sucrose
injection, USP)
Recommended
cumulative doses
Number of
administrations
for recommended
cumulative dose
(for non-dialysis
dependent CKD)
Iron deficiency anemia (IDA) in adult patients who
have non-dialysis dependent chronic kidney disease
(NDD-CKD)
IDA in patients with peritoneal-dialysis dependent
(PDD) or hemodialysis dependent (HDD) CKD
IV push
Injectafer
Venofer
750 mg (2 doses separated by at
least 7 days)†‡
100 mg to 400 mg, depending
upon the indication
Total cumulative dose not to
exceed 1500 mg of iron per course
Usual total treatment course is
1000 mg
(maximum dose)
Yes
IDA in adult patients who have intolerance to oral
iron or have had unsatisfactory response to oral iron
Indicated for pediatric patients (age 2 years
and older) with HDD-CKD for iron maintenance
treatment or with NDD-CKD or PDD-CKD who are
on erythropoietin therapy for iron maintenance
treatment
Dextran-free IV iron
SELECTED SAFETY INFORMATION FOR INJECTAFER
WARNINGS AND PRECAUTIONS
2
Serious hypersensitivity reactions, including anaphylactic-type reactions, some of which have been lifethreatening and fatal, have been reported in patients receiving Injectafer. Patients may present with
shock, clinically significant hypotension, loss of consciousness, and/or collapse. Monitor patients for signs
and symptoms of hypersensitivity during and after Injectafer administration for at least 30 minutes and
until clinically stable following completion of the infusion. Only administer Injectafer when personnel and
therapies are immediately available for the treatment of serious hypersensitivity reactions.
to
IV infusion
IDA of various etiologies, which may include*:
–GI disorders
–OB/GYN disorders
–Cancer
–Heart failure
–Post-gastric bypass
Yes
Yes, over at least 15 minutes
to
Yes, over 15 minutes to 2.5 hours,
depending on dose
SELECTED SAFETY INFORMATION FOR VENOFER
WARNINGS AND PRECAUTIONS
Serious hypersensitivity reactions, including anaphylactic-type reactions, some of which have been lifethreatening and fatal, have been reported in patients receiving Venofer. Patients may present with shock,
clinically significant hypotension, loss of consciousness, and/or collapse. If hypersensitivity reactions or
signs of intolerance occur during administration, stop Venofer immediately. Monitor patients for signs and
symptoms of hypersensitivity during and after Venofer administration for at least 30 minutes and until
clinically stable following completion of the infusion. Only administer Venofer when personnel and therapies
are immediately available for the treatment of serious hypersensitivity reactions. Most reactions associated
with intravenous iron preparations occur within 30 minutes of the completion of the infusion.
*Injectafer and Venofer are not indicated to treat these conditions.
For adult patients weighing less than 50 kg (110 lb), give each dose as 15 mg/kg body weight
for a total cumulative dose not to exceed 1500 mg of iron per course of treatment.
†
When administered via IV infusion, dilute up to 750 mg of iron in no more than 250 mL of
sterile 0.9% sodium chloride injection, USP, such that the concentration of the infusion is not
<2 mg of iron per mL and administer over at least 15 minutes. When administered as a slow IV
push, give at the rate of approximately 100 mg (2 mL) per minute.
‡
Please see attached Full Prescribing Information for Injectafer and Venofer.
3
An outpatient case for Injectafer®
Robin’s* inflammatory bowel disease may have
impaired the absorption of her oral iron therapy
Name/age
Diagnosis
Weight
Medication
history
LAB RESULTS
Hb
10.5 g/dL
Robin H, 41
Ferritin
15.8 ng/mL
IDA secondary to inflammatory bowel disease
TSAT
11.6%
159 lb/72.1 kg
Although Robin was fully compliant with her course of oral iron therapy
(ferrous sulfate, 325 mg TID), her Hb level only increased by 0.5 g/dL
The #1 IV iron in oncology and
gastroenterology clinics†
Only Injectafer provides up to 1500 mg of iron in just
2 administrations of up to 750 mg, separated by at
least 7 days‡
Two administration options—IV infusion or slow
IV push§
The ONLY dextran-free IV iron for adult patients with
IDA from etiologies other than CKD
An inpatient case for Venofer®
72-hour stability
When added to an infusion bag containing 0.9%
sodium chloride injection, USP, at concentrations
ranging from 2 mg to 4 mg of iron per mL, Injectafer
solution is physically and chemically stable for
72 hours when stored at room temperature
To maintain stability, do not dilute to concentrations
less than 2 mg iron/mL
Michael* is a CKD patient who was hospitalized after
experiencing complications
Name/age
Diagnosis
Weight
Iron
replacement
therapy
LAB RESULTS
Hb
9.8 g/dL
Michael A, 72
Ferritin
88.0 ng/mL
Chronic kidney disease and IDA. Patient was admitted to the
hospital after experiencing shortness of breath, swelling in
his legs, and persistent wheezing
TSAT
17.4%
166 lb/75.3 kg
Scheduled to receive an IV iron replacement goal of 1000 mg in divided doses, each
administered as an IV push to minimize fluid intake
The top selling IV iron in the US every year since 2003º
Over 20 million patients treated with over 417 million units prescribed worldwide¶
Wide formulary acceptance for in-hospital use
Multiple dosage strengths and dosing options available
May be administered as a slow IV push over 2-5 minutes
Stable for 7 days
Up to 50% more iron (1500 mg) in the form of Injectafer may be administered
in only 2 administrations
Compared with iron sucrose, which has a recommended cumulative dose of 1000 mg in
5 administrations in patients with NDD-CKD over a 14-day period
*Note: The individuals depicted in this brochure are fictional and for illustrative purposes only.
†
Syringe stability: When diluted with 0.9% NaCl at concentrations ranging from 2 mg to 10 mg of elemental
iron per mL, or undiluted (20 mg elemental iron per mL) and stored in a plastic syringe, has been found
to be physically and chemically stable for 7 days at controlled room temperature (25°C ± 2°C) and under
refrigeration (4°C ± 2°C)
Intravenous admixture stability: When added to intravenous infusion bags (PVC or non-PVC) containing 0.9%
NaCl at concentrations ranging from 1 mg to 2 mg of elemental iron per mL, has been found to be physically
and chemically stable for 7 days at controlled room temperature (25°C ± 2°C)
Based on IMS DDD MG Sales (July 2015 to December 2015).
For adult patients weighing less than 50 kg (110 lb), give each dose as 15 mg/kg body weight for a total cumulative dose not to exceed 1500 mg of
iron per course of treatment.
‡
When administered via IV infusion, dilute up to 750 mg of iron in no more than 250 mL of sterile 0.9% sodium chloride injection, USP, such that the
concentration of the infusion is not <2 mg of iron per mL and administer over at least 15 minutes. When administered as a slow IV push, give at the
rate of approximately 100 mg (2 mL) per minute.
§
º
¶
IMS Health Sales Data 2003-2015.
Data on file. PSUR (Periodic Safety Update Report), February 2016. Luitpold Pharmaceuticals, Inc. Shirley, NY.
ADVERSE REACTIONS
ADVERSE REACTIONS
The most common adverse reactions (≥2%) following the administration of Venofer are diarrhea, nausea,
vomiting, headache, dizziness, hypotension, pruritus, pain in extremity, arthralgia, back pain, muscle cramp,
injection site reactions, chest pain and peripheral edema. Additional adverse reactions include infusion site pain
or burning, graft complications, and nasopharyngitis, sinusitis, upper respiratory tract infections and pharyngitis.
In two randomized clinical studies, a total of 1775 patients were exposed to Injectafer, 15 mg/kg of body weight,
up to a single maximum dose of 750 mg of iron on two occasions, separated by at least 7 days, up to a cumulative
dose of 1500 mg of iron. Adverse reactions reported by ≥2% of Injectafer-treated patients were nausea (7.2%);
hypertension (3.8%); flushing/hot flush (3.6%); blood phosphorus decrease (2.1%); and dizziness (2.0%).
In pediatric patients, more than 50% of the patients experienced at least one treatment-emergent reaction. The
most common adverse reactions (≥2%) were headache, respiratory tract viral infection, peritonitis, vomiting,
pyrexia, dizziness, cough, renal transplant, nausea, arteriovenous fistula thrombosis,
hypotension and hypertension.
The following serious adverse reactions have been most commonly reported from the post-marketing
spontaneous reports: urticaria, dyspnea, pruritus, tachycardia, erythema, pyrexia, chest discomfort, chills,
angioedema, back pain, arthralgia, and syncope.
Injection site discoloration has been reported following extravasation. Assure
stable intravenous access to avoid extravasation.
SELECTED SAFETY INFORMATION FOR INJECTAFER
4
SELECTED SAFETY INFORMATION FOR VENOFER
Please see attached Full Prescribing Information for Injectafer and Venofer.
5
INDICATIONS
Injectafer (ferric carboxymaltose injection) is
an iron replacement product indicated for the
treatment of iron deficiency anemia in adult
patients who have intolerance to oral iron or have
had unsatisfactory response to oral iron, and in
adult patients with non-dialysis dependent chronic
kidney disease.
®
IMPORTANT SAFETY
INFORMATION
CONTRAINDICATIONS
Injectafer is contraindicated in patients with
hypersensitivity to Injectafer or any of its inactive
components.
WARNINGS AND PRECAUTIONS
Serious hypersensitivity reactions, including
anaphylactic-type reactions, some of which
have been life-threatening and fatal, have
been reported in patients receiving Injectafer.
Patients may present with shock, clinically
significant hypotension, loss of consciousness,
and/or collapse. Monitor patients for signs
and symptoms of hypersensitivity during and
after Injectafer administration for at least 30
minutes and until clinically stable following
completion of the infusion. Only administer
Injectafer when personnel and therapies are
immediately available for the treatment of
serious hypersensitivity reactions. In clinical trials,
serious anaphylactic/anaphylactoid reactions were
reported in 0.1% (2/1775) of subjects receiving
Injectafer. Other serious or severe adverse reactions
potentially associated with hypersensitivity which
included, but were not limited to, pruritus, rash,
urticaria, wheezing, or hypotension were reported
in 1.5% (26/1775) of these subjects.
In clinical studies, hypertension was reported in
3.8% (67/1775) of subjects. Transient elevations in
systolic blood pressure, sometimes occurring with
facial flushing, dizziness, or nausea were observed
in 6% (106/1775) of subjects. These elevations
generally occurred immediately after dosing and
resolved within 30 minutes. Monitor patients for
signs and symptoms of hypertension following each
Injectafer administration.
INDICATION
Venofer® (iron sucrose injection, USP) is indicated
for the treatment of iron deficiency anemia in
patients with chronic kidney disease.
In the 24 hours following administration of
Injectafer, laboratory assays may overestimate
serum iron and transferrin bound iron by also
measuring the iron in Injectafer.
IMPORTANT SAFETY
INFORMATION
ADVERSE REACTIONS
Venofer is contraindicated in patients with known
hypersensitivity to Venofer.
In two randomized clinical studies, a total of 1775
patients were exposed to Injectafer, 15 mg/kg of
body weight, up to a single maximum dose of 750
mg of iron on two occasions, separated by at least
7 days, up to a cumulative dose of 1500 mg of iron.
Adverse reactions reported by ≥2% of Injectafertreated patients were nausea (7.2%); hypertension
(3.8%); flushing/hot flush (3.6%); blood phosphorus
decrease (2.1%); and dizziness (2.0%).
The following serious adverse reactions have been
most commonly reported from the post-marketing
spontaneous reports: urticaria, dyspnea, pruritus,
tachycardia, erythema, pyrexia, chest discomfort,
chills, angioedema, back pain, arthralgia,
and syncope.
To report adverse events, please contact American Regent at 1-800-734-9236. You may
also contact the FDA at www.fda.gov/medwatch or 1-800-FDA-1088.
Please see attached Full Prescribing Information for Injectafer and Venofer.
6
ADVERSE REACTIONS
CONTRAINDICATIONS
WARNINGS AND PRECAUTIONS
Serious hypersensitivity reactions, including
anaphylactic-type reactions, some of which
have been life-threatening and fatal, have been
reported in patients receiving Venofer. Patients
may present with shock, clinically significant
hypotension, loss of consciousness, and/or
collapse. If hypersensitivity reactions or signs
of intolerance occur during administration,
stop Venofer immediately. Monitor patients for
signs and symptoms of hypersensitivity during
and after Venofer administration for at least
30 minutes and until clinically stable following
completion of the infusion. Only administer
Venofer when personnel and therapies are
immediately available for the treatment of
serious hypersensitivity reactions. Most reactions
associated with intravenous iron preparations occur
within 30 minutes of the completion of the infusion.
Venofer may cause clinically significant hypotension.
Monitor for signs and symptoms of hypotension
following each administration of Venofer.
Hypotension following administration of Venofer
may be related to rate of administration and/or total
dose delivered.
Excessive therapy with parenteral iron can lead
to excess storage of iron with the possibility of
iatrogenic hemosiderosis. All adult and pediatric
patients receiving Venofer require periodic
monitoring of hematologic and iron parameters
(hemoglobin, hematocrit, serum ferritin and
transferrin saturation). Do not administer Venofer to
patients with evidence of iron overload. Transferrin
saturation (TSAT) values increase rapidly after
intravenous administration of iron sucrose; do not
perform serum iron measurements for at least
48 hours after intravenous dosing.
The most common adverse reactions (≥2%)
following the administration of Venofer are diarrhea,
nausea, vomiting, headache, dizziness, hypotension,
pruritus, pain in extremity, arthralgia, back pain,
muscle cramp, injection site reactions, chest
pain and peripheral edema. Additional adverse
reactions include infusion site pain or burning, graft
complications, and nasopharyngitis, sinusitis, upper
respiratory tract infections and pharyngitis.
In pediatric patients, more than 50% of the patients
experienced at least one treatment-emergent
reaction. The most common adverse reactions
(≥2%) were headache, respiratory tract viral
infection, peritonitis, vomiting, pyrexia, dizziness,
cough, renal transplant, nausea, arteriovenous
fistula thrombosis, hypotension and hypertension.
In post-marketing safety studies of Venofer in
1,051 patients with HDD-CKD, adverse reactions
reported by >1% were cardiac failure congestive,
sepsis and dysgeusia.
Because adverse reactions from post-marketing
experience are reported voluntarily from a
population of uncertain size, it is not always
possible to reliably estimate their frequency or
establish a causal relationship to drug exposure.
In addition to potential serious hypersensitivity
reactions, the following adverse reactions have
been identified during post-approval use of
Venofer: bronchospasm, dyspnea, convulsions,
light-headedness, confusion, angioedema, swelling
of the joints, hyperhidrosis, bradycardia and
chromaturia.
Symptoms associated with Venofer total dosage or
infusing too rapidly included hypotension, dyspnea,
headache, vomiting, nausea, dizziness, joint
aches, paresthesia, abdominal and muscle pain,
edema and cardiovascular collapse. These adverse
reactions have occurred up to 30 minutes after the
administration of Venofer injections. Reactions have
occurred following the first dose or subsequent
doses of Venofer. Slowing the infusion rate may
alleviate symptoms.
Injection site discoloration has been reported
following extravasation. Assure stable intravenous
access to avoid extravasation.
7
®
Trusted options for your adult IDA patients
Which option is appropriate
for your patients?
The #1 IV iron in oncology and
gastroenterology clinics*
Over a decade of clinical
experience‡
The only dextran-free IV iron for adult patients
with IDA from etiologies other than CKD
Over 7500 patients treated in clinical
trials worldwide†
The market leader for the treatment of IDA in
CKD (dialysis and non-dialysis dependent)
Consistently the #1 selling IV iron in the US§
Wide formulary acceptance for
in-hospital use
Approved in 70 countries worldwide†
INDICATIONS FOR INJECTAFER®
Injectafer is an iron replacement product
indicated for the treatment of iron deficiency
anemia in adult patients:
who have intolerance to or have had
unsatisfactory response to oral iron or
who have non-dialysis dependent chronic
kidney disease
INDICATION FOR VENOFER®
Venofer is indicated for the treatment of iron
deficiency anemia in patients with chronic kidney
disease.
CONTRAINDICATIONS FOR VENOFER
Venofer is contraindicated in patients with known
hypersensitivity to Venofer.
CONTRAINDICATIONS FOR INJECTAFER
Injectafer is contraindicated in patients with
hypersensitivity to Injectafer or any of its
inactive components.
*Based on IMS DDD MG Sales (July 2015 to December 2015).
†
Data on file. PSUR (Periodic Safety Update Report), February 2016. Luitpold Pharmaceuticals, Inc. Shirley, NY.
‡
Initial US approval: 2000.
§
Data on file. IMS Sales Data 2003-2015.
Please see attached Full Prescribing Information and the Important Safety Information inside for
Injectafer and Venofer.
American Regent ® is a registered trademark of Luitpold Pharmaceuticals, Inc. Injectafer ® and the Injectafer ® logo are trademarks of Vifor (International), Inc.,
Switzerland. Venofer ® and the Venofer ® logo are trademarks of Vifor (International), Inc., Switzerland. Injectafer ® and Venofer ® are manufactured under license
from Vifor (International), Inc., Switzerland.
©2016 American Regent, Inc. PP-IN-US-0015 Iss. 4/2016
INJECTAFER®
(ferric carboxymaltose injection)
RQ105200
1
INDICATIONS AND USAGE
Injectafer is indicated for the treatment of iron deficiency anemia in adult
patients:
• who have intolerance to oral iron or have had unsatisfactory response to
oral iron;
• who have non-dialysis dependent chronic kidney disease.
2
DOSAGE AND ADMINISTRATION
For patients weighing 50 kg (110lb) or more: Give Injectafer in two doses
separated by at least 7 days. Give each dose as 750 mg for a total cumulative
dose not to exceed 1500 mg of iron per course.
For patients weighing less than 50 kg (110lb): Give Injectafer in two doses
separated by at least 7 days. Give each dose as 15 mg/kg body weight for a
total cumulative dose not to exceed 1500 mg of iron per course.
The dosage of Injectafer is expressed in mg of elemental iron. Each mL of
Injectafer contains 50 mg of elemental iron. Injectafer treatment may be
repeated if iron deficiency anemia reoccurs.
Administer Injectafer intravenously, either as an undiluted slow intravenous
push or by infusion. When administering as a slow intravenous push, give at
the rate of approximately 100 mg (2 mL) per minute. When administered via
infusion, dilute up to 750 mg of iron in no more than 250 mL of sterile 0.9%
sodium chloride injection, USP, such that the concentration of the infusion is
not less than 2 mg of iron per mL and administer over at least 15 minutes.
When added to an infusion bag containing 0.9% sodium chloride injection,
USP, at concentrations ranging from 2 mg to 4 mg of iron per mL, Injectafer
solution is physically and chemically stable for 72 hours when stored at room
temperature. To maintain stability, do not dilute to concentrations less than
2 mg iron/mL.
Inspect parenteral drug products visually for the absence of particulate
matter and discoloration prior to administration. The product contains no
preservatives. Each vial of Injectafer is intended for single-use only. Any
unused drug remaining after injection must be discarded.
Avoid extravasation of Injectafer since brown discoloration of the extravasation
site may be long lasting. Monitor for extravasation. If extravasation occurs,
discontinue the Injectafer administration at that site.
3
In clinical trials, serious anaphylactic/anaphylactoid reactions were reported
in 0.1% (2/1775) of subjects receiving Injectafer. Other serious or severe
adverse reactions potentially associated with hypersensitivity which included,
but not limited to, pruritus, rash, urticaria, wheezing, or hypotension were
reported in 1.5% (26/1775) of these subjects.
5.2 Hypertension
In clinical studies, hypertension was reported in 3.8% (67/1,775) of subjects
in clinical trials 1 and 2. Transient elevations in systolic blood pressure,
sometimes occurring with facial flushing, dizziness, or nausea were observed
in 6% (106/1,775) of subjects in these two clinical trials. These elevations
generally occurred immediately after dosing and resolved within 30 minutes.
Monitor patients for signs and symptoms of hypertension following each
Injectafer administration [see Dosage and Administration (2)].
5.3 Laboratory Test Alterations
In the 24 hours following administration of Injectafer, laboratory assays may
overestimate serum iron and transferrin bound iron by also measuring the
iron in Injectafer.
6
ADVERSE REACTIONS
The following adverse reactions are discussed in greater detail in other
sections of the labeling:
• Hypersensitivity Reactions [see Warnings and Precautions (5.1)]
• Hypertension [see Warnings and Precautions (5.2)]
• Laboratory Test Alterations [see Warnings and Precautions (5.3)]
6.1 Adverse Reactions in Clinical Trials
Because clinical trials are conducted under widely varying conditions, the
adverse reaction rates observed cannot be directly compared to rates in other
clinical trials and may not reflect the rates observed in clinical practice.
In two randomized clinical studies [Studies 1 and 2, See Clinical Studies (14)],
a total of 1,775 patients were exposed to Injectafer 15 mg/kg body weight up
to a maximum single dose of 750 mg of iron on two occasions separated by
at least 7 days up to a cumulative dose of 1500 mg of iron.
Adverse reactions reported by ≥ 1% of treated patients are shown in the
following table.
Table 1. Adverse reactions reported in ≥ 1% of Study Patients in Clinical Trials
1 and 2
Term
DOSAGE FORMS AND STRENGTHS
750 mg iron / 15 mL single-use vial
4
CONTRAINDICATIONS
Nausea
Hypertension
Flushing/Hot Flush
Blood Phosphorus Decrease
Dizziness
Vomiting
Injection Site Discoloration
Headache
Alanine Aminotransferase
Increase
Dysgeusia
Hypotension
Constipation
Hypersensitivity to Injectafer or any of its components [see Warnings and
Precautions (5.1)].
5
DRUG INTERACTIONS
*Sections or subsections omitted from the full prescribing information
are not listed.
FULL PRESCRIBING INFORMATION
WARNINGS AND PRECAUTIONS
5.1 Hypersensitivity Reactions
Serious hypersensitivity reactions, including anaphylactic-type reactions,
some of which have been life-threatening and fatal, have been reported in
patients receiving Injectafer. Patients may present with shock, clinically
significant hypotension, loss of consciousness, and/or collapse. Monitor
patients for signs and symptoms of hypersensitivity during and after
Injectafer administration for at least 30 minutes and until clinically stable
following completion of the infusion. Only administer Injectafer when
personnel and therapies are immediately available for the treatment of
serious hypersensitivity reactions. [see Adverse Reactions (6.1 and 6.2)].
a
Other adverse reactions reported by ≥ 0.5% of treated patients include
abdominal pain, diarrhea, gamma glutamyl transferase increased, injection
site pain/irritation, rash, paraesthesia, sneezing. Transient decreases in
laboratory blood phosphorus levels (< 2 mg/dL) have been observed in 27%
(440/1638) patients in clinical trials.
6.2 Post-marketing Experience
Because these reactions are reported voluntarily from a population of uncertain
size, it is not always possible to reliably estimate their frequency or establish a
causal relationship to drug exposure. The following serious adverse reactions
have been most commonly reported from the post-marketing spontaneous
reports with Injectafer: urticaria, dyspnea, pruritis, tachycardia, erythema,
pyrexia, chest discomfort, chills, angioedema, back pain, arthralgia, and
syncope. One case of hypophosphatemic osteomalacia was reported in
a subject who received 500 mg of Injectafer every 2 weeks for a total of
16 weeks. Partial recovery followed discontinuation of Injectafer.
Injectafer
Pooled
Comparatorsa
Oral
iron
(N=1775)
%
7.2
3.8
3.6
2.1
2.0
1.7
1.4
1.2
(N=1783)
%
1.8
1.9
0.2
0.1
1.2
0.5
0.3
0.9
(N=253)
%
1.2
0.4
0.0
0.0
0.0
0.4
0.0
0.0
1.1
0.2
0.0
1.1
1.0
0.5
2.1
1.9
0.9
0.0
0.0
3.2
7
DRUG INTERACTIONS
Formal drug interaction studies have not been performed with Injectafer.
8
USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Pregnancy Category C
Risk Summary
Adequate and well controlled studies in pregnant women have not been
conducted. However, animal reproduction studies have been conducted with
ferric carboxymaltose. In these studies, administration of ferric carboxymaltose
to rabbits during the period of organogenesis caused fetal malformations and
increased implantation loss at maternally toxic doses of approximately 12%
to 23% of the human weekly dose of 750 mg (based on body surface area).
The incidence of major malformations in human pregnancies has not been
established for Injectafer. However, all pregnancies, regardless of exposure to
any drug, has a background rate of 2 to 4% for major malformations, and 15
to 20% for pregnancy loss. Injectafer should be used during pregnancy only if
the potential benefit justifies the potential risk to the fetus.
Animal Data
Administration of ferric carboxymaltose to rats as a one-hour intravenous
infusion up to 30 mg/kg/day iron on gestation days 6 to 17 did not result in
adverse embryofetal findings. This daily dose in rats is approximately 40%
of the human weekly dose of 750 mg based on body surface area. In rabbits,
ferric carboxymaltose was administered as a one-hour infusion on gestation
days 6 to 19 at iron doses of 4.5, 9, 13.5, and 18 mg/kg/day. Malformations
were seen starting at the daily dose of 9 mg/kg (23% of the human weekly
dose of 750 mg). Spontaneous abortions occurred starting at the daily iron
dose of 4.5 mg/kg (12% of the human weekly dose based on body surface
area). Pre-implantation loss was at the highest dose. Adverse embryofetal
effects were observed in the presence of maternal toxicity.
A pre- and post-natal development study was conducted in rats at intravenous
doses up to 18 mg/kg/day of iron (approximately 23% of the weekly human
dose of 750 mg on a body surface area basis). There were no adverse effects
on survival of offspring, their behavior, sexual maturation or reproductive
parameters.
8.3 Nursing Mothers
A study to determine iron concentrations in breast milk after administration of
Injectafer (n=11) or oral ferrous sulfate (n=14) was conducted in 25 lactating
women with postpartum iron deficiency anemia. Mean breast milk iron levels
were higher in lactating women receiving Injectafer than in lactating women
receiving oral ferrous sulfate.
8.4 Pediatric Use
Safety and effectiveness have not been established in pediatric patients.
8.5 Geriatric Use
Of the 1775 subjects in clinical studies of Injectafer, 50% were 65 years and
over, while 25% were 75 years and over. No overall differences in safety or
effectiveness were observed between these subjects and younger subjects,
and other reported clinical experience has not identified differences in
responses between the elderly and younger patients, but greater sensitivity of
some older individuals cannot be ruled out.
10 OVERDOSAGE
Excessive dosages of Injectafer may lead to accumulation of iron in storage
sites potentially leading to hemosiderosis. A patient who received Injectafer
18,000 mg over 6 months developed hemosiderosis with multiple joint
disorder, walking disability and asthenia . Hypophosphatemic osteomalacia
was reported in a patient who received Injectafer 4000 mg over 4 months.
Partial recovery followed discontinuation of Injectafer. [see Post-marketing
Experience (6.2)].
11
DESCRIPTION
Ferric carboxymaltose, an iron replacement product, is an iron carbohydrate
complex with the chemical name of polynuclear iron (III) hydroxide
4(R)-(poly-(1→4)-O-a-D-glucopyranosyl)-oxy-2(R),3(S),5(R),6tetrahydroxy-hexanoate. It has a relative molecular weight of approximately
150,000 Da corresponding to the following empirical formula:
[FeOx(OH)y(H2O)z]n [{(C6H10O5)m (C6H12O7)}l]k,
where n ≈ 103, m ≈ 8, l≈ 11, and k ≈ 4
(l represents the mean branching degree of the ligand).
The chemical structure is presented below:
Includes oral iron and all formulations of IV iron other than Injectafer
651 S ML King Jr Ave • Waukegan, IL 60085 • Phone 847.336.4200 • Fax 847.360.4924
complete packaging | individual solutionsSM
INJECTAFER®
(ferric carboxymaltose injection)
Other adverse reactions reported by ≥ 0.5% of treated patients include
abdominal pain, diarrhea, gamma glutamyl transferase increased, injection
site pain/irritation, rash, paraesthesia, sneezing. Transient decreases in
laboratory blood phosphorus levels (< 2 mg/dL) have been observed in 27%
(440/1638) patients in clinical trials.
6.2 Post-marketing Experience
Because these reactions are reported voluntarily from a population of uncertain
size, it is not always possible to reliably estimate their frequency or establish a
causal relationship to drug exposure. The following serious adverse reactions
have been most commonly reported from the post-marketing spontaneous
reports with Injectafer: urticaria, dyspnea, pruritis, tachycardia, erythema,
pyrexia, chest discomfort, chills, angioedema, back pain, arthralgia, and
syncope. One case of hypophosphatemic osteomalacia was reported in
a subject who received 500 mg of Injectafer every 2 weeks for a total of
16 weeks. Partial recovery followed discontinuation of Injectafer.
7
8
USE IN SPECIFIC POPULATIONS
6
INDICATIONS AND USAGE
DOSAGE AND ADMINISTRATION
DOSAGE FORMS AND STRENGTHS
CONTRAINDICATIONS
WARNINGS AND PRECAUTIONS
5.1 Hypersensitivity Reactions
5.2 Hypertension
5.3 Laboratory Test Alterations
ADVERSE REACTIONS
6.1 Adverse Reactions in Clinical Trials
6.2 Post-marketing Experience
DRUG INTERACTIONS
USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
8.3 Nursing Mothers
8.4 Pediatric Use
8.5 Geriatric Use
7
10 OVERDOSAGE
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
12.2 Pharmacodynamics
12.3 Pharmacokinetics
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, and Impairment of Fertility
14 CLINICAL STUDIES
14.1 Trial 1: Iron Deficiency Anemia in Patients Who are Intolerant to
Oral Iron or Have Had Unsatisfactory Response to Oral Iron
14.2 Trial 2: Iron Deficiency Anemia in Patients with Non-Dialysis
Dependent Chronic Kidney Disease
16 HOW SUPPLIED/STORAGE AND HANDLING
17 PATIENT COUNSELING INFORMATION
1
2
3
4
5
Formal drug interaction studies have not been performed with Injectafer.
FULL PRESCRIBING INFORMATION: CONTENTS*
8
--------------------------DOSAGE FORMS AND STRENGTHS----------------------750 mg iron / 15 mL single-use vial. (3)
-------------------------------CONTRAINDICATIONS--------------------------------Hypersensitivity to Injectafer or any of its inactive components. (4)
------------------------WARNINGS AND PRECAUTIONS---------------------------• Hypersensitivity reactions: Observe for signs and symptoms of
hypersensitivity during and after Injectafer administration for at least
30 minutes and until clinically stable following completion of each
administration. (5.1)
• Hypertension: Monitor patients closely for signs and symptoms of
hypertension following each Injectafer administration. (5.2)
------------------------------ADVERSE REACTIONS---------------------------------The most common adverse reactions (≥ 2%) are nausea, hypertension,
flushing, hypophosphatemia, and dizziness (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact American Regent at
1-800-734-9236 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
------------------------USE IN SPECIFIC POPULATIONS---------------------------• Nursing Mothers: Exercise caution when administered to a nursing
woman. (8.3)
See 17 for PATIENT COUNSELING INFORMATION and FDA-approved
patient labeling.
Revised: July 2013
8.1 Pregnancy
Pregnancy Category C
Risk Summary
Adequate and well controlled studies in pregnant women have not been
conducted. However, animal reproduction studies have been conducted with
ferric carboxymaltose. In these studies, administration of ferric carboxymaltose
to rabbits during the period of organogenesis caused fetal malformations and
increased implantation loss at maternally toxic doses of approximately 12%
to 23% of the human weekly dose of 750 mg (based on body surface area).
The incidence of major malformations in human pregnancies has not been
established for Injectafer. However, all pregnancies, regardless of exposure to
any drug, has a background rate of 2 to 4% for major malformations, and 15
to 20% for pregnancy loss. Injectafer should be used during pregnancy only if
the potential benefit justifies the potential risk to the fetus.
Animal Data
Administration of ferric carboxymaltose to rats as a one-hour intravenous
infusion up to 30 mg/kg/day iron on gestation days 6 to 17 did not result in
adverse embryofetal findings. This daily dose in rats is approximately 40%
of the human weekly dose of 750 mg based on body surface area. In rabbits,
ferric carboxymaltose was administered as a one-hour infusion on gestation
days 6 to 19 at iron doses of 4.5, 9, 13.5, and 18 mg/kg/day. Malformations
were seen starting at the daily dose of 9 mg/kg (23% of the human weekly
dose of 750 mg). Spontaneous abortions occurred starting at the daily iron
dose of 4.5 mg/kg (12% of the human weekly dose based on body surface
area). Pre-implantation loss was at the highest dose. Adverse embryofetal
effects were observed in the presence of maternal toxicity.
A pre- and post-natal development study was conducted in rats at intravenous
doses up to 18 mg/kg/day of iron (approximately 23% of the weekly human
dose of 750 mg on a body surface area basis). There were no adverse effects
on survival of offspring, their behavior, sexual maturation or reproductive
parameters.
8.3 Nursing Mothers
A study to determine iron concentrations in breast milk after administration of
Injectafer (n=11) or oral ferrous sulfate (n=14) was conducted in 25 lactating
women with postpartum iron deficiency anemia. Mean breast milk iron levels
were higher in lactating women receiving Injectafer than in lactating women
receiving oral ferrous sulfate.
Other adverse reactions reported by ≥ 0.5% of treated patients include
8.4 Pediatric Use
abdominal pain, diarrhea, gamma glutamyl transferase increased, injection
Safety and effectiveness have not been established in pediatric patients.
site pain/irritation, rash, paraesthesia, sneezing. Transient decreases in
8.5
Geriatric
laboratory
bloodUse
phosphorus levels (< 2 mg/dL) have been observed in 27%
Of
the 1775patients
subjectsininclinical
clinicaltrials.
studies of Injectafer, 50% were 65 years and
(440/1638)
over, while 25% were 75 years and over. No overall differences in safety or
6.2 Post-marketing Experience
effectiveness were observed between these subjects and younger subjects,
Because these reactions are reported voluntarily from a population of uncertain
and other reported clinical experience has not identified differences in
size, it is not always possible to reliably estimate their frequency or establish a
responses between the elderly and younger patients, but greater sensitivity of
causal relationship to drug exposure. The following serious adverse reactions
some older individuals cannot be ruled out.
HIGHLIGHTS OF PRESCRIBING INFORMATION
These highlights do not include all the information needed to use
Injectafer safely and effectively. See full prescribing information for
Injectafer.
INJECTAFER® (ferric carboxymaltose injection)
For intravenous use
Initial U.S. Approval: 2013
------------------------------INDICATIONS AND USAGE-----------------------------Injectafer is an iron replacement product indicated for the treatment of iron
deficiency anemia in adult patients:
• who have intolerance to oral iron or have had unsatisfactory response to
oral iron;
• who have non-dialysis dependent chronic kidney disease.
-------------------------DOSAGE AND ADMINISTRATION--------------------------For patients weighing 50 kg (110lb) or more: Give Injectafer in two
doses separated by at least 7 days. Give each dose as 750 mg for a total
cumulative dose of 1500 mg of iron per course.
For patients weighing less than 50 kg (110lb): Give Injectafer in two doses
separated by at least 7 days and give each dose as 15 mg/kg body weight.
Injectafer treatment may be repeated if iron deficiency anemia reoccurs. (2)
RQ105200
--------------------------DOSAGE FORMS AND STRENGTHS----------------------750 mg iron / 15 mL single-use vial. (3)
-------------------------------CONTRAINDICATIONS--------------------------------Hypersensitivity to Injectafer or any of its inactive components. (4)
------------------------WARNINGS AND PRECAUTIONS---------------------------• Hypersensitivity reactions: Observe for signs and symptoms of
hypersensitivity during and after Injectafer administration for at least
30 minutes and until clinically stable following completion of each
administration. (5.1)
• Hypertension: Monitor patients closely for signs and symptoms of
hypertension following each Injectafer administration. (5.2)
------------------------------ADVERSE REACTIONS---------------------------------The most common adverse reactions (≥ 2%) are nausea, hypertension,
flushing, hypophosphatemia, and dizziness (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact American Regent at
1-800-734-9236 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
------------------------USE IN SPECIFIC POPULATIONS---------------------------• Nursing Mothers: Exercise caution when administered to a nursing
woman. (8.3)
See 17 for PATIENT COUNSELING INFORMATION and FDA-approved
patient labeling.
Revised: July 2013
*Sections or subsections omitted from the full prescribing information
are not listed.
10 OVERDOSAGE
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
12.2 Pharmacodynamics
12.3 Pharmacokinetics
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, and Impairment of Fertility
14 CLINICALRQ105200
STUDIES
14.1 Trial 1: Iron Deficiency Anemia in Patients Who are Intolerant to
Oral Iron or Have Had Unsatisfactory Response to Oral Iron
14.2 Trial 2: Iron Deficiency Anemia in Patients with Non-Dialysis
Dependent Chronic Kidney Disease
16 HOW SUPPLIED/STORAGE AND HANDLING
17 PATIENT COUNSELING INFORMATION
In clinical trials, serious anaphylactic/anaphylactoid reactions were reported
in 0.1% (2/1775) of subjects receiving Injectafer. Other serious or severe
adverse reactions potentially associated with hypersensitivity which included,
but not limited to, pruritus, rash, urticaria, wheezing, or hypotension were
reported in 1.5% (26/1775) of these subjects.
5.2 Hypertension
In clinical studies, hypertension was reported in 3.8% (67/1,775) of subjects
in clinical trials 1 and 2. Transient elevations in systolic blood pressure,
sometimes occurring with facial flushing, dizziness, or nausea were observed
in 6% (106/1,775) of subjects in these two clinical trials. These elevations
generally occurred immediately after dosing and resolved within 30 minutes.
Monitor patients for signs and symptoms of hypertension following each
Injectafer administration [see Dosage and Administration (2)].
5.3 Laboratory Test Alterations
--------------------------DOSAGE
FORMS AND STRENGTHS----------------------In the 24 hours following administration of Injectafer, laboratory assays may
750 mg iron / 15 mL single-use vial. (3)
overestimate serum iron and transferrin bound iron by also measuring the
-------------------------------CONTRAINDICATIONS--------------------------------iron
in Injectafer.
Hypersensitivity to Injectafer or any of its inactive components. (4)
6
ADVERSE REACTIONS
------------------------WARNINGS AND PRECAUTIONS---------------------------following adverse
reactionsObserve
are discussed
detailof in other
•The Hypersensitivity
reactions:
for signs in
andgreater
symptoms
sections
of the labeling:
hypersensitivity
during and after Injectafer administration for at least
• 30
Hypersensitivity
Reactions
[seestable
Warnings
and Precautions
(5.1)]
minutes and until
clinically
following
completion of
each
• administration.
Hypertension [see
Warnings and Precautions (5.2)]
(5.1)
INJECTAFER®
(ferric carboxymaltose injection)
Proof A
7/26/2013
RQ105200
Cohort 2
Injectafer
IV SCa
(N=245)
(N=237)
Baseline
10.6 (1.0) 10.6 (1.0)
9.1 (1.6)
9.0 (1.5)
Highest Value
12.2 (1.1) 11.4 (1.2)
12.0 (1.2)
11.2 (1.3)
Change (from baseline to
highest value)
1.6 (1.2)
2.9 (1.6)
2.2 (1.3)
0.8 (0.8)
p-value
0.001
0.001
SD=standard deviation; a: Intravenous iron per standard of care
Increases from baseline in mean ferritin (264.2 ± 224.2 ng/mL in Cohort 1
and 218.2 ± 211.4 ng/mL in Cohort 2), and transferrin saturation (13 ± 16%
in Cohort 1 and 20 ± 15% in Cohort 2) were observed at Day 35 in Injectafertreated patients.
14.2 Trial 2: Iron Deficiency Anemia in Patients with Non‑Dialysis
Dependent Chronic Kidney Disease
Trial 2 was a randomized, open-label, controlled clinical study in patients with
non-dialysis dependent chronic kidney disease. Inclusion criteria included
hemoglobin (Hb) ≤ 11.5 g/dL, ferritin ≤ 100 ng/mL or ferritin ≤ 300 ng/mL
when transferrin saturation (TSAT) ≤ 30%. Study patients were randomized
to either Injectafer or Venofer. The mean age of study patients was 67 years
(range, 19 to 96); 64% were female; 54% were Caucasian, 26% were African
American, 18% Hispanics, and 2% were other races.
Table 3 shows the baseline and the change in hemoglobin from baseline to
highest value between baseline and Day 56 or time of intervention.
16
DRUG INTERACTIONS
Hemoglobin (g/dL)
Mean (SD)
Cohort 1
Injectafer Oral Iron
(N=244)
(N=251)
0.9 (0.92)
0.21 (0.13, 0.28)
HOW SUPPLIED/STORAGE AND HANDLING
NDC 0517-0650-01 750 mg iron/15 mL Single-Use Vial Individually boxed
NDC 0517-0650-02 750 mg iron/15 mL Single-Use Vial Packages of 2
Store at 20°C to 25°C (68°F to 77°F); excursions permitted to 15°C to 30°C
(59°F to 86°F). [See the USP controlled room temperature]. Do not freeze.
17
PATIENT COUNSELING INFORMATION
•
Question patients regarding any prior history of reactions to
parenteral iron products.
Advise patients of the risks associated with Injectafer.
Advise patients to report any signs and symptoms of hypersensitivity
that may develop during and following Injectafer administration,
such as rash, itching, dizziness, lightheadedness, swelling and
breathing problems [see Warnings and Precautions (5)]
Injectafer is manufactured under license from Vifor (International) Inc,
Switzerland.
•
•
AMERICAN
REGENT, INC.
SHIRLEY, NY 11967
IN0650ADV
Iss. 7/2013
INJECTAFER®
(ferric carboxymaltose injection)
Patient Information
INJECTAFER (ferric carboxymaltose injection)
Please read this information carefully before taking this
medication. This summary does not tell you everything
about INJECTAFER. Speak with your doctor or healthcare
professional if there is something you do not understand or if
you would like to learn more about INJECTAFER. Your doctor
or healthcare professional is your best source of information
about this medicine.
What is INJECTAFER?
Iron is a mineral that the body needs to produce red blood
cells. When the body does not get enough iron, it cannot
produce the number of normal red blood cells needed to keep
you in good health. This condition is called iron deficiency
(iron shortage) or iron deficiency anemia.
INJECTAFER is used to treat iron deficiency anemia. Iron
deficiency anemia may be caused by several medical
conditions including heavy menstrual bleeding, pregnancy,
childbirth, inflammatory bowel disease, other malabsorption
diseases, bariatric surgery, or chronic kidney disease.
General information about using INJECTAFER safely and
effectively
Injectable iron is administered only by or under the supervision
of your health care professional.
Serious or life threatening allergic reactions have been
reported with intravenous iron products. Tell your health
care professional if you have ever had any unusual or allergic
reaction to any IV iron.
Patients should report to their healthcare professional any
signs and symptoms of an allergic reaction to INJECTAFER, in
particular rashes, shortness of breath and wheezing.
Iron is not easily eliminated from the body, and its build up
may be lead to a condition called iron overload which may be
harmful. Certain medical conditions such as liver disease may
also make you more likely to develop iron overload. Ask your
doctor or healthcare professional.
Other adverse reactions reported by ≥ 0.5% of treated patients include
abdominal pain, diarrhea, gamma glutamyl transferase increased, injection
site pain/irritation, rash, paraesthesia, sneezing. Transient decreases in
laboratory blood phosphorus levels (< 2 mg/dL) have been observed in 27%
(440/1638) patients in clinical trials.
6.2 Post-marketing Experience
Because these reactions are reported voluntarily from a population of uncertain
size, it is not always possible to reliably estimate their frequency or establish a
causal relationship to drug exposure. The following serious adverse reactions
have been most commonly reported from the post-marketing spontaneous
reports with Injectafer: urticaria, dyspnea, pruritis, tachycardia, erythema,
pyrexia, chest discomfort, chills, angioedema, back pain, arthralgia, and
syncope. One case of hypophosphatemic osteomalacia was reported in
a subject who received 500 mg of Injectafer every 2 weeks for a total of
16 weeks. Partial recovery followed discontinuation of Injectafer.
CLINICAL STUDIES
The safety and efficacy of Injectafer for treatment of iron deficiency anemia
were evaluated in two randomized, open-label, controlled clinical trials (Trial
1 and Trial 2). In these two trials, Injectafer was administered at a dose of
15 mg/kg body weight up to a maximum single dose of 750 mg of iron
on two occasions separated by at least 7 days up to a cumulative dose of
1500 mg of iron.
14.1 Trial 1: Iron Deficiency Anemia in Patients Who Are Intolerant to Oral
Iron or Have Had Unsatisfactory Response to Oral Iron
Trial 1 was a randomized, open-label, controlled clinical study in patients
with iron deficiency anemia who had an unsatisfactory response to oral iron
(Cohort 1) or who were intolerant to oral iron (Cohort 2) during the 14 day
oral iron run-in period. Inclusion criteria prior to randomization included
hemoglobin (Hb) <12 g/dL, ferritin ≤ 100 ng/mL or ferritin ≤ 300 ng/mL when
transferrin saturation (TSAT) ≤ 30%. Cohort 1 subjects were randomized to
Injectafer or oral iron for 14 more days. Cohort 2 subjects were randomized
to Injectafer or another IV iron per standard of care [90% of subjects received
iron sucrose]. The mean age of study patients was 43 years (range, 18 to
94); 94% were female; 42% were Caucasian, 32% were African American,
24% were Hispanic, and 2% were other races. The primary etiologies of iron
deficiency anemia were heavy uterine bleeding (47%) and gastrointestinal
disorders (17%).
Table 2 shows the baseline and the change in hemoglobin from baseline to
highest value between baseline and Day 35 or time of intervention.
Table 2. Mean Change in Hemoglobin From Baseline to the Highest
Value Between Day 35 or Time of Intervention (Modified Intent‑to‑Treat
Population)
1.1 (1.0)
7
14
Venofer
(N=1244)
10.3 (0.8)
11.3 (1.1)
Increases from baseline in mean ferritin (734.7 ± 337.8 ng/mL), and transferrin
saturation (30 ± 17%) were observed at Day 56 in Injectafer-treated patients.
USE IN SPECIFIC POPULATIONS
NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenicity studies have not been performed with ferric carboxymaltose.
Ferric carboxymaltose was not genotoxic in the following genetic toxicology
studies: in vitro microbial mutagenesis (Ames) assay, in vitro chromosome
aberration test in human lymphocytes, in vitro mammalian cell mutation assay
in mouse lymphoma L5178Y/TK+/- cells, in vivo mouse micronucleus test at
single intravenous doses up to 500 mg/kg.
In a combined male and female fertility study, ferric carboxymaltose was
administered intravenously over one hour to male and female rats at iron
doses of up to 30 mg/kg. Animals were dosed 3 times per week (on Days 0,
3, and 7). There was no effect on mating function, fertility or early embryonic
development. The dose of 30 mg/kg in animals is approximately 40% of the
human dose of 750 mg based on body surface area.
Formal drug interaction studies have not been performed with Injectafer.
13
Injectafer
(N=1249)
10.3 (0.8)
11.4 (1.2)
RQ105200
Hemoglobin (g/dL)
Mean (SD)
Baseline
Highest Value
Change (from baseline to highest
value)
Treatment Difference (95% CI)
8
12.3 Pharmacokinetics
After administration of a single dose of Injectafer of 100 to 1000 mg of iron in
iron deficient patients, maximum iron levels of 37 μg/mL to 333 μg/mL were
obtained respectively after 15 minutes to 1.21 hours post dose. The volume of
distribution was estimated to be 3 L.
The iron injected or infused was rapidly cleared from the plasma, the terminal
half-life ranged from 7 to 12 hours. Renal elimination of iron was negligible.
------iron
Table 3.
Mean Change in Hemoglobin From Baseline to the
Highest Value Between Baseline and Day 56 or Time of Intervention
(Modified Intent‑to‑Treat Population)
8.1 Pregnancy
Pregnancy Category C
Risk Summary
Adequate and well controlled studies in pregnant women have not been
conducted. However, animal reproduction studies have been conducted with
ferric carboxymaltose. In these studies, administration of ferric carboxymaltose
to rabbits during the period of organogenesis caused fetal malformations and
increased implantation loss at maternally toxic doses of approximately 12%
to 23% of the human weekly dose of 750 mg (based on body surface area).
The incidence of major malformations in human pregnancies has not been
established for Injectafer. However, all pregnancies, regardless of exposure to
any drug, has a background rate of 2 to 4% for major malformations, and 15
to 20% for pregnancy loss. Injectafer should be used during pregnancy only if
the potential benefit justifies the potential risk to the fetus.
Animal Data
Administration of ferric carboxymaltose to rats as a one-hour intravenous
infusion up to 30 mg/kg/day iron on gestation days 6 to 17 did not result in
adverse embryofetal findings. This daily dose in rats is approximately 40%
of the human weekly dose of 750 mg based on body surface area. In rabbits,
ferric carboxymaltose was administered as a one-hour infusion on gestation
days 6 to 19 at iron doses of 4.5, 9, 13.5, and 18 mg/kg/day. Malformations
were seen starting at the daily dose of 9 mg/kg (23% of the human weekly
dose of 750 mg). Spontaneous abortions occurred starting at the daily iron
dose of 4.5 mg/kg (12% of the human weekly dose based on body surface
area). Pre-implantation loss was at the highest dose. Adverse embryofetal
effects were observed in the presence of maternal toxicity.
A pre- and post-natal development study was conducted in rats at intravenous
doses up to 18 mg/kg/day of iron (approximately 23% of the weekly human
dose of 750 mg on a body surface area basis). There were no adverse effects
on survival of offspring, their behavior, sexual maturation or reproductive
parameters.
8.3 Nursing Mothers
A study to determine iron concentrations in breast milk after administration of
Injectafer (n=11) or oral ferrous sulfate (n=14) was conducted in 25 lactating
women with postpartum iron deficiency anemia. Mean breast milk iron levels
were higher in lactating women receiving Injectafer than in lactating women
receiving oral ferrous sulfate.
Other adverse reactions reported by ≥ 0.5% of treated patients include
8.4 Pediatric Use
abdominal pain, diarrhea, gamma glutamyl transferase increased, injection
Safety and effectiveness have not been established in pediatric patients.
site pain/irritation, rash, paraesthesia, sneezing. Transient decreases in
8.5
Geriatric
laboratory
bloodUse
phosphorus levels (< 2 mg/dL) have been observed in 27%
Of
the 1775patients
subjectsininclinical
clinicaltrials.
studies of Injectafer, 50% were 65 years and
(440/1638)
over, while 25% were 75 years and over. No overall differences in safety or
6.2 Post-marketing Experience
effectiveness were observed between these subjects and younger subjects,
Because these reactions are reported voluntarily from a population of uncertain
and other reported clinical experience has not identified differences in
size, it is not always possible to reliably estimate their frequency or establish a
responses between the elderly and younger patients, but greater sensitivity of
causal relationship to drug exposure. The following serious adverse reactions
some older individuals cannot be ruled out.
12.2 Pharmacodynamics
Using positron emission tomography (PET) it was demonstrated that red cell
uptake of 59Fe and 52Fe from Injectafer ranged from 61% to 99%. In patients
with iron deficiency, red cell uptake of radio-labeled iron ranged from 91% to
99% at 24 days after Injectafer dose. In patients with renal anemia red cell
uptake of radio-labeled iron ranged from 61% to 84% after 24 days Injectafer
dose.
nse to
CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
Ferric carboxymaltose is a colloidal iron (III) hydroxide in complex with
carboxymaltose, a carbohydrate polymer that releases iron.
-------
12
--------------------------DOSAGE FORMS AND STRENGTHS----------------------750 mg iron / 15 mL single-use vial. (3)
-------------------------------CONTRAINDICATIONS--------------------------------Hypersensitivity to Injectafer or any of its inactive components. (4)
------------------------WARNINGS AND PRECAUTIONS---------------------------• Hypersensitivity reactions: Observe for signs and symptoms of
hypersensitivity during and after Injectafer administration for at least
30 minutes and until clinically stable following completion of each
administration. (5.1)
• Hypertension: Monitor patients closely for signs and symptoms of
hypertension following each Injectafer administration. (5.2)
------------------------------ADVERSE REACTIONS---------------------------------The most common adverse reactions (≥ 2%) are nausea, hypertension,
flushing, hypophosphatemia, and dizziness (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact American Regent at
1-800-734-9236 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
------------------------USE IN SPECIFIC POPULATIONS---------------------------• Nursing Mothers: Exercise caution when administered to a nursing
woman. (8.3)
See 17 for PATIENT COUNSELING INFORMATION and FDA-approved
patient labeling.
Revised: July 2013
*Sections or subsections omitted from the full prescribing information
are not listed.
10 OVERDOSAGE
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
12.2 Pharmacodynamics
12.3 Pharmacokinetics
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, and Impairment of Fertility
14 CLINICAL STUDIES
14.1 Trial 1: Iron Deficiency Anemia in Patients Who are Intolerant to
Oral Iron or Have Had Unsatisfactory Response to Oral Iron
14.2 Trial 2: Iron Deficiency Anemia in Patients with Non-Dialysis
Dependent Chronic Kidney Disease
16 HOW SUPPLIED/STORAGE AND HANDLING
17 PATIENT COUNSELING INFORMATION
In clinical trials, serious anaphylactic/anaphylactoid reactions were reported
in 0.1% (2/1775) of subjects receiving Injectafer. Other serious or severe
adverse reactions potentially associated with hypersensitivity which included,
but not limited to, pruritus, rash, urticaria, wheezing, or hypotension were
reported in 1.5% (26/1775) of these subjects.
5.2 Hypertension
In clinical studies, hypertension was reported in 3.8% (67/1,775) of subjects
in clinical trials 1 and 2. Transient elevations in systolic blood pressure,
sometimes occurring with facial flushing, dizziness, or nausea were observed
in 6% (106/1,775) of subjects in these two clinical trials. These elevations
generally occurred immediately after dosing and resolved within 30 minutes.
Monitor patients for signs and symptoms of hypertension following each
Injectafer administration [see Dosage and Administration (2)].
5.3 Laboratory Test Alterations
--------------------------DOSAGE
FORMS AND STRENGTHS----------------------In the 24 hours following administration of Injectafer, laboratory assays may
750 mg iron / 15 mL single-use vial. (3)
overestimate serum iron and transferrin bound iron by also measuring the
-------------------------------CONTRAINDICATIONS--------------------------------iron
in Injectafer.
Hypersensitivity to Injectafer or any of its inactive components. (4)
6
ADVERSE REACTIONS
------------------------WARNINGS AND PRECAUTIONS---------------------------following adverse
reactionsObserve
are discussed
detailof in other
•The Hypersensitivity
reactions:
for signs in
andgreater
symptoms
sections
of the labeling:
hypersensitivity
during and after Injectafer administration for at least
• 30
Hypersensitivity
Reactions
[seestable
Warnings
and Precautions
(5.1)]
minutes and until
clinically
following
completion of
each
• administration.
Hypertension [see
Warnings and Precautions (5.2)]
(5.1)
Injectafer (ferric carboxymaltose injection) is a dark brown, sterile, aqueous,
isotonic colloidal solution for intravenous injection. Each mL contains 50 mg
iron as ferric carboxymaltose in water for injection. Injectafer is available in
15 mL single-use vials. Sodium hydroxide and/or hydrochloric acid may have
been added to adjust the pH to 5.0-7.0.
Vial closure is not made with natural rubber latex.
al
oses
ght.
. (2)
adult
nse to
doses
ulative
doses
t for a
mL of
may be
enous
give at
------ed via
iron
0.9%
INJECTAFER®
(ferric carboxymaltose injection)
Who should not take INJECTAFER?
You should not be given INJECTAFER if you have anemia that
is not caused by iron deficiency, or if you have iron overload.
If you are pregnant or plan to become pregnant please notify
your doctor or healthcare professional. They will decide
whether it is safe for you to receive INJECTAFER.
How should I take INJECTAFER?
INJECTAFER is administered intravenously (into your vein) by
your doctor or healthcare professional in two doses.
What should I avoid while taking INJECTAFER?
You should not take iron supplements by mouth if you
are receiving iron injections. Tell your doctor about all
the medicines you take, including prescription and nonprescription medicines, vitamins and herbal supplements.
What are the possible side effects of INJECTAFER?
The side effects of INJECTAFER are infrequent, usually
mild and generally do not cause patients to stop treatment.
The most common side effects are nausea, injection site
reactions (including pain or bruising at the injection site),
asymptomatic reductions in blood phosphorus, flushing,
headache, hypertension, dizziness, and increased alanine
aminotransferase. Potentially long lasting brown staining of
skin near injection site may occur.
These are not all the possible side effects of INJECTAFER. For
more information ask your doctor or healthcare professional.
Talk to your doctor if you think you have side effects from
taking INJECTAFER.
651 S ML King Jr Ave • Waukegan, IL 60085 • Phone 847.336.4200 • Fax 847.360.4924
Proof A
HIGHLIGHTS OF PRESCRIBING INFORMATION
These highlights do not include all the information needed to use VENOFER safely and effectively.
See full prescribing information for VENOFER.
Venofer® (iron sucrose injection, USP)
Initial U.S. Approval: 2000
--------------------------------------------------------------- INDICATIONS AND USAGE --------------------------------------------------------------Venofer is an iron replacement product indicated for the treatment of iron deficiency anemia in patients with chronic kidney disease
(CKD). (1)
----------------------------------------------------------- DOSAGE AND ADMINISTRATION ----------------------------------------------------------Population
Adult patients
Pediatric patients
Dose
Hemodialysis Dependent-Chronic Kidney
Disease (HDD-CKD) (2.1)
100 mg slow intravenous injection or infusion
Non-Dialysis Dependent-Chronic Kidney
Disease (NDD-CKD) (2.2)
200 mg slow intravenous injection or infusion
Peritoneal Dialysis Dependent-Chronic
Kidney Disease (PDD-CKD) (2.3)
300 mg or 400 mg intravenous infusion
HDD-CKD (2.4), PDD-CKD or NDD-CKD (2.5)
0.5 mg/kg slow intravenous injection or infusion
---------------------------------------------------------- DOSAGE FORMS AND STRENGTHS --------------------------------------------------------• 10 mL single-use vial / 200 mg elemental iron (20 mg/mL) (3)
• 5 mL single-use vial / 100 mg elemental iron (20 mg/mL) (3)
• 2.5 mL single-use vial / 50 mg elemental iron (20 mg/mL) (3)
----------------------------------------------------------------- CONTRAINDICATIONS ----------------------------------------------------------------• Known hypersensitivity to Venofer (4)
--------------------------------------------------------- WARNINGS AND PRECAUTIONS ------------------------------------------------------------• Hypersensitivity Reactions: Observe for signs and symptoms of hypersensitivity during and after Venofer administration for at least 30
minutes and until clinically stable following completion of each administration. Only administer Venofer when personnel and therapies
are immediately available for the treatment of serious hypersensitivity reactions. (5.1)
• Hypotension: Venofer may cause hypotension. Monitor for signs and symptoms of hypotension during and following each
administration of Venofer. (5.2)
• Iron Overload: Regularly monitor hematologic responses during Venofer therapy. Do not administer Venofer to patients with iron
overload. (5.3)
----------------------------------------------------------------- ADVERSE REACTIONS ----------------------------------------------------------------• The most common adverse reactions (≥2%) following the administration of Venofer are diarrhea, nausea, vomiting, headache,
dizziness, hypotension, pruritus, pain in extremity, arthralgia, back pain, muscle cramp, injection site reactions, chest pain, and
peripheral edema. (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact American Regent, Inc. at 1-800-734-9236 or FDA at 1-800-FDA-1088 or
www.fda.gov/medwatch.
See 17 for PATIENT COUNSELING INFORMATION
Revised: 8/2015
FULL PRESCRIBING INFORMATION: CONTENTS*
1.
INDICATIONS AND USAGE
2.
DOSAGE AND ADMINISTRATION
2.1 Adult Patients with Hemodialysis Dependent-Chronic Kidney Disease (HDD-CKD)
2.2 Adult Patients with Non-Dialysis Dependent-Chronic Kidney Disease (NDD-CKD)
2.3 Adult Patients with Peritoneal Dialysis Dependent-Chronic Kidney Disease (PDD-CKD)
2.4 Pediatric Patients (2 years of age and older) with HDD-CKD for iron maintenance treatment
2.5 Pediatric Patients (2 years of age and older) with NDD-CKD or PDD-CKD who are on erythropoietin
therapy for iron maintenance treatment
3.
DOSAGE FORMS AND STRENGTHS
4.
CONTRAINDICATIONS
5.
WARNINGS AND PRECAUTIONS
5.1 Hypersensitivity Reactions
5.2 Hypotension
5.3 Iron Overload
6.
ADVERSE REACTIONS
6.1 Adverse Reactions in Clinical Trials
6.2 Adverse Reactions from Post-Marketing Experience
7.
DRUG INTERACTIONS
8.
USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
8.3 Nursing Mothers
8.4 Pediatric Use
8.5 Geriatric Use
10.OVERDOSAGE
11.DESCRIPTION
12. CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
12.2 Pharmacodynamics
12.3 Pharmacokinetics
13. NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
14. CLINICAL STUDIES
14.1 Study A: Hemodialysis Dependent-Chronic Kidney Disease (HDD-CKD)
14.2 Study B: Hemodialysis Dependent-Chronic Kidney Disease (HDD-CKD)
14.3 Study C: Hemodialysis Dependent-Chronic Kidney Disease (HDD-CKD)
14.4 Study D: Non-Dialysis Dependent-Chronic Kidney Disease (NDD-CKD)
14.5 Study E: Peritoneal Dialysis Dependent-Chronic Kidney Disease (PDD-CKD)
14.6 Study F: Iron Maintenance Treatment Dosing in Pediatric Patients Ages 2 years and Older with
Chronic Kidney Disease
16. HOW SUPPLIED/STORAGE AND HANDLING
16.1 How Supplied
16.2 Stability and Storage
17.
PATIENT COUNSELING INFORMATION
* Sections or subsections omitted from the full prescribing information are not listed.
FULL PRESCRIBING INFORMATION
1. INDICATIONS AND USAGE
Venofer is indicated for the treatment of iron deficiency anemia in patients with chronic kidney disease (CKD).
2. DOSAGE AND ADMINISTRATION
Venofer must only be administered intravenously either by slow injection or by infusion. The dosage of Venofer is expressed in mg of
elemental iron. Each mL contains 20 mg of elemental iron.
2.1 Adult Patients with Hemodialysis Dependent-Chronic Kidney Disease (HDD-CKD)
Administer Venofer 100 mg undiluted as a slow intravenous injection over 2 to 5 minutes, or as an infusion of 100 mg diluted in a
maximum of 100 mL of 0.9% NaCl over a period of at least 15 minutes, per consecutive hemodialysis session. Venofer should be
administered early during the dialysis session. The usual total treatment course of Venofer is 1000 mg. Venofer treatment may be
repeated if iron deficiency reoccurs.
2.2 Adult Patients with Non-Dialysis Dependent-Chronic Kidney Disease (NDD-CKD)
Administer Venofer 200 mg undiluted as a slow intravenous injection over 2 to 5 minutes or as an infusion of 200 mg in a maximum of
100 mL of 0.9% NaCl over a period of 15 minutes. Administer on 5 different occasions over a 14 day period. There is limited experience
with administration of an infusion of 500 mg of Venofer, diluted in a maximum of 250 mL of 0.9% NaCl, over a period of 3.5 to 4 hours
on Day 1 and Day 14. Venofer treatment may be repeated if iron deficiency reoccurs.
2.3 Adult Patients with Peritoneal Dialysis Dependent-Chronic Kidney Disease (PDD-CKD)
Administer Venofer in 3 divided doses, given by slow intravenous infusion, within a 28 day period: 2 infusions each of 300 mg over 1.5
hours 14 days apart followed by one 400 mg infusion over 2.5 hours 14 days later. Dilute Venofer in a maximum of 250 mL of 0.9% NaCl.
Venofer treatment may be repeated if iron deficiency reoccurs.
2.4 Pediatric Patients (2 years of age and older) with HDD-CKD for iron maintenance treatment
The dosing for iron replacement treatment in pediatric patients with HDD-CKD has not been established.
For iron maintenance treatment: Administer Venofer at a dose of 0.5 mg/kg, not to exceed 100 mg per dose, every two weeks for 12
weeks given undiluted by slow intravenous injection over 5 minutes or diluted in 25 mL of 0.9% NaCl and administered over 5 to 60
minutes. Venofer treatment may be repeated if necessary.
2.5 Pediatric Patients (2 years of age and older) with NDD-CKD or PDD-CKD who are on erythropoietin therapy for iron maintenance
treatment
The dosing for iron replacement treatment in pediatric patients with NDD-CKD or PDD-CKD has not been established.
For iron maintenance treatment: Administer Venofer at a dose of 0.5 mg/kg, not to exceed 100 mg per dose, every four weeks for 12
weeks given undiluted by slow intravenous injection over 5 minutes or diluted in 25 mL of 0.9% NaCl and administered over 5 to 60
minutes. Venofer treatment may be repeated if necessary.
3. DOSAGE FORMS AND STRENGTHS
• 10 mL single-use vial / 200 mg elemental iron (20 mg/mL)
• 5 mL single-use vial / 100 mg elemental iron (20 mg/mL)
• 2.5 mL single-use vial / 50 mg elemental iron (20 mg/mL)
4.CONTRAINDICATIONS
• Known hypersensitivity to Venofer
5. WARNINGS AND PRECAUTIONS
5.1 Hypersensitivity Reactions
Serious hypersensitivity reactions, including anaphylactic-type reactions, some of which have been life-threatening and fatal,
have been reported in patients receiving Venofer. Patients may present with shock, clinically significant hypotension, loss of
consciousness, and/or collapse. If hypersensitivity reactions or signs of intolerance occur during administration, stop Venofer
immediately. Monitor patients for signs and symptoms of hypersensitivity during and after Venofer administration for at least 30
minutes and until clinically stable following completion of the infusion. Only administer Venofer when personnel and therapies
are immediately available for the treatment of serious hypersensitivity reactions. Most reactions associated with intravenous iron
preparations occur within 30 minutes of the completion of the infusion [see Adverse Reactions (6.1 and 6.2)].
5.2Hypotension
Venofer may cause clinically significant hypotension. Monitor for signs and symptoms of hypotension following each administration of
Venofer. Hypotension following administration of Venofer may be related to the rate of administration and/or total dose administered [See
Dosage and Administration (2), Warnings and Precautions (5.1), and Adverse Reactions (6.2)].
5.3 Iron Overload
Excessive therapy with parenteral iron can lead to excess storage of iron with the possibility of iatrogenic hemosiderosis. All adult and
pediatric patients receiving Venofer require periodic monitoring of hematologic and iron parameters (hemoglobin, hematocrit, serum
ferritin and transferrin saturation). Do not administer Venofer to patients with evidence of iron overload. Transferrin saturation (TSAT)
values increase rapidly after intravenous administration of iron sucrose; do not perform serum iron measurements for at least 48 hours
after intravenous dosing [See Dosage and Administration (2) and Overdosage (10)].
6. ADVERSE REACTIONS
The following serious adverse reactions associated with Venofer are described in other sections [See Warnings and Precautions (5.1,
5.2 and 5.3)].
6.1 Adverse Reactions in Clinical Trials
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug may
not reflect the rates observed in practice.
Adverse Reactions in Adult Patients with CKD
The frequency of adverse reactions associated with the use of Venofer has been documented in six clinical trials involving 231 patients
with HDD-CKD, 139 patients with NDD-CKD and 75 patients with PDD-CKD. Treatment-emergent adverse reactions reported by ≥2% of
treated patients in the six clinical trials for which the rate for Venofer exceeds the rate for comparator are listed by indication in Table 1.
Patients with HDD-CKD received 100 mg doses at 10 consecutive dialysis sessions until a cumulative dose of 1000 mg was administered.
Patients with NDD-CKD received either 5 doses of 200 mg over 2 weeks or 2 doses of 500 mg separated by fourteen days, and patients
with PDD-CKD received 2 doses of 300 mg followed by a dose of 400 mg over a period of 4 weeks.
Table 1. Treatment-Emergent Adverse Reactions Reported in ≥2% of Study Populations and for which the Rate for Venofer Exceeds
the Rate for Comparator
Venofer PI JUN2016_8JUN2016.indd 1
HDD-CKD
Adverse Reactions (Preferred Term)
NDD-CKD
PDD-CKD
Venofer
(N=231) %
Venofer
(N=139) %
Oral Iron
(N=139) %
Venofer
(N=75) %
EPO* Only
(N=46) %
78.8
76.3
73.4
72.0
65.2
0
2.2
0.7
0
0
Eye Disorders
Conjunctivitis
0.4
0
0
2.7
0
Gastrointestinal Disorders
Abdominal pain
Diarrhea
Dysgeusia
Nausea
Vomiting
3.5
5.2
0.9
14.7
9.1
1.4
7.2
7.9
8.6
5.0
2.9
10.1
0
12.2
8.6
4.0
8.0
0
5.3
8.0
6.5
4.3
0
4.3
2.2
General Disorders and
Administration Site Conditions
Asthenia
Chest pain
Feeling abnormal
Infusion site pain or burning
Injection site extravasation
Peripheral edema
Pyrexia
2.2
6.1
3.0
0
0
2.6
3.0
0.7
1.4
0
5.8
2.2
7.2
0.7
2.2
0
0
0
0
5.0
0.7
2.7
2.7
0
0
0
5.3
1.3
0
0
0
0
0
10.9
0
Infections and Infestations
Nasopharyngitis, Sinusitis, Upper
respiratory tract infections, Pharyngitis
2.6
2.2
4.3
16.0
4.3
Injury, Poisoning and Procedural
Complications
Graft complication
9.5
1.4
0
0
0
Metabolism and Nutrition Disorders
Fluid overload
Gout
Hyperglycemia
Hypoglycemia
3.0
0
0
0.4
1.4
2.9
2.9
0.7
0.7
1.4
0
0.7
1.3
0
0
4.0
0
0
2.2
0
Musculoskeletal and Connective
Tissue Disorders
Arthralgia
Back pain
Muscle cramp
Myalgia
Pain in extremity
3.5
2.2
29.4
0
5.6
1.4
2.2
0.7
3.6
4.3
2.2
3.6
0.7
0
0
4.0
1.3
2.7
1.3
2.7
4.3
4.3
0
0
6.5
Nervous System Disorders
Dizziness
Headache
6.5
12.6
6.5
2.9
1.4
0.7
1.3
4.0
4.3
0
Respiratory, Thoracic and
Mediastinal Disorders
Cough
Dyspnea
Nasal congestion
3.0
3.5
0
2.2
5.8
1.4
0.7
1.4
2.2
1.3
1.3
1.3
0
2.2
0
Skin and Subcutaneous
Tissue Disorders
Pruritus
3.9
2.2
4.3
2.7
0
Vascular Disorders
Hypertension
Hypotension
6.5
39.4
6.5
2.2
4.3
0.7
8.0
2.7
6.5
2.2
Subjects with any adverse reaction
Ear and Labyrinth Disorders
Ear Pain
* EPO=Erythropoietin
One hundred thirty (11%) of the 1,151 patients evaluated in the 4 U.S. trials in HDD-CKD patients (studies A, B and the two post
marketing studies) had prior other intravenous iron therapy and were reported to be intolerant (defined as precluding further use of that
iron product). When these patients were treated with Venofer there were no occurrences of adverse reactions that precluded further use
of Venofer [See Warning and Precautions (5)].
6/8/2016 4:01:41 PM
Adverse Reactions in Pediatric Patients with CKD (ages 2 years and older)
In a randomized, open-label, dose-ranging trial for iron maintenance treatment with Venofer in pediatric patients with CKD on stable
erythropoietin therapy [see Clinical Studies (14.6)], at least one treatment-emergent adverse reaction was experienced by 57% (27/47) of
the patients receiving Venofer 0.5 mg/kg, 53% (25/47) of the patients receiving Venofer 1.0 mg/kg, and 55% (26/47) of the patients receiving
Venofer 2.0 mg/kg.
A total of 5 (11%) subjects in the Venofer 0.5 mg/kg group, 10 (21%) patients in the Venofer 1.0 mg/kg group, and 10 (21%) patients in the
Venofer 2.0 mg/kg group experienced at least 1 serious adverse reaction during the study. The most common treatment-emergent adverse
reactions (> 2% of patients) in all patients were headache (6%), respiratory tract viral infection (4%), peritonitis (4%), vomiting (4%), pyrexia
(4%), dizziness (4%), cough (4%), renal transplant (4%), nausea (3%), arteriovenous fistula thrombosis (2%), hypotension (2%), and
hypertension (2.1%).
6.2 Adverse Reactions from Post-Marketing Experience
Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency
or establish a causal relationship to drug exposure.
In the post-marketing safety studies in 1,051 treated patients with HDD-CKD, the adverse reactions reported by > 1% were: cardiac failure
congestive, sepsis and dysgeusia.
The following adverse reactions have been identified during post-approval use of Venofer. Because these reactions are reported voluntarily
from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug
exposure: Anaphylactic-type reactions, shock, loss of consciousness, collapse, bronchospasm, dyspnea, convulsions, light-headedness,
confusion, angioedema, swelling of the joints, hyperhidrosis, back pain, bradycardia, and chromaturia.
Symptoms associated with Venofer total dosage or infusing too rapidly included hypotension, dyspnea, headache, vomiting, nausea, dizziness,
joint aches, paresthesia, abdominal and muscle pain, edema, and cardiovascular collapse. These adverse reactions have occurred up to 30
minutes after the administration of Venofer injection. Reactions have occurred following the first dose or subsequent doses of Venofer.
Symptoms may respond to intravenous fluids, hydrocortisone, and/or antihistamines. Slowing the infusion rate may alleviate symptoms.
Injection site discoloration has been reported following extravasation. Assure stable intravenous access to avoid extravasation.
7. DRUG INTERACTIONS
Drug interactions involving Venofer have not been studied. However, Venofer may reduce the absorption of concomitantly administered oral
iron preparations.
8. USE IN SPECIFIC POPULATIONS
8.1Pregnancy
Pregnancy Category B
There are no adequate and well-controlled studies in pregnant women. In animal reproduction studies, iron sucrose was administered
intravenously to rats and rabbits during the period of organogenesis at doses up to 13 mg/kg/day of elemental iron (half or equivalent to the
maximum recommended human dose based on body surface area, respectively) and revealed no evidence of harm to the fetus due to iron
sucrose. Because animal reproductive studies are not always predictive of human response, Venofer should be used during pregnancy only
if clearly needed.
8.3 Nursing Mothers
It is not known whether iron sucrose is excreted in human milk. Iron sucrose is secreted into the milk of lactating rats. Because many drugs
are excreted in human milk, caution should be exercised when Venofer is administered to a nursing woman.
8.4 Pediatric Use
Safety and effectiveness of Venofer for iron replacement treatment in pediatric patients with dialysis-dependent or non-dialysis-dependent
CKD have not been established.
Safety and effectiveness of Venofer for iron maintenance treatment in pediatric patients 2 years of age and older with dialysis-dependent or
non-dialysisdependent CKD receiving erythropoietin therapy were studied. Venofer at doses of 0.5 mg/kg, 1.0 mg/kg, and 2.0 mg/kg was
administered. All three doses maintained hemoglobin between 10.5 g/dL and 14.0 g/dL in about 50% of subjects over the 12-week treatment
period with stable EPO dosing. [See Clinical Studies (14.6)]
Venofer has not been studied in patients younger than 2 years of age.
In a country where Venofer is available for use in children, at a single site, five premature infants (weight less than 1,250 g) developed
necrotizing enterocolitis and two of the five died during or following a period when they received Venofer, several other medications and
erythropoietin. Necrotizing enterocolitis may be a complication of prematurity in very low birth weight infants. No causal relationship to
Venofer or any other drugs could be established.
8.5 Geriatric Use
Clinical studies of Venofer did not include sufficient numbers of subjects aged 65 years and older to determine whether they respond differently
from younger subjects. Of the 1,051 patients in two post-marketing safety studies of Venofer, 40% were 65 years and older. No overall
differences in safety were observed between these subjects and younger subjects, and other reported clinical experience has not identified
differences in responses between the elderly and younger patients, but greater sensitivity of some older individuals cannot be ruled out. In
general, dose administration to an elderly patient should be cautious, reflecting the greater frequency of decreased hepatic, renal, or cardiac
function, and of concomitant disease or other drug therapy.
10.OVERDOSAGE
No data are available regarding overdosage of Venofer in humans. Excessive dosages of Venofer may lead to accumulation of iron in storage
sites potentially leading to hemosiderosis. Do not administer Venofer to patients with iron overload. [See Contraindications (4)]
Toxicities in single-dose studies in mice and rats, at intravenous iron sucrose doses up to 8 times the maximum recommended human dose
based on body surface area, included sedation, hypoactivity, pale eyes, bleeding in the gastrointestinal tract and lungs, and mortality.
11.DESCRIPTION
Venofer (iron sucrose injection, USP), an iron replacement product, is a brown, sterile, aqueous, complex of polynuclear iron (III)-hydroxide
in sucrose for intravenous use. Iron sucrose injection has a molecular weight of approximately 34,000 to 60,000 daltons and a proposed
structural formula:
[Na2Fe5O8(OH) • 3(H2O)]n • m(C12H22O11)
where: n is the degree of iron polymerization and m is the number of sucrose molecules associated with the iron (III)-hydroxide.
Each mL contains 20 mg elemental iron as iron sucrose in water for injection. Venofer is available in 10 mL single-use vials (200 mg elemental
iron per 10 mL), 5 mL single-use vials (100 mg elemental iron per 5 mL), and 2.5 mL single-use vials (50 mg elemental iron per 2.5 mL). The
drug product contains approximately 30% sucrose w/v (300 mg/mL) and has a pH of 10.5 to 11.1. The product contains no preservatives.
The osmolarity of the injection is 1,250 mOsmol/L.
12. CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
Venofer is an aqueous complex of poly-nuclear iron (III)-hydroxide in sucrose. Following intravenous administration, Venofer is dissociated
into iron and sucrose and the iron is transported as a complex with transferrin to target cells including erythroid precursor cells. The iron in
the precursor cells is incorporated into hemoglobin as the cells mature into red blood cells.
12.2Pharmacodynamics
Following intravenous administration, Venofer is dissociated into iron and sucrose. In 22 patients undergoing hemodialysis and receiving
erythropoietin (recombinant human erythropoietin) therapy treated with iron sucrose containing 100 mg of iron, three times weekly for three
weeks, significant increases in serum iron and serum ferritin and significant decreases in total iron binding capacity occurred four weeks from
the initiation of iron sucrose treatment.
12.3Pharmacokinetics
In healthy adults administered intravenous doses of Venofer, its iron component exhibited first order kinetics with an elimination half-life of
6 h, total clearance of 1.2 L/h, and steady state apparent volume of distribution of 7.9 L. The iron component appeared to distribute mainly in
blood and to some extent in extravascular fluid. A study evaluating Venofer containing 100 mg of iron labeled with 52Fe/59Fe in patients with
iron deficiency showed that a significant amount of the administered iron is distributed to the liver, spleen and bone marrow and that the bone
marrow is an irreversible iron trapping compartment.
Following intravenous administration of Venofer, iron sucrose is dissociated into iron and sucrose. The sucrose component is eliminated
mainly by urinary excretion. In a study evaluating a single intravenous dose of Venofer containing 1,510 mg of sucrose and 100 mg of iron in
12 healthy adults (9 female, 3 male: age range 32 to 52), 68.3% of the sucrose was eliminated in urine in 4 h and 75.4% in 24 h. Some iron
was also eliminated in the urine. Neither transferrin nor transferrin receptor levels changed immediately after the dose administration. In this
study and another study evaluating a single intravenous dose of iron sucrose containing 500 to 700 mg of iron in 26 patients with anemia on
erythropoietin therapy (23 female, 3 male; age range 16 to 60), approximately 5% of the iron was eliminated in urine in 24 h at each dose level.
The effects of age and gender on the pharmacokinetics of Venofer have not been studied.
Pharmacokinetics in Pediatric Patients
In a single-dose PK study of Venofer, patients with NDD-CDK ages 12 to 16 (N=11) received intravenous bolus doses of Venofer at 7 mg/kg
(maximum 200 mg) administered over 5 minutes. Following single dose Venofer, the half-life of total serum iron was 8 hours. The mean Cmax
and AUC values were 8545 μg/dL and 31305 hr•μg/dL, respectively, which were 1.42- and 1.67-fold higher than dose adjusted adult Cmax and
AUC values.
Venofer is not dialyzable through CA210 (Baxter) High Efficiency or Fresenius F80A High Flux dialysis membranes. In in vitro studies, the
amount of iron sucrose in the dialysate fluid was below the levels of detection of the assay (less than 2 parts per million).
13. NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenicity studies have not been performed with iron sucrose.
Iron sucrose was not mutagenic in vitro in the bacterial reverse mutation assay (Ames test) or the mouse lymphoma assay. Iron sucrose was
not clastogenic in the in vitro chromosome aberration assay using human lymphocytes or in the in vivo mouse micronucleus assay.
Iron sucrose at intravenous doses up to 15 mg/kg/day of elemental iron (1.2 times the maximum recommended human dose based on body
surface area) had no effect on fertility and reproductive function of male and female rats.
14. CLINICAL STUDIES
Five clinical trials involving 647 adult patients and one clinical trial involving 131 pediatric patients were conducted to assess the safety and
efficacy of Venofer.
14.1 Study A: Hemodialysis Dependent-Chronic Kidney Disease (HDD–CKD)
Study A was a multicenter, open-label, historically-controlled study in 101 patients with HDD-CKD (77 patients with Venofer treatment
and 24 in the historical control group) with iron deficiency anemia. Eligibility criteria for Venofer treatment included patients undergoing
chronic hemodialysis, receiving erythropoietin, hemoglobin level between 8.0 and 11.0 g/dL, transferrin saturation < 20%, and serum
ferritin < 300 ng/mL. The mean age of the patients was 65 years with the age range of 31 to 85 years. Of the 77 patients, 44 (57%) were
male and 33 (43%) were female.
Venofer PI JUN2016_8JUN2016.indd 2
Venofer 100 mg was administered at 10 consecutive dialysis sessions either as slow injection or a slow infusion. The historical control
population consisted of 24 patients with similar ferritin levels as patients treated with Venofer, who were off intravenous iron for at least 2
weeks and who had received erythropoietin therapy with hematocrit averaging 31 to 36 for at least two months prior to study entry. The mean
age of patients in the historical control group was 56 years, with an age range of 29 to 80 years. Patient age and serum ferritin level were
similar between treatment and historical control patients. Patients in the Venofer treated population showed a greater increase in hemoglobin
and hematocrit than did patients in the historical control population.
See Table 2.
Table 2. Changes from Baseline in Hemoglobin and Hematocrit
End of treatment
Efficacy
parameters
Historical
Control
(n=18)
Venofer
(n=69)
2 week follow-up
Venofer
(n=73)
5 week follow-up
Historical
Control
(n=18)
Venofer
(n=71)
Historical
Control
(n=15)
Hemoglobin (g/dL)
1.0 ± 0.12**
0.0 ± 0.21
1.3 ± 0.14**
-0.6 ± 0.24
1.2 ± 0.17*
-0.1 ± 0.23
Hematocrit (%)
3.1 ± 0.37**
-0.3 ± 0.65
3.6 ± 0.44**
-1.2 ± 0.76
3.3 ± 0.54
0.2 ± 0.86
**p < 0.01 and *p < 0.05 compared to historical control from ANCOVA analysis with baseline hemoglobin, serum ferritin and
erythropoietin dose as covariates.
Serum ferritin increased at endpoint of study from baseline in the Venofer-treated population (165.3 ± 24.2 ng/mL) compared to the
historical control population (-27.6 ± 9.5 ng/mL). Transferrin saturation also increased at endpoint of study from baseline in the Venofertreated population (8.8 ± 1.6%) compared to this historical control population (-5.1 ± 4.3%).
14.2 Study B: Hemodialysis Dependent-Chronic Kidney Disease (HDD-CKD)
Study B was a multicenter, open label study of Venofer in 23 patients with iron deficiency and HDD-CKD who had been discontinued from
iron dextran due to intolerance. Eligibility criteria were otherwise identical to Study A. The mean age of the patients in this study was 53 years,
with ages ranging from 21 to 79 years. Of the 23 patients enrolled in the study, 10 (44%) were male and 13 (56%) were female.
All 23 enrolled patients were evaluated for efficacy. Increases in mean hemoglobin (1.1 ± 0.2 g/dL), hematocrit (3.6 ± 0.6%), serum
ferritin (266.3 ± 30.3 ng/mL) and transferrin saturation (8.7 ± 2.0%) were observed from baseline to end of treatment.
14.3 Study C: Hemodialysis Dependent-Chronic Kidney Disease (HDD-CKD)
Study C was a multicenter, open-label study in patients with HDD-CKD. This study enrolled patients with a hemoglobin ≤ 10 g/dL, a
serum transferrin saturation ≤ 20%, and a serum ferritin ≤ 200 ng/mL, who were undergoing maintenance hemodialysis 2 to 3 times
weekly. The mean age of the patients enrolled in this study was 41 years, with ages ranging from 16 to 70 years. Of 130 patients evaluated
for efficacy in this study, 68 (52%) were male and 62 (48%) were female. Forty-eight percent of the patients had previously been treated
with oral iron. Exclusion criteria were similar to those in studies A and B. Venofer was administered in doses of 100 mg during sequential
dialysis sessions until a pre-determined (calculated) total dose of iron was administered. A 50 mg dose (2.5 mL) was given to patients
within two weeks of study entry as a test dose. Twenty-seven patients (20%) were receiving erythropoietin treatment at study entry and
they continued to receive the same erythropoietin dose for the duration of the study.
The modified intention-to-treat (mITT) population consisted of 131 patients. Increases from baseline in mean hemoglobin (1.7 g/dL),
hematocrit (5%), serum ferritin (434.6 ng/mL), and serum transferrin saturation (14%) were observed at week 2 of the observation
period and these values remained increased at week 4 of the observation period.
14.4 Study D: Non-Dialysis Dependent-Chronic Kidney Disease (NDD-CKD)
Study D was a randomized, open-label, multicenter, active-controlled study of the safety and efficacy of oral iron versus Venofer in
patients with NDD-CKD with or without erythropoietin therapy. Erythropoietin therapy was stable for 8 weeks prior to randomization. In
the study 188 patients with NDD-CKD, hemoglobin of ≤ 11.0 g/dL, transferrin saturation ≤ 25%, ferritin ≤ 300 ng/mL were randomized
to receive oral iron (325 mg ferrous sulfate three times daily for 56 days); or Venofer (either 200 mg over 2 to 5 minutes 5 times within
14 days or two 500 mg infusions on Day 1 and Day 14, administered over 3.5 to 4 hours). The mean age of the 91 treated patients in
the Venofer group was 61.6 years (range 25 to 86 years) and 64 years (range 21 to 86 years) for the 91 patients in the oral iron group.
A statistically significantly greater proportion of Venofer subjects (35/79; 44.3%) compared to oral iron subjects (23/82; 28%) had an
increase in hemoglobin ≥ 1 g/dL at anytime during the study (p = 0.03).
14.5 Study E: Peritoneal Dialysis Dependent-Chronic Kidney Disease (PDD-CKD)
Study E was a randomized, open-label, multicenter study comparing patients with PDD-CKD receiving an erythropoietin and intravenous
iron to patients with PDD-CKD receiving an erythropoietin alone without iron supplementation. Patients with PDD-CKD, stable
erythropoietin for 8 weeks, hemoglobin of ≤ 11.5 g/dL, TSAT ≤ 25%, ferritin ≤ 500 ng/mL were randomized to receive either no iron or
Venofer (300 mg in 250 mL 0.9% NaCl over 1.5 hours on Day 1 and 15 and 400 mg in 250 mL 0.9% NaCl over 2.5 hours on Day 29). The
mean age of the 75 treated patients in the Venofer / erythropoietin group was 51.9 years (range 21 to 81 years) vs. 52.8 years (range 23
to 77 years) for 46 patients in the erythropoietin alone group.
Patients in the Venofer / erythropoietin group had statistically significantly greater mean change from baseline to the highest hemoglobin
value (1.3 g/dL), compared to subjects who received erythropoietin alone (0.6 g/dL) (p < 0.01). A greater proportion of subjects treated
with Venofer / erythropoietin (59.1 %) had an increase in hemoglobin of ≥ 1 g/dL at any time during the study compared to the subjects
who received erythropoietin only (33.3%).
14.6 Study F: Iron Maintenance Treatment Dosing in Pediatric Patients Ages 2 years and Older with Chronic Kidney Disease
Study F was a randomized, open-label, dose-ranging study for iron maintenance treatment in pediatric patients with dialysis-dependent or
non-dialysisdependent CKD on stable erythropoietin therapy. The study randomized patients to one of three doses of Venofer (0.5 mg/kg,
1.0 mg/kg or 2.0 mg/kg). The mean age was 13 years (range 2 to 20 years). Over 70% of patients were 12 years or older in all three
groups. There were 84 males and 61 females. About 60% of patients underwent hemodialysis and 25% underwent peritoneal dialysis in
all three dose groups. At baseline, the mean hemoglobin was 12 g/dL, the mean TSAT was 33% and the mean ferritin was 300 ng/mL.
Patients with HDD-CKD received Venofer once every other week for 6 doses. Patients with PDD-CKD or NDD-CKD received Venofer once
every 4 weeks for 3 doses. Among 131 evaluable patients with stable erythropoietin dosing, the proportion of patients who maintained
hemoglobin between 10.5 g/dL and 14.0 g/dL during the 12-week treatment period was 58.7%, 46.7%, and 45.0% in the Venofer 0.5 mg/kg,
1.0 mg/kg, and 2.0 mg/kg groups, respectively. A dose-response relationship was not demonstrated.
16. HOW SUPPLIED/STORAGE AND HANDLING
16.1 How Supplied
Venofer is supplied sterile in 10 mL, 5 mL, and 2.5 mL single-use vials. Each 10 mL vial contains 200 mg elemental iron, each 5 mL vial
contains 100 mg elemental iron, and each 2.5 mL vial contains 50 mg elemental iron (20 mg/mL).
NDC-0517-2310-05
NDC-0517-2310-10
200 mg/10 mL Single-Use Vial
200 mg/10 mL Single-Use Vial
Packages of 5
Packages of 10
NDC-0517-2340-01
NDC-0517-2340-10
NDC-0517-2340-25
100 mg/5 mL Single-Use Vial
100 mg/5 mL Single-Use Vial
100 mg/5 mL Single-Use Vial
Individually Boxed
Packages of 10
Packages of 25
NDC-0517-2340-99
100 mg/5 mL Single-Use Vial
Packages of 10
NDC-0517-2325-10
NDC-0517-2325-25
50 mg/2.5 mL Single-Use Vial
50 mg/2.5 mL Single-Use Vial
Packages of 10
Packages of 25
16.2 Stability and Storage
Contains no preservatives. Store in original carton at 20° to 25°C (68° to 77°F); excursions permitted to 15° to 30°C (59° to 86°F). [See
USP Controlled Room Temperature]. Do not freeze.
Syringe Stability: Venofer, when diluted with 0.9% NaCl at concentrations ranging from 2 mg to 10 mg of elemental iron per mL, or
undiluted (20 mg elemental iron per mL) and stored in a plastic syringe, was found to be physically and chemically stable for 7 days at
controlled room temperature (25°C ± 2°C) and under refrigeration (4°C ± 2°C).
Intravenous Admixture Stability: Venofer, when added to intravenous infusion bags (PVC or non-PVC) containing 0.9% NaCl at
concentrations ranging from 1 mg to 2 mg of elemental iron per mL, has been found to be physically and chemically stable for 7 days at
controlled room temperature (25°C ± 2°C).
Do not dilute to concentrations below 1 mg/mL.
Do not mix Venofer with other medications or add to parenteral nutrition solutions for intravenous infusion.
Parenteral drug products should be inspected visually for particulate matter and discoloration prior to infusion.
17. PATIENT COUNSELING INFORMATION
Prior to Venofer administration:
• Question patients regarding any prior history of reactions to parenteral iron products
• Advise patients of the risks associated with Venofer
• Advise patients to report any symptoms of hypersensitivity that may develop during and following Venofer administration, such
as rash, itching, dizziness, light-headedness, swelling, and breathing problems [see Warnings and Precautions (5)]
IN2340ADV
Venofer is manufactured under license from Vifor (International) Inc., Switzerland.
PremierProRx® is a registered trademark of Premier, Inc., used under license.
6/8/2016 4:01:41 PM