Survey
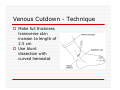
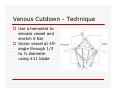
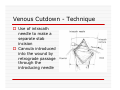
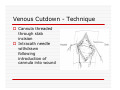
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
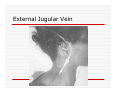
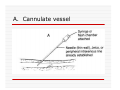
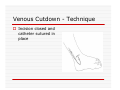
USE OF INTRAVENOUS ACCESS IN RESUSCITATION SITES, TECHNIQUES, POTENTIAL COMPLICATIONS OBJECTIVES Overview Peripheral Venous Access Sites Techniques Potential Complications Central Lines Sites Seldinger Technique Potential Complications Venous Cutdown Sites Techniques Potential Complications OVERVIEW Minimum of two large caliber IVs (1416 Gauge) U/E peripheral IV preferred When establishing IV, blood should be drawn Avoid veins that drain from neck trauma, into an affected traumatic extremity, or the side of a chest or abdominal trauma U/E Peripheral IV - Anatomy Success of cannulation depends on knowledge of anatomy Antero-Radial side forearm – Cephalic vein Ulnar posterior forearm – Basilic vein –easily accessed if elbow flexed and cannulator stands at head of patient U/E Peripheral IV - Anatomy Antecubital veins – Medial Cubital, Basilic, Cephalic Easily cannulated – but restricted elbow motion Above elbow – larger Basilic and Cephalic veins – more difficult to see U/E Peripheral IV - Anatomy L/E Peripheral IV - Anatomy Dorsal venous arch splits into the greater saphenous vein medially and the lesser saphenous vein laterally Greater saphenous vein most easily accessible at the ankle, but may also be cannulated below the knee and below femoral triangle L/E Peripheral IV - Anatomy Greater saphenous vein passes 1 cm anterior to medial malleolus where it lies next to the periosteum L/E Peripheral IV - Anatomy External Jugular Vein Formed below the ear and behind the angle of the mandible, passes obliquely across the sternocleidomastoid, under the middle of the clavicle to join the subclavian vein Presence of valves Flow dependent on neck position External Jugular Vein Materials Required for Peripheral IV Line Insertion Alcohol pads Tourniquet Gauze Tegaderm Intravenous catheter 1-in tape ¼-in tape Gloves Inspection and Positioning Place a 1 inch tourniquet on the upper arm Palpate with index and middle fingers of nondominant hand Tourniquet Cannulation Clean site with Alcohol Stabilize the vein – position thumb alongside vein and pull down. Place index finger more cephalad and push upward Agiocath between thumb and forefinger of dominant hand, bevel up, angled 10-30 degrees, parallel to vein Cannulation When flash is seen, advance catheter a few millimeters more to ensure it has entered vein, not just wall Loosen stylet - advance catheter only Occlude vein at tip of catheter, remove needle, attach IV line, release tourniquet Blood samples may be drawn at this time Cannulation Securing the IV External Jugular Cannulation Place patient in Trendelenberg to fill External Jugular Rotate head to opposite side Align cannula in the direction of the vein with point aimed toward ipsilateral shoulder Puncture midway between angle of jaw and midclavicular line, lightly compressing the vein above the clavicle Complications - Peripheral IV Phlebitis Extravasation Nerve Damage Air Embolism Bruising Thrombosis Phlebitis Presence of palpable cord accompanied by warmth, erythema, tenderness, and induration Extravasation Infiltration relatively minor and common complication of IV therapy If infusions hypertonic, vasopressors or chemotherapies – risk of skin sloughing If dopamine or norepinephrine extravasates, phentolamine may be used as antidote – skin injected with small aliquots of 50:50 dilution Extravasation of Phenytoin Air Embolism Significant, but rare Symptoms of Chest pain, SOB, Sudden vascular collapse, Cyanosis, Hypotension If suspected, place pt in LLD with head and chest tilted downward Central Lines Subclavian Internal Jugular Femoral Subclavian Vein - Anatomy Continuation of axillary vein at outer edge of first rib Joins IJ to become innominate vein 34 cm proximally Valveless After crossing first rib, lies posterior to the medial third of the clavicle Anterior scalene muscle is posterior to vein, anterior to subclavian artery Subclavian Vein - Anatomy Phrenic nerve runs over anterior surface of scalene and immediately behind the junction of subclavian and IJ veins Thoracic duct (L) and lymphatic duct ®, pass over anterior scalene muscle and enter subclavian near junction with IJ Internal Jugular - Anatomy Emerges in neck deep to posterior belly of digastric muscle At origin, courses adjacent to spinal accessory, vagus, and hypoglossal nerves as well as internal carotid artery Tributary veins enter IJ at level of hyoid bone Internal Jugular - Anatomy IJ, ICA, and Vagus nerve course together in carotid sheath…..IJ is antero-lateral Lateral & slightly anterior to carotid Level of thyroid cartilage, IJ just deep to SCM Emerges from under apex of triangle of two heads of SCM Joins subclavian behind clavicle Internal Jugular - Anatomy Lower cervical region, carotid deep paratracheal location Brachial plexus separated from IJ by scalenus anterior Phrenic nerve anterior to scalenus anterior muscle Stellate ganglion anterior to lower brachial plexus Femoral Vein - Anatomy Just medial to the femoral artery below inguinal ligament Beneath lies psoas muscle and hip As progress more distal, femoral vein becomes posterior to femoral artery NAVEL Seldinger Technique Thin walled needle used to access vessel lumen Once introducing needle positioned in vessel lumen, guidewire is threaded through the needle and needle removed Wire serves as guide over which selected catheter placed. Seldinger Technique Introducing needle large enough to accommodate guidewire is attached to a small syringe. Needle and syringe introduced together When free return of blood, remove syringe, stabilize needle hub Cap needle hub with thumb to decrease risk air embolism A. Cannulate vessel Seldinger Technique Flexible end of guidewire threaded through the needle Wire should thread smoothly through vein without resistance If resistance met, remove wire from needle and reattach syringe to confirm intravascular placement If resistance to wire removal, wire & needle should be removed together Seldinger Technique If threading easily, advance guidewire until at least one quarter in vessel Once wire in vessel, remove needle Make small skin incision at site of wire. Incision should be width of catheter to be inserted and extend completely through the dermis B. Thread wire through vessel C. Remove needle D. Enlarge skin entry with #11 scalpel Seldinger Technique Stabilize guidewire at point of skin entry and thread dilator/sheath over wire until 1 cm from skin Before dilator/sheath enters skin, wire must protrude out back of dilator Wire must be grasped as dilator/sheath advanced If wire not protruding from prox end of dilator, pull at skin entry point E. Catheter sheath and dilator threaded over wire F. If prox wire not visible, pull from skin through catheter until out back H. Once sheath and dilator well into vessel, remove dilator and wire Catheter Insertion Length based on Height R Subclavian = (Hgt/10)-2cm L Subclavian = (Hgt/10)+2cm RIJ = Hgt/10 LIJ = (Hgt/10) + 4cm Subclavian, Infraclavicular Approach Place patient supine with head neutral +/- arm abduction, small towel or pillow between shoulder blades to retract shoulder Trendelenburg (10-15o ) decreases risk air embolism Lower pleural dome Right + no thoracic duct Right = preferred side Subclavian, Infraclavicular Approach Cleanse the skin well Apply sterile gloves and drape area If patient is awake, use a local anesthetic at the venipuncture site Introduce a large calibre needle attached to a 12 mL syringe (containing 1mL saline) - 1 cm below junction of middle and medial thirds of clavicle Subclavian, Infraclavicular Approach Here, vein lies just posterior to clavicle and just above first rib Needle bevel should be oriented infero-medially Before needle insertion, left index finger is placed in the suprasternal notch and thumb is positioned at the costoclavicular junction Subclavian, Infraclavicular Approach Hold needle and syringe in the frontal plane Direct needle medially, slightly cephalad, and posteriorly behind the clavicle toward the posterior, superior angle to the sternal end of the clavicle (toward finger placed in suprasternal notch) Subclavian, Infraclavicular Approach Slowly advance the needle while gently withdrawing the plunger of the syringe When free flow of blood appears, remove the syringe and occlude the needle with a finger to prevent and air embolism Insert guidewire while monitoring ECG for abnormalities Subclavian, Infraclavicular Approach Remove needle while holding guidewire in place Insert catheter over guidewire to predetermined depth Connect catheter to IV tubing Affix catheter to skin (suture) Dress area, tape IV tubing CXR - line position, R/O Pneumo Subclavian, Supraclavicular Approach Goal to puncture subclavian vein in superior aspect as it joins IJ Needle inserted above and behind clavicle, lateral to SCM Right side preferred – lower pleural dome, no thoracic duct, direct route to SVC Trendelenburg position, prep and drape area Subclavian, Supraclavicular Approach Entry point 1 cm lat to clavicular head of SCM and 1 cm posterior to clavicle Aim needle to bisect clavicosternomastoid angle - tip pointing caudal to contralateral nipple Orient bevel medially Tip of needle pointed 10o above horizontal & 45o to saggital Vessel puncture at depth of 2-3 cm Internal Jugular Approach Three different IJ approaches: Central, Posterior, Anterior Position in 15-30o Trendelenburg, head turned slightly away (If c-sp cleared) Cleanse skin well and drape area Apply sterile gloves If patient awake, use local anaesthetic at venipuncture site Internal Jugular – A. Central Approach Identify triangle formed by clavicle and sternal and clavicular heads of SCM Use marking pen to indicate lateral border of carotid pulse Introduce a large calibre needle attached to a 12 mL syringe with 0.51 mL of saline, into center of triangle Internal Jugular – A. Central Approach Direct needle caudally at an angle 30o posterior to frontal plane, parallel to course of carotid artery Slowly advance needle while gently withdrawing on syringe plunger When free flow of blood appears in syringe, remove syringe and occlude needle with a finger Internal Jugular – A. Central Approach Insert guidewire while monitoring ECG for rhythm abnormalities Remove needle, advance catheter, remove guidewire, connect to IV Suture catheter in place, apply dressing CXR – line position, R/O pneumo Internal Jugular – B. Posterior Approach Skin entered at lateral edge of SCM 1/3 from clavicle to mastoid process Direct needle caudally and medially toward sternal notch Internal Jugular – C. Anterior Approach Identify course of carotid artery and mark with middle and index fingers Needle should enter skin at midpoint of medial aspect of SCM Direct needle at angle 30-45o to coronal plane, caudally toward ipsilateral nipple Femoral Approach Position pt supine Cleanse skin and drape area Apply sterile gloves Palpate femoral artery…vein is medial Keeping a finger on the artery, introduce a large calibre needle attached to a 12 mL syringe with 0.51 mL of saline Femoral Approach Needle directed toward patient’s head, should enter skin directly over femoral vein at 45o angle Needle should be held parallel to the frontal plane Direct needle cephalad and posteriorly, slowly advancing the needle while withdrawing on syringe Femoral Approach When free flow blood appears in syringe, remove syringe & occlude needle with finger Insert guidewire and remove needle Advance catheter, remove guidewire, connect to IV Suture catheter in place, apply dressing CXR & Abd Xray- identify position/placement Complication of Central Venous Access - General Vascular Air embolus Adjacent artery puncture Pericardial tamponade Catheter embolus Mural thrombus formation Large vein obstruction Local hematoma Arteriovenous fistula Complication of Central Venous Access - General Infectious Generalized sepsis Local cellulitis Osteomyelitis Septic arthritis Complication of Central Venous Access - General Miscellaneous Dysrhythmias Catheter knotting Catheter malposition Complications of Subclavian and Internal Jugular Approaches Pulmonary Pneumothorax Hemothorax Hydrothorax Chylothorax Hemomediastinum Hydromediastinum Neck hematoma and tracheal obstruction Tracheal perforation Endotracheal cuff perforation Complications of Subclavian and Internal Jugular Approaches Neurologic Phrenic nerve injury Brachial plexus injury Cerebral infarct Complications of Femoral Approach General (ATLS) DVT Arterial or neurologic injury Infection AV fistula Intra-abdominal Bowel perforation Bladder perforation Psoas abscess Venous Cutdown Acceptable alternative when unable to perform percutaneous IV insertion No longer mandatory in ATLS due to speed of central venous access techniques Greater Saphenous Vein Longest vein, superficial through most of course Most easily accessible at ankle…crosses one cm anterior to medial malleolus and continues up anteromedial aspect of leg Can expose vessel at ankle : 2 cm ant & superior to medial malleolus Can expose vessel 1-4 cm below knee and just post to tibia (rare) Can expose vessel 3-4 cm distal to inguinal ligament Basilic Vein Preferred site for venous cutdown in Upper Extremity Generally exposed 2.5 cm lateral to the medial epicondyle Venous Cutdown - Equipment Curved Kelly hemostat Scalpel with #11 blade Small mosquito hemostat Tissue spreader Iris scissors Plastic venous dilator 4-0 silk suture ties 4-0 nylon suture Gauze Tape Arm board IV catheter Venous Cutdown - Technique Prepare skin Drape area Infiltrate skin over vein with 0.5% lidocaine Venous Cutdown - Technique Make full thickness transverse skin incision to length of 2.5 cm Use blunt dissection with curved hemostat Venous Cutdown - Technique Identify vein and dissect it free Elevate and dissect the vein for a distance of ~ 2cm, free it from its bed Venous Cutdown - Technique Hemostat can be used to pass proximal and distal ties for stabilization of vein Distal ligature may be tied Venous Cutdown - Technique Use a hemostat to elevate vessel and stretch it flat Incise vessel at 45o angle through 1/3 to ½ diameter using #11 blade Venous Cutdown - Technique Use of intracath needle to make a separate stab incision Cannula introduced into the wound by retrograde passage through the introducing needle Venous Cutdown - Technique Cannula threaded through stab incision Intracath needle withdrawn following introduction of cannula into wound Venous Cutdown - Technique Identification of vessel lumen may be facilitated through use of a plastic venous dilator or elevator Small pointed tip threaded into vessel to expose the lumen Venous Cutdown - Technique In larger veins, a mosquito hemostat can facilitate the placement of the cannula by opening the lumen and providing countertraction Venous Cutdown - Technique Incision closed and catheter sutured in place Venous Mini-Cutdown - Technique Locate vessel with skin incision and blunt dissection Puncture vein under direct vision with percutaneous venous catheter Needle introduced through a separate stab incision Venous Mini-Cutdown - Technique Over the needle or through the needle catheters may be used Eliminates need for tying or cutting the vein Venous Cutdown - Complications Cellulitis Hematoma Phlebitis Perforation of posterior wall of vein Venous thrombosis Nerve transection Arterial transection