Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
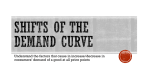
how I do it ENTSO07_85_132:Layout 1 N asal obstruction, for the Rhinology clinic, is a frequently presented symptom and has been shown to adversely affect patients’ quality of life.1 It is a troublesome problem for the surgeon as well as the patient. There are a number of possible anatomical causes for this symptom: frequent. Here we aim to present a summary of endoscopic inferior turbinectmy by discussing both the anatomy and physiology, and also the pathophysiology of this technique. We then move onto the Mr KW S Ah-See pre-op assessment, technique and post-op treatment. Consultant Otolaryngologist-Head and Neck Surgeon, Aberdeen Royal Infirmary, Foresterhill, Aberdeen, AB25 2ZN, UK. Tel: +44 (0)122 455 3571, Email: [email protected] Contributors to ‘How I Do It’ Mr B Ram, Consultant ENT Surgeon, Aberdeen Royal Infirmary, UK. Mr J Newton, ENT SpR, East of Scotland ENT rotation, currently based at Aberdeen Royal Infirmary, UK. Mr M Shakeel, ENT career SHO, Aberdeen Royal Infirmary, UK. 86 Page 86 enlarged inferior turbinates, deviated nasal septum, and a narrow internal nasal valve area are the most Mr KW Ah-See, MD, FRCS, FRCS(ORL), Declaration of Competing Interests None declared. 09:46 Endoscopic Inferior Turbinectomy ‘How I Do It’ is compiled by Correspondence Mr B Ram, Aberdeen Royal Infirmary, Aberdeen, AB25 2ZN, UK. 23/8/07 Inferior turbinate enlargement can be secondary to mucosal hypertrophy or bony hypertrophy – or both. If the bone is involved then it causes a permanent obstruction while there will be fluctuation in nasal obstruction in mucosal hypertrophy. Conservative treatment in the form of steroids, antihistamines and decongestants are usually successful, however some patients are refractory to medical therapy. Reduction of the inferior turbinates has been performed for more than 100 years. The aim of surgery is to correct the anatomical abnormality and consequently improve nasal obstruction and restore normal breathing and drainage. In addition, this also potentiates the medical management of rhinitis, by improvement of delivery of the topical medications to the superior nasal cavity.2 Effective turbinate reduction surgery can be a challenge and many techniques have been developed to achieve this. Partial turbinectomy, radical turbinectomy, laser therapy, electrocautery, cryotherapy, submucosal resection, and submucosal resection with lateral displacement3 all have their advocates. Anatomy and Physiology Inside the nasal cavity, there are three bony projections from the lateral nasal wall called turbinates or conchae (the superior, middle and inferior turbinates). The superior and middle turbinates are part of the ethmoid bone. The inferior turbinate is a separate bone,4 which does not extend all the way into the fleshy posterior tip.5 The inferior turbinate is 60mm long, 7.5mm high and 4mm wide. The arterial supply to the inferior turbinate mainly comes from the descending branch of the sphenopalatine artery, which enters the superior aspect of the inferior turbinate up to 15mm from the posterior tip. This artery then divides into a smaller posterior branch, which lies entirely within the soft tissue supplying the posterior tip, and two larger anterior branches, which supply to the rest of the turbinate. The sensory nerve supply of the turbinates comes from the anterior palatine nerve and the lateral nasal nerve. The sympathetic fibres originate from the first and second thoracic segments of the spinal cord. The parasympathetic preganglionic fibres arise from the superior salivatory nucleus. The turbinates are lined by pseudostratified ciliated columnar epithelium containing numerous goblet cells. The mucous membrane covering the middle and inferior turbinates contain additional venous sinusoids located between the capillaries and venules. Pathophysiology The internal nasal valve area is bounded by septum medially and laterally by the caudal edge of the upper lateral cartilage. The anterior end of the inferior turbinate lies in the internal nasal valve area and any degree of hypertrophy affecting it greatly increases the airflow resistance and consequently causes nasal obstruction. Studies have shown that mucosal swelling is not solely responsible for nasal obstruction in enlargements of the inferior turbinate.6 Bony hypertrophy plays a large role and this supports trimming as the treatment of choice. Pre-op assessment A detailed history is taken and a thorough ENT examination is performed: anterior rhinoscopy as well as rigid nasendoscopy is mandatory. A computed tomography (CT) scan can be done in selected cases to find out the state of paranasal sinuses. Technique Local anaesthetics may be suitable for minor procedures to the turbinates, but trimming of the turbinates requires a full general anaesthetic. The anaesthetist should pay particular attention to protection of the airway from blood, using either an oro-tracheal tube with pharyngeal packing or a laryngeal mask. The patient is prepared for a standard endonasal procedure using the following preparations. On the ward 30 minutes pre-operatively the patient’s nose is packed loosely with ribbon guaze (impregnated with lidocaine hydrochloride 5% with phenylephrine hydrochloride 0.5%). After induction of anaesthesia, xylometazoline 0.1% (otrivine) is poured into both nares. Finally the inferior turbinates are infiltrated ENTNews | SEPT/OCT 2007 | VOL 16 NO 4 ENTSO07_85_132:Layout 1 23/8/07 09:47 Page 87 how i do it 2 1 5 3 Bony hypertrophy plays a large role and this supports trimming as the treatment of choice 4 6 8 Figure 1: Pre-operative appearance of left inferior turbinate. Figure 2: Injecting Lignospan into anterior end of inferior turbinate. Figure 3: In-fracture of inferior turbinate. Figure 4: Trimming of turbinate. Figure 5: Removal of excised turbinate. 7 Figure 6: Securing haemostasis after trimming. Figure 7: Securing haemostasis after trimming. Figure 8: Post-operative appearance: posterior stump demonstrated. ENTSO07_85_132:Layout 1 23/8/07 09:49 Page 88 how i do it Bent anterior end of suction diathermy. with 1:80,000 adrenaline with 2% lidocaine hydrochloride (Lignospan Special) to the anterior and middle thirds. An initial assessment of the nasal anatomy is carried out using the 0° 4mm nasal endoscope. Once the diagnosis has been confirmed and other nasal pathology excluded, the inferior turbinate is in-fractured using a Hill’s elevator. This allows easier access to the lateral aspect or the inferior meatus. At this stage some surgeons use a straight artery clip, placed along the length of the inferior turbinate to crush the hypertrophied and vascular mucosa – but the authors feel this is unnecessary if the nose is adequately prepared. Turbinectomy scissors are then used to cut along the turbinate, from anterior to posterior, staying as near the lateral nasal wall as possible. The small posterior remnant of the turbinate is left in place. The excised turbinate is then removed using forceps. The suction diathermy (see above) is then introduced, with the distal end bent at an angle of around 15°. With adequate suction, the whole length of the turbinate is cauterised until haemostasis is achieved. The contralateral side is then completed in the same way and Naseptin cream is applied to the turbinate stump. The major potential complication is primary haemorrhage. Dryness, crusting, synaechiae formation, excessive secretions, foul discharge, bone exposure, osteitis, empty nose syndrome (atrophic rhinitis) and epiphora are also recognised complications. Rare neurological sequelae include greater palatine nerve dehiscence and partial oculomotor and trigeminal nerve palsy.7 Confining the trimming to the anterior and middle parts of the inferior turbinate offers the advantage of lower incidence of haemorrhage.8 Post-op period There is no requirement for routine post-operative nasal packing. The patient is discharged the following day on regular saline douches, Xylometazoline 0.1% for one week and oral analgesia. The patient is reviewed after two weeks to remove the crusting and at further two-weekly intervals until the crusting is minimal. 88 Rare neurological sequelae include greater palatine nerve dehiscence and partial oculomotor and trigeminal nerve palsy Our experience The senior author has performed 142 procedures between April 2003 and June 2007. Two patients developed secondary bleeding that settled with conservative management. There are no reports of cases of atrophic rhinitis documented in these patients. References 1. Juniper EF. Impact of upper respiratory allergic diseases on quality of life. J Allergy Clin Immunol. 1998;101(suppl):S386-91. 2. Dowley AC, Homer JJ. The effect of inferior turbinate hypertrophy on nasal spray distribution to the middle meatus. Clin. Otolaryngol. 2001;26:488-90. 3. Passali D, Passali FM, Damiani V, Passali GC, Bellussi L. Treatment of inferior turbinate hypertrophy: A randomized clinical trial. Ann Otol Rhinol Laryngol. 2003;112:683-8. 4. Martinez SA, Nissen AJ, Stock CR, Tesmer T. Nasal turbinate resection for relief of nasal obstruction. Laryngoscope 1983;93:871-5. 5. Padgham N, Vaughan-Jones R. Cadaver studies of the anatomy of arterial supply to the inferior turbinate. J R Soc Med. 1991;12:728-30. 6. Berger G, Hammel I, Berger R, Avraham S, Ophir D. Histopathology of the inferior turbinate with compensatory hypertrophy in patients with deviated nasal septum. Laryngoscope 2000;110:2100-5. 7. Magarey MJR, Jayaraj SM, Saleh HA, Sandison A. Ball valve nasal obstruction following incomplete inferior turbinectomy. J Laryngol Otol. 2004;118(2):146-7. 8. Garth RJ, Cox HJ, Thomas MR. Haemorrhage as a complication of inferior turbinectomy: a comparison of anterior and radical trimming. Clinical Otolaryngology & Allied Sciences 1995;20(3):236-8. ENTNews | SEPT/OCT 2007 | VOL 16 NO 4