Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Gastroenteritis wikipedia , lookup
Typhoid fever wikipedia , lookup
Marburg virus disease wikipedia , lookup
Oesophagostomum wikipedia , lookup
Brucellosis wikipedia , lookup
Neglected tropical diseases wikipedia , lookup
Sexually transmitted infection wikipedia , lookup
Middle East respiratory syndrome wikipedia , lookup
Bioterrorism wikipedia , lookup
Whooping cough wikipedia , lookup
Chagas disease wikipedia , lookup
Onchocerciasis wikipedia , lookup
Visceral leishmaniasis wikipedia , lookup
Schistosomiasis wikipedia , lookup
Leishmaniasis wikipedia , lookup
Leptospirosis wikipedia , lookup
Coccidioidomycosis wikipedia , lookup
Eradication of infectious diseases wikipedia , lookup
African trypanosomiasis wikipedia , lookup
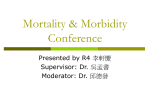
Na tio REDUCING THE IMPACT OF MENINGOCOCCAL DISEASE IN ADOLESCENTS AND YOUNG ADULTS na l F A CM ou nd E o at ffe io rin n fo g fr rI nf om ec th tio e us Di FACULTY William Schaffner, MD, Chairman Lee H. Harrison, MD Sheldon L. Kaplan, MD Elizabeth Miller, MD Walter A. Orenstein, MD Georges Peter, MD Nancy E. Rosenstein, MD National Foundation for Infectious Diseases This CME activity has been planned and produced in accordance with the Essential Areas and Policies of the Accreditation Council for Continuing Medical Education (ACCME), and is made possible by an unrestricted educational grant to the National Foundation for Infectious Diseases from sanofi pasteur. Issued: July 2005 Release Date: July 2005 Expiration Date: July 2007 Estimated Time to Complete Activity: 1.5 hours se as es FACULTY William Schaffner, MD, Chairman Professor and Chair, Department of Preventive Medicine Professor of Medicine (Infectious Diseases) Vanderbilt University School of Medicine Nashville, Tennessee Lee H. Harrison, MD Professor of Medicine Infectious Diseases Epidemiology Research Unit University of Pittsburgh School of Medicine Pittsburgh, Pennsylvania Sheldon L. Kaplan, MD Professor and Vice Chairman for Clinical Affairs Department of Pediatrics Baylor College of Medicine Houston, Texas Elizabeth Miller, MD Head of the Immunisation Department Communicable Disease Surveillance Centre Health Protection Agency Centre for Infections London, England Walter A. Orenstein, MD Director, Vaccine Policy and Development Associate Director, Emory Vaccine Center Emory University School of Medicine Atlanta, Georgia Georges Peter, MD Professor, Department of Pediatrics Brown Medical School Founding Director, Division of Pediatric Infectious Diseases Rhode Island Hospital Providence, Rhode Island Nancy E. Rosenstein, MD Chief, Meningitis and Special Pathogens Branch Division of Bacterial and Mycotic Diseases National Center for Infectious Diseases Centers for Disease Control and Prevention Atlanta, Georgia REDUCING THE IMPACT OF MENINGOCOCCAL DISEASE IN ADOLESCENTS AND YOUNG ADULTS Continuing Medical Education Information 1 Introduction 3 Epidemiology of Meningococcal Disease 5 Transmission and Pathogenesis: Examining Risk Factors 7 U.S. Immunization Recommendations 8 Presentations, Progression and Sequelae 11 Conclusion 15 References 16 Self-Assessment Examination 18 CME Evaluation 19 Copyright © 2005 by National Foundation for Infectious Diseases. All Rights Reserved. CONTINUING MEDICAL EDUCATION INFORMATION Target Audience the Centers for Disease Control and Prevention’s Advisory Primary care physicians, pediatricians, infectious Committee on Immunization Practices and the scientific disease specialists, college health professionals and data that provide rationale for an immunization strategy public health officials responsible for or interested in designed to lessen the burden of meningococcal disease. communicable diseases. Educational Format Statement of Need This activity was developed by the faculty based on a Meningococcal disease causes substantial morbidity and literature review and personal knowledge and expertise mortality. Cyclical trends in disease epidemiology suggest about meningococcal disease. that persons across many age groups may be at increased risk of disease and severe complications, including death. 1 U.S. immunization policy and recommendations changed Evaluation and Exam following approval of a conjugate meningococcal vaccine A course evaluation form and self-assessment examination for use in persons aged 11 to 55 years. All physicians and at the end of this monograph will provide participants public health officials interested in communicable with the opportunity to critique the program content and diseases should be aware of the new recommendations by method of delivery, identify future educational needs and possible bias in the presentation materials and complete the self-assessment examination to receive CME credits. OBJECTIVES After completing the monograph, physicians will be able to: Accreditation This activity has been planned and implemented in • Discuss the epidemiology of meningococcal disease in terms of age, serogroup and geographic distribution; accordance with the Essential Areas and Policies of the Accreditation Council for Continuing Medical Education (ACCME) by the National Foundation for Infectious Diseases (NFID). NFID is accredited by the ACCME to • Describe clinical presentations of meningococcal disease; provide Continuing Medical Education (CME) for physicians. NFID takes responsibility for the content, quality and scientific integrity of the CME activity. • Outline U.S. immunization recommendations; NFID designates this CME activity for a maximum of 1.5 • Compare features of conjugate and polysaccharide vaccines. credits toward the AMA Physician’s Recognition Award of the American Medical Association. Each physician should claim only those hours of credit that he/she actually spent on the educational activity. Commercial Support Disclaimer This CME activity is made possible by an unrestricted Any procedures, medications or other courses of diagnosis educational grant from sanofi pasteur to the National or treatment discussed or suggested in this activity should Foundation for Infectious Diseases. not be used by clinicians without evaluation of their patient’s condition, possible contraindications or dangers in use, review of any applicable manufacturer’s product Financial Disclosures information and comparison with recommendations of Lee H. Harrison, MD, has a financial interest/relationship other authorities. with sanofi pasteur in the form of research support, consulting, and speaking fees. Release date: July 2005 Expiration date: July 2007 Sheldon L. Kaplan, MD, has a financial interest/relationship with sanofi pasteur in the form of a research grant, stipend and/or fellowship. 2 Elizabeth Miller, MD, has a financial interest/relationship with Chiron, Wyeth Pharmaceuticals and Baxter in the form of provision of meningococcal surveillance reports for submission to licensing authorities. Walter A. Orenstein, MD, has no significant financial interests or relationships to disclose in relation to this program. Georges Peter, MD, has no significant financial interests or relationships to disclose in relation to this program. Nancy E. Rosenstein, MD, has no significant financial interests or relationships to disclose in relation to this program. William Schaffner, MD, has no significant financial interests or relationships to disclose in relation to this program. © National Foundation for Infectious Diseases, 4733 Bethesda Avenue, Suite 750, Bethesda, Maryland, 20814 INTRODUCTION Following approval of the first conjugate vaccine 11 to 18 years of age (CDC. Unpublished data).2 The against meningococcal disease, the Centers for Disease annual disease rate generally ranges from 0.9 to 1.5 Control and Prevention’s (CDC) Advisory Committee cases per 100,000, but clearly the overall and age-specific on Immunization Practices (ACIP) has broadened its incidence rates are markedly cyclical. meningococcal disease vaccination recommendations.1 The ACIP recommends routine vaccination of young adolescents with the meningococcal conjugate vaccine at the pre-adolescent health care visit (11-12 years of age). Meningococcal Disease Immunization Recommendations For those persons who have not previously received the meningococcal conjugate vaccine, ACIP recommends vaccination before high-school entry (approximately 15 years of age). Routine vaccination is also recommended for college freshmen living in dormitories. By 2008, the goal will be routine vaccination of all adolescents beginning 3 In addition to the ACIP, other important groups have issued recommendations regarding meningococcal disease vaccination. These may be reviewed at the following Web addresses: Advisory Committee on Immunization Practices www.cdc.gov/mmwr/PDF/rr/rr5407.pdf at 11 years of age. This document describes meningococcal disease epidemiology and disease burden among children, adolescents and young adults in the U.S. It also discusses prevention strategies for meningococcal disease, with a focus on recommended use of the quadrivalent conjugate American Academy of Family Physicians www.aafp.org/x34406.xml American Academy of Pediatrics www.cispimmunize.org/pro/pdf/aapmengpolicy.pdf American College Health Association www.acha.org/projects_programs/men.cfm meningococcal vaccine. An overview of the meningococcal conjugate vaccination program in the United Kingdom, implemented in 1999, provides an example of the benefits of widespread conjugate immunization across a population. Meningococcal disease is associated with an overall case fatality rate of 10% to 14%.1 Fatality rates can vary widely, Meningococcal disease is a potentially life-threatening however, depending on prevalence of the disease, the nature infection caused by the bacterium Neisseria meningitidis. of the infection and societal conditions.5 Case fatality rates It affects 1,400 to 2,800 persons in the U.S. annually.1 generally increase with age,6 but again, aberrations have Most cases are sporadic; less than 5% occur in outbreaks.2,3 been noted. During a decade-long span ending in 2002, Incidence is highest in children less than 2 years of age, CDC surveillance reported fatality rates of 12% in those but approximately 50% of cases occur in those over 15 aged 10 to 17 years and 14% in those aged 14 to 24 years years. Temporal and geographic peaks have been noted, (CDC. Unpublished data).2 Beyond mortality, meningococcal however, in various age groups. A study in Maryland found disease is also associated with substantial long-term that in the 1990s, 30% of cases occurred in adolescents morbidity. Of those who survive, 11% to 19% have and young adults.4 During the same period (1991 to 2002), 13% to 14% of disease countrywide was in persons permanent sequelae, such as hearing loss, brain damage, renal failure or limb amputation.1,7,8 Five clinically relevant meningococcal serogroups, A, and college students who wish to reduce their risk of B, C, Y and W-135, are responsible for nearly all disease meningococcal disease may elect to be vaccinated. worldwide. Currently, serogroups B, C and Y cause the majority of U.S. infections; serogroup A is extremely rare Widespread conjugate meningococcal vaccination should in the U.S. and W-135 causes a very small proportion of decrease the risk of meningococcal disease in adolescents infections. However, serogroup distribution has changed and adults. Expectations for conjugate vaccines are based over time. Serogroup Y caused only 2% of U.S. cases in on recent experience. In the U.K., widespread use of the early 1990s but 39% of cases from 1996 to 2001 (this conjugate meningococcal C vaccines has led to sharp specific change appears to be confined to the U.S. thus decreases in meningococcal C disease (which was respon- far). Serogroup distribution also varies by age.3 Serogroup sible for 30% to 40% of cases in the U.K.), reduction in B is the most common serogroup in infants, serogroup bacterial carriage and consequent reduction in incidence C is most common in adolescents and young adults and in unimmunized persons.9,10 In the U.S., universal use serogroup Y causes the majority of cases in those aged of conjugate Haemophilus influenzae type b (Hib) and 65 years and older.2 Similar fluctuations in serogroups are seen worldwide. pneumococcal vaccines has led to sharp decreases in meningitis cases caused by these bacteria.11,12 Because of these immunization successes, meningococcal disease A quadrivalent conjugate meningococcal vaccine is now the most common cause of bacterial meningitis (MCV4), approved for use in persons aged 11 to 55 years among children over 2 years of age, adolescents and young (Menactra®, sanofi adults in the U.S.11 pasteur), is a key addition to existing meningococcal disease prevention measures.1 Like the polysaccharide vaccine, which has been licensed in the United States since 1978, the quadrivalent conjugate offers Several factors make meningococcal protection against four serogroups of N. meningitidis disease a matter of public health importance. (A, C, Y, W-135), the bacteria that cause meningococcal First, it is a communicable disease disease. Successful conjugate vaccine technology, however, offers additional benefits compared with polysaccharide associated with notable morbidity and vaccines, including improved duration of protection, mortality. Second, isolated meningococcal induction of immunologic memory, booster responses and cases and outbreaks often cause serious reduction in nasopharyngeal bacterial carriage. medical and social stress in communities and Routine vaccination is also recommended for groups that are associated with increased costs — both have elevated risk. These groups include microbiologists economic and social. Finally, each case of who are routinely exposed to isolates of N. meningitidis; meningococcal disease requires a public persons who travel to or reside in countries in which health response (i.e., identification of close N. meningitidis is epidemic; military recruits; and those with complement deficiency or functional or anatomic asplenia. In addition to these groups, all other adolescents contacts for prophylaxis). 4 EPIDEMIOLOGY OF MENINGOCOCCAL DISEASE N. MENINGITIDIS is a commensal bacterium of the human The distribution of serogroups causing meningococcal nasopharynx that infrequently causes invasive disease. Up to 10% to 30% of adolescents and young disease (A, B, C, Y, W-135) varies over time and by adults13-15 geographic location.2 From 1988 through 1991, most U.S. and 19% to 39% of adult males (military recruits)15 are cases of meningococcal disease were caused by serogroups asymptomatic, transient nasopharyngeal carriers of N. B and C, with serogroup Y accounting for only 2% of meningitidis, although most carry nonpathogenic strains. cases.3 More recently (1996 through 2001), serogroup Y Asymptomatic carriage rates in young children are much lower (< 2%).14,15 Some carriers develop protective disease caused the largest proportion of cases (39%), followed by serogroup C (31%) and serogroup B (23%).2 antibodies against the organism.16 In a minority of exposed individuals, N. meningitidis penetrates the Although serogroup W-135 is relatively uncommon in the nasopharyngeal mucosa, reaches the bloodstream and U.S. and was not previously known to cause outbreaks, it causes systemic disease.17 played a major role in an outbreak during the Hajj pilgrimage to Mecca in 2000. Four cases of W-135 meningococcal disease were identified in pilgrims returning to the U.S. varied between 0.9 and 1.5 cases per 100,000 persons from Saudi Arabia and their close contacts.18 for 4 decades. Although meningococcal disease occurs throughout the year, incidence peaks in late winter and early spring.11 Serogroup A was a common cause of U.S. epidemics early Rates of meningococcal disease are highest in the last century, but has been rare since World War II. in infancy with a second spike in incidence in adolescence, with a peak at around 18 years of age (Figure 1).2,6 Serogroups A and C continue to predominate throughout Asia and Africa,19 with serogroup A remaining the major Invasive Meningococcal Disease by Age and Sex in the U.S., 1992-1996 responsible for a large meningitis outbreak in Burkina 5 Incidence per 100,000 Figure 1: cause of meningococcal disease in sub-Saharan Africa (the “meningitis belt”).20,21 Even so, serogroup W-135 was Male Female 4 3 Faso in 2002.22 The diversity in geographic distribution of 15 meningococcal serogroups causing disease, while 10 unexplained, is important given the ease and frequency of travel and potential exposure to serogroups other than 5 those common to one’s region of residence. 0 ≤3 4-5 6-11 12-15 16-19 20-23 Age group (months) 2 Overall, serogroups B, C and Y cause a substantial proportion of disease across all ages, but specific distribution 1 varies by age group.3 Recent U.S. data (2002) show that Age (years) Rates of meningococcal disease were adjusted for race. Source: Rosenstein6 ≥85 80-84 75-79 70-74 65-69 60-64 55-59 50-54 45-49 40-44 35-39 30-34 25-29 20-24 15-19 10-14 5-9 infants and toddlers experience a higher proportion of 0-4 Incidence per 100,000 5 The rate of meningococcal disease in the U.S. generally serogroup B disease than older age groups (Figure 2).2 Among young adults (18 to 34 years old), serogroup C is the most common (48% of cases) and in those 65 years and older, serogroup Y is most common (62%). In a The cyclic nature of disease and prospective surveillance study of U.S. college students with meningococcal infection during the 1998–1999 school year, serogroup C was the most common (48% of isolates for which serogroup data were available), followed changing distribution of serogroups, combined with frequency of travel by B, Y and W-135 (28%, 19% and 1%, respectively).23 worldwide, underscore the need N. meningitidis is an aerobic, gram-negative for a prevention strategy that diplococcus. The bacterium has an outer membrane that is surrounded by a protective polysaccharide incorporates all major serogroups. capsule. Thirteen antigenically and chemically unique polysaccharide capsules have been identified and form the basis of serogroup classification of the organism. Five serogroups — A, B, C, Y and 6 W-135 — cause nearly all cases of invasive meningococcal disease. Figure 2: Serogroup Distribution of Invasive Meningococcal Disease by Age Group in the U.S. – Active Bacterial Core Surveillance 2002 B Other Y C 100 90 Percent of Cases 80 70 60 50 40 30 20 10 0 ≤1 2-4 5-17 18-34 Age (years) Source: ABCs2 35-49 50-64 ≥65 TRANSMISSION AND PATHOGENESIS: EXAMINING RISK FACTORS transmission of N. MENINGITIDIS occurs by droplet aero- Likewise, certain environmental factors have been solization (e.g., coughing or sneezing) or direct contact shown to increase the risk of meningococcal disease. with secretions from the nasopharynx of colonized persons. The infection rate (secondary infection) is 500- to Whether the organism remains a colonizer of the 800-fold greater in household contacts exposed to a nasopharynx or crosses the mucosal barrier and gains person who has a sporadic meningococcal infection access to the bloodstream, central nervous system and/or than in the general population.34 Increased risk of other organs depends on both specific bacterial virulence meningococcal infection among military recruits35 and factors (e.g., fimbriae, polysaccharide capsule, IgA college freshmen living in dormitories23 is likely a protease) and host defense mechanisms (e.g., mucosal consequence of crowded living conditions. epithelium, secretory IgA, serum antibody, ciliary activity, complement, blood-brain barrier).24 In the U.S., higher rates of meningococcal disease have been observed in black persons and persons of low 7 Various medical conditions increase the risk of socio-economic status, which are likely surrogate risk developing meningococcal disease. Persons with immature markers (e.g., for household crowding and exposure to or dysfunctional humoral immunity are most susceptible tobacco smoke) rather than inherent genetic risk factors to meningococcal infection.25,26 Immune defects that for disease.36 Active smoking and passive exposure to predispose to meningococcal disease include functional tobacco smoke increase the risk of illness, most likely by or anatomical asplenia, deficiency of properdin and increasing the creation and dissemination of respiratory mannose-lectin binding protein and terminal complement droplets or compromising the respiratory mucosa as a components.27-29 Antecedent barrier to microbial invasion.37 During outbreaks, bar or respiratory tract infection also has been associated with increased risk of meningococcal disease.30,31 Finally, evidence indicates nightclub attendance and alcohol consumption have been identified as risk factors for infection.38-40 genetic risk factors may increase susceptibility to meningococcal infection.32,33 Once N. meningitidis enters the nasopharynx, the organism attaches to and multiplies on nonciliated epithelial cells. Increased risk of meningococcal infection among military recruits and college freshmen living in dormitories is likely a consequence of crowded living conditions. Some exposed individuals become asymptomatic nasopharyngeal carriers of N. meningitidis,13,14 which is an immunizing event. In less than 1% of colonized persons, N. meningitidis penetrates the nasopharyngeal mucosa and causes a systemic infection.17 In the bloodstream, the organism can rapidly produce and release endotoxin, which stimulates cytokine production and the alternative complement pathway.7 In about half of bacteremic persons, N. meningitidis crosses the blood-brain barrier into the cerebrospinal fluid (CSF), and meningitis follows. U.S. IMMUNIZATION RECOMMENDATIONS The quadrivalent meningococcal conjugate vaccine coverage among adolescents. A routine visit at 11-12 years (MCV4, Menactra®) of age to assess immunization status and other preventive is recommended for routine vaccination (Table 1) of young adolescents at the pre-adolescent health care visit (11-12 years of age).1 For those persons who have not previously received MCV4, vaccination is services is recommended by the ACIP, American Academy of Pediatrics (AAP), American Academy of Family Physicians (AAFP) and the American Medical Association (AMA).41 recommended before high-school entry (approximately 15 years of age). Also, if not previously vaccinated, routine Routine meningococcal vaccination is also recommended vaccination is recommended for college freshmen living in for persons in specific risk groups.1 These are microbiolo- dormitories. Finally, other adolescents and college students gists routinely exposed to isolates of N. meningitidis; who wish to decrease their risk for meningococcal disease military recruits; persons who travel to, or reside in may elect to receive the vaccine. countries in which N. meningitidis is hyperendemic or epidemic; persons with terminal complement component The ACIP recommends catch-up vaccination at approxi- deficiencies; and those who have anatomic or functional mately 15 years of age as an effective strategy to reduce asplenia. HIV patients who wish to decrease their risk of meningococcal disease incidence among adolescents and meningococcal disease may elect to be vaccinated. young adults. The routine vaccination recommendation at 11-12 years of age might strengthen the role of the Conjugate Versus Polysaccharide Vaccine pre-adolescent visit and have a positive effect on vaccine Vaccination with MCV4 is preferred for all persons in Table 1: Recommendations for Use of Meningococcal Conjugate Vaccine* • At the pre-adolescent health care visit (11-12 years old) • At high-school entry (approximately 15 years old), if not previously vaccinated with MCV4 • College freshmen living in dormitories • Microbiologists routinely exposed to isolates of N. meningitidis • Military recruits • International travelers and citizens residing in endemic or hyperendemic areas • Persons with anatomic or functional asplenia • Persons with terminal complement component disorders * Approved for use in persons aged 11 to 55 years Source: CDC1 the age range for which it is approved, 11 to 55 years, because of the benefits it should provide compared with polysaccharide vaccine (Table 2).1 Immunogenicity data show MCV4 induces antibody levels at least as good as the polysaccharide vaccine. Both vaccines include protection against four of the five strains (A, C, Y and W-135) that cause the majority of cases worldwide. Neither includes protection against serogroup B disease (see box, “About Serogroup B Vaccines”). Although the vaccines are equally immunogenic, MCV4, which is administered intramuscularly (versus subcutaneous injection of the polysaccharide vaccine) is more reactogenic.1 MCV4 is expected to have a duration of protection of at least 8 years compared with 3 to 5 years for the polysaccharide vaccine. Ongoing studies will provide specific data about duration of protection in the coming years. 8 Table 2: Comparison: Conjugate and Polysaccharide Meningococcal Disease Vaccines 9 Conjugate (Menactra®) Polysaccharide (Menomune®) Strains included A, C, Y, W-135 A, C, Y, W-135 Immunogenicity* 82% to 97% 80% to 95% Duration of protection > 8 years† 3-5 years Administration Intramuscular injection Subcutaneous injection Safety Generally mild adverse reactions; mainly pain, redness and induration at injection site, headache, fatigue and malaise. Generally mild adverse reactions; most frequent is pain and redness at injection site. Severe reaction uncommon. Induction of immunologic memory‡ Expected No Booster responses‡ Expected No Reduction in nasopharyngeal bacterial carriage‡ Expected No Herd immunity‡ Expected under some vaccination strategies No Cost§ $82 $86 * Measured as ≥four-fold rises in antibody titers in adolescents; † Based on CDC model, ongoing evaluation is expected to provide direct data in three to five years; ‡ Assumptions based on demonstrated benefits of other conjugate vaccines § Retail cost to physicians. Sources: CDC1, CDC unpublished data. In fact, extensive post-licensure evaluation of MCV4 will be ongoing. Data collected in the coming years will provide vaccine-specific information and will shape future recommendations. The hope is that this conjugate vaccine provides benefits similar to other conjugate vaccines. About Serogroup B Vaccines In clinical trials, most candidate vaccines against serogroup B polysaccharide have not stimulated Conjugate technology changes the nature of the immune protective immunity in humans.42 Research has response from T-cell independent to T-cell dependent. This focused on noncapsular antigens as vaccine leads to benefits not seen with polysaccharide vaccines, including induction of immunologic memory, booster responses and reduction in nasopharyngeal bacterial carriage. Reduction in asymptomatic carriage rates, if wide- candidates. For example, an outer-membrane protein serogroup B vaccine, licensed for use in New Zealand in 2004, was designed to match spread, leads to protection of unvaccinated individuals and combat an outbreak of serogroup B disease through a herd immunity effect. These benefits have been ongoing throughout the 1990s. However, this demonstrated with use of a monovalent meningococcal approach does not address the diversity of outer- conjugate C vaccine in the U.K. and widespread Hib and membrane proteins that cause sporadic serogroup B disease or geographic variations.43,44 pneumococcal conjugate vaccination in the U.S. (discussed below). Data on similar benefits are not yet available on MCV4. pneumococcal vaccination also appears to have a substantial herd immunity effect. While the vaccine is used only in children, disease rates have declined among adults. For the serotypes included in the vaccine, disease incidence decreased in those aged 20 to 39 years, 40 to 64 years and 65 years and older by 46%, 20% and 29%, respectively (CDC. Unpublished data). The U.K. Experience: Monovalent Meningococcal Conjugate C Vaccine Additional evidence comes from the U.K., where a comprehensive monovalent meningococcal conjugate C vaccine immunization program was implemented in 1999.9 Disease epidemiology in the U.K. differs from that in the U.S.; the U.K. sees very little serogroup Y disease and has a higher incidence of serogroup C infection. Widespread use of the monovalent conjugate C vaccine would be The quadrivalent meningococcal polysaccharide vaccine (Menomune®, sanofi expected to have a greater relative impact in the U.K. pasteur) continues to be recom- mended in children aged 2 to 10 years and adults older The U.K. program includes a routine 3-dose infant than 55 years who are at increased risk of infection. The vaccination course (at 2, 3 and 4 months) with a single polysaccharide vaccine is also an acceptable alternative for dose for children aged 12 months to 17 years (with a persons aged 11 to 55 years if MCV4 is unavailable. subsequent extension to 25 years of age).9 Immunization rates of about 85% in target groups resulted in an 81% Both vaccines are recommended for control of menin- reduction in serogroup C disease incidence within 18 gococcal disease outbreaks, with the conjugate vaccine months. While the vaccine was immunogenic in young preferred for those aged 11 to 55 years. Revaccination may infants, their immunity waned at about 1 year.46 be indicated for those who previously received the polysaccharide vaccine if they remain at high risk for infection Despite this, control of disease in all age groups has been and are aged 11 to 55 years. excellent with disease incidence declining 67% in the unvaccinated population.10 This is attributable to the herd Benefits of Other Conjugate Vaccines immunity arising from the marked reduction in nasopha- Non-meningococcal conjugate vaccines, including Hib ryngeal carriage (a key feature of conjugate vaccines). and a 7-valent pneumococcal, are routinely used in the Nasopharyngeal carriage rates decreased 66% among U.S. Before introduction of the vaccine, Hib disease was students aged 15 to 17 years.47 Surveillance has shown the leading cause of bacterial meningitis in children no evidence of serogroup replacement or development younger than 5 years. Incidence of invasive Hib disease of capsular switching in the first 18 months in the U.K.48 has declined more than 99% since vaccine licensure.45 MCV4 will be used much differently in the U.S. than the Similarly, rates of invasive pneumococcal disease monovalent vaccine is used in the U.K. It is unclear if the in children younger than 2 years have declined 70% to current U.S. immunization strategy will yield a herd 80% since vaccine licensure in 2000.2,12 Conjugate immunity benefit. 10 PRESENTATIONS, PROGRESSION AND SEQUELAE Meningitis and Meningococcemia Meningococcal disease manifests most commonly A 12-year-old African-American boy was rushed to the as meningitis and/or meningococcal bacteremia.7,8 It is emergency room by his parents at 5 p.m. on a Saturday meningococcemia, however, Otherwise healthy, he had had two days of a non-productive a less common but more cough accompanied by malaise, headache and intermittent after they found him unresponsive in the bathroom. severe presentation (5% to 20% of cases) that is associated nausea. He had been seen that morning by his physician with the highest mortality rates and long-term sequelae. who prescribed azithromycin for bronchitis. It had taken Meningococcemia often begins with a sudden onset of some time to fill the prescription and the boy received only fever, malaise, myalgia and headache; seizures occur in one dose of the medication, which he promptly vomited just 20% of cases. About half of dren and young 11 CASE REVIEW: 12-year-old male adults)50 patients49 (even more chil- develop a prominent petechial or purpuric rash, primarily on the extremities. When present, a meningococcal rash can change and spread very rapidly. Meningococcemia may occur either with or without meningitis. The more common clinical presentation, meningococcal meningitis, is often nonspecific. Early symptoms may mimic those of other more common but less serious diseases.5,8 Patients may present with sudden onset of fever, headache, meningismus and signs of cerebral dysfunction. However, before he was discovered in the bathroom. In the emergency department, the boy had no detectable blood pressure and required immediate intubation. A few petechial lesions were evident on the palms and soles of the feet, at the belt line and in the conjunctivae. The peripheral white blood cell count was 25,900/cumm with a profound left shift and a platelet count of 35,500/cumm. Antimicrobials and pressor agents were started immediately. A lumbar puncture revealed a white cell count of 19,340 with 85% neutrophils and a glucose concentration of 16 mg/dl. Both blood and CSF culture grew N. meningitidis. the classic triad of headache, confusion and nuchal rigidity The patient had a prolonged, stormy course. He never is not always evident. Wide variations in presentation can regained consciousness, developed purpura fulminans and occur at all ages, and symptoms can progress and change peripheral gangrene that required bilateral below-the-knee rapidly during the course of the disease. amputation. He died of pulmonary complications after 33 days in the hospital. Infants and the elderly may not present with the classic symptoms and signs of meningococcal meningitis.51 Meningismus is absent in neonates and often in infants.52 One of the most important clues to a meningitis diagnosis in neonates is a change in affect or level of alertness. Clinical suspicion should also be raised by temperature instability, listlessness, high-pitched crying, lethargy, weak suck, refusal to eat, irritability, jaundice, vomiting, diarrhea Teaching Points: Symptoms of meningococcemia can appear suddenly and progress rapidly. Even with rapid diagnosis and appropriate treatment, serious sequelae are possible; deafness being the most common one in children. Meningococcal rashes may appear at areas where pressure occurs from stockings, elastic or belts. or respiratory distress. Elderly patients, especially those with multiple co-morbid diseases, may be afebrile or hypothermic, lethargic or exhibit reduced alertness and Figure 3: Clinical Manifestations of Meningococcal Disease have variable signs of meningeal inflammation. Confusion is common,53 as is a prior or concurrent respiratory tract Bacteremia 43.3% infection. A definitive diagnosis of meningococcal disease is based on isolation of N. meningitidis from a normally Pneumonia 6.0% sterile site (e.g., blood; CSF; joint, pleural or pericardial fluid). Arthritis 2.0% Otitis media 1.0% Meningococcal meningitis is fatal in approximately 10% Epiglottitis 0.3% of cases among the general population; the case fatality Pericarditis 0.1% rate is as high as 53% in patients with meningococcemia.7 Meningitis 47.3% Factors associated with an increased mortality rate include recovery of an isolate from the bloodstream and serogroup C infection.6 Source: Rosenstein6 Other Presentations Up to 15% of patients with meningococcal disease have pneumonia.6,54,55 Meningococcal pneumonia occurs primarily in older adults and is most commonly associated with serogroup Y or W-135 infection.6 Less common mani- festations of disease (<2% of cases) include pericarditis, otitis media, epiglottitis and arthritis (Figure 3).6 Sequelae Even with appropriate therapy, systemic meningococcal infection can progress rapidly — often within hours of the first symptoms. Despite the susceptibility of N. meningitidis to penicillin and advances in medical care, 11% to 19% of patients who survive invasive meningococcal disease suffer from permanent sequelae, including hearing loss, neurologic or brain damage, renal failure and limb amputation.7,8 Prevention of Secondary Disease The primary method of preventing secondary meningococcal disease is antimicrobial prophylaxis of persons in close contact with an infected person (Table 3). Those Table 3: Meningococcal Disease Prophylaxis Recommendations: High-Risk Contacts • Household contact (especially young children) • Child care or nursery school contact* • Direct exposure to secretions of index patient through kissing, sharing toothbrushes or eating utensils (markers of close social contact)* • Mouth-to-mouth resuscitation, unprotected contact during endotracheal intubation* • Frequently slept or ate in same dwelling as index patient* * During 7 days before onset of illness Source: AAP60 12 CASE REVIEW: 18-year-old female An 18-year-old white female attending a state univer- 12,500/cumm with a marked left shift. Although the blood sity (freshman dormitory resident) began to experience culture was negative, the CSF culture was positive for aches and chills while at class during the third week of N. meningitidis, Group C. The patient was hospitalized the semester. The patient assumed she had a mild viral for 8 days and was discharged to the care of her parents illness and returned to the dorm to sleep. Shortly after at home. She re-started her college studies during the dinner, she went to the infirmary complaining of aches second semester. Subsequent testing determined that the and nausea. The patient reported that she came to the patient had sustained a moderate high and mid-range infirmary at the urging of her roommate. The patient was bilateral hearing loss. articulate and mildly febrile (101ºF); she expressed a desire to go back to her room. Infirmary staff agreed and Teaching Points: Early symptoms of meningococcal ordered Tylenol and rest. infection can mimic other mild to generally moderate illnesses (e.g., cold and flu). The onset of symptoms in 13 In the morning, when she did not join her friends at this patient was insidious and, upon her first presentation breakfast, they went to the patient’s room to check on to the infirmary, non-specific. The cognitive dysfunction her. She was in bed, and friends described her as “inco- was not evident until her second visit to the infirmary. herent” and “confused.” The friends brought the patient Meningococcal disease was not immediately evident back to the infirmary where staff noticed a rash on her (e.g., she had no rash or high fever) upon her initial pre- torso. Transport to a local hospital took approximately 35 sentation in the university infirmary. Therapy should be minutes. started upon suspicion of meningococcal infection and not withheld pending results of cultures. Antibiotics were started within 15 minutes of arrival in the emergency department. The white blood cell count was most in need of chemoprophylaxis against meningococcal meningococcal disease (Table 4).11,60 One study showed infection include household members, daycare center azithromycin is also effective in eradicating nasopharyngeal contacts and persons directly exposed to the oral carriage.61 Persons with invasive meningococcal disease secretions of a patient with invasive meningococcal treated with agents other than ceftriaxone or other third- infection. Antimicrobial prophylaxis of at-risk persons generation cephalosporins should also receive one of the should be initiated within 24 hours after the index chemoprophylactic antibiotics before hospital discharge.62 infection is identified, if possible.11 Outbreak Control Oral rifampin and ciprofloxacin and parenteral ceftriaxone Given the devastating nature of meningococcal disease, substantially reduce (by 90% to 95%) nasopharyngeal sporadic cases often become the topic of front-page and carriage of TV news. Such cases elicit community fear and increased N. meningitidis56-59 and are therefore recommended by the ACIP and the AAP for prophylaxis of telephone calls and visits to treatment centers. Public health departments are faced with assessing potential associated with this intervention are high compared with outbreaks, determining the need for and designing many other recommended preventive measures.63 A similar appropriate control procedures and fielding public analysis examining routine vaccination in college freshmen inquiries. Requests for chemoprophylaxis and vaccination also highlighted the high cost of a widespread meningo- are common, even among those without close contact coccal vaccination program.64 Both analyses included a with infected persons. wide range of costs associated with each meningococcal disease case. The high end of these ranges demonstrates The decision to implement mass vaccination is the potential for serious disease sequelae and even death complicated.11 that accompany each infection. Such vaccination campaigns are expensive, require considerable public health effort and can create unwarranted public concern. Still, mass vaccination may Although data about the economic impact of meningococcal be necessary to prevent the substantial morbidity and disease are imperfect, older CDC data estimated the direct mortality associated with meningococcal disease. The cost of meningococcal disease at $13,431 per case (1995 CDC has issued guidelines, including criteria for deciding dollars).65 The estimated lifetime costs of sequelae ranged whether use of meningococcal vaccine is warranted from $44,187 per case (hearing loss) to $864,980 (severe (available at: www.cdc.gov/mmwr/pdf/rr/rr4605.pdf). retardation). Indirect costs (lost productivity) were estimated to be $1 million per case. Preventing disease would avert Economic Impact and Cost Effectiveness these costs for the individual, families, health care providers, An economic cost and benefit analysis of routine menin- employers, health care payers and society. gococcal vaccination at 11 years of age showed that costs Table 4: Schedule for Antibiotic Prophylaxis of Meningococcal Disease Drug Age Group Dosage and Route of Administration Duration Ciprofloxacin Adults 500 mg po Single dose Ceftriaxone Children < 15 yrs Adults 125 mg IM 250 mg IM Single dose Single dose Rifampin Children < 1 mo Children > 1 mo Adults 5 mg/kg po q12h 10 mg/kg po q12h 600 mg po q12h 2 days 2 days 2 days Sources: CDC1, AAP60 14 CONCLUSION meningococcal disease is a serious illness that can Health care providers must also be aware of the variable progress rapidly, resulting in substantial morbidity and potentially fulminant clinical presentation of menin- and mortality, even with appropriate treatment. U.S. gococcal disease. The difficulty of a quick and accurate immunization policy shifted with the availability of diagnosis and the occurrence of substantial morbidity a quadrivalent conjugate meningococcal vaccine. and mortality even with appropriate and rapid treatment The conjugate vaccine is approved for use in persons are compelling reasons for a conjugate vaccine-based aged 11 to 55 years and recommended for routine approach to the prevention of meningococcal disease. vaccination of adolescents and college freshmen living in dormitories. Others at high risk and therefore recommended for vaccination include microbiologists routinely exposed to isolates of N. meningitidis, international travelers or U.S. citizens living in areas where N. meningitidis is endemic or hyperendemic, those with anatomic or functional asplenia or terminal complement 15 component disorders and military recruits. The constantly changing epidemiology, coupled with the ease and frequency of travel of U.S. citizens, suggests broad coverage against meningococcal serogroups is warranted. Although no vaccine against serogroup B is available currently, the quadrivalent meningococcal conjugate and polysaccharide vaccines both provide protection against the other four clinically relevant strains of N. meningitidis (A, C, Y, W-135). The conjugate vaccine is available for persons aged 11 to 55 years while the polysaccharide vaccine is approved for use in anyone aged 2 years or older and recommended for those aged 2 to 10 and 55 years and older. REFERENCES 1. Centers for Disease Control and Prevention. Prevention and control of meningococcal disease: Recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR 2005;54(RR-7):1-21. 2. Active Bacterial Core Surveillance (ABCs) 1997-2001 meningococcal surveillance reports. Available at: www.cdc.gov/ ncidod/dbmd/abcs/. Accessed July 15, 2004. 3. Centers for Disease Control and Prevention. Prevention and control of meningococcal disease and meningococcal disease and college students — recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR 2000; 49(RR-7):1-22. 4. Harrison LH, Pass MA, Mendelsohn AB, et al. Invasive meningococcal disease in adolescents and young adults. JAMA 2001; 286:694-699. 5. Apicella MA. Neisseria Meningitidis. In: Mandel GL, Bennett JE, Dolin R., eds, Principles and Practice of Infectious Diseases. 5th ed. Philadelphia, PA: Churchill Livingstone; 2000:2228-2241. 6. Rosenstein NE, Perkins BA, Stephens DS, et al. The changing epidemiology of meningococcal disease in the United States, 1992-1996. J Infect Dis 1999; 180:1984-1901. 7. Kirsch EA, Barton P, Kitchen L, Giroir BP. Pathophysiology, treatment, and outcome of meningococcemia: A review and recent experience. Pediatr Infect Dis J 1996; 15:967-979. 8. Edwards MS, Baker CJ. Complications and sequelae of meningococcal infections in children. J Pediatr 1981; 99:540-545. 9. Miller E, Salisbury D, Ramsay M. Planning, registration, and implementation of an immunisation campaign against meningococcal serogroup C disease in the UK: A success story. Vaccine 2002; 20(suppl 1):S58-S67. 10. Ramsay ME, Andrews NJ, Trotter CL, Kaczmarski EB, Miller E. Herd immunity from meningococcal serogroup C conjugate vaccine in England: Database analysis. BMJ 2003; 326:365-366. 11. Centers for Disease Control and Prevention. Control and prevention of meningococcal disease and control and prevention of serogroup C meningococcal disease: Evaluation and management of suspected outbreaks —recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR 1997; 46(RR-5):1-21. 12. Whitney CG, Farley MM, Hadler J, et al, for the Active Bacterial Core Surveillance of the Emerging Infections Program Network. Decline in invasive pneumococcal disease after the introduction of protein-polysaccharide conjugate vaccine. N Engl J Med 2003; 348:1737-1746. 13. Greenfield S, Sheehe PR, Feldman HA. Meningococcal carriage in a population of “normal” families. J Infect Dis 1971; 123:67-73. 14. Caugant DA, Hoiby EA, Magnus P, et al. Asymptomatic carriage of Neisseria meningitidis in a randomly sampled population. J Clin Microbiol 1994; 32:323-330. 15. Cartwright KA, Stuart JM, Jones DM, Noah ND. The Stonehouse survey: Nasopharyngeal carriage of meningococci and Neisseria lactamica. Epidemiol Infect 1987; 99:591-601. 16. Stephens DS. Uncloaking the meningococcus: Dynamics of carriage and disease. Lancet 1999; 353:941-942. 17. Aycock WL, Mueller JH. Meningococcus carrier rates and meningitis incidence. Bacteriol Rev 1950; 14:115-160. 18. Centers for Disease Control and Prevention. Notice to readers: Risk for meningococcal disease associated with the Hajj 2001. MMWR 2001;50(6):97-98. 19. Schwartz B, Moore PS, Broome CV. Global epidemiology of meningococcal disease. Clin Microbiol Rev 1989; 2(suppl):S118-S124. 20. Riedo FX, Plikaytis BD, Broome CV. Epidemiology and prevention of meningococcal disease. Pediatr Infect Dis J 1995; 14:643-657. 21. Rosenstein NE, Perkins BA, Stephens DS, Popovic T, Hughes JM. Meningococcal disease. N Engl J Med 2001; 344:1378-1388. 22. Parent du Chatelet I,Traore Y, Gessner BD, et al. Bacterial meningitis in Burkina Faso: surveillance using field-based polymerase chain reaction testing. Clin Infect Dis. 2005;40(1):17-25. 23. Bruce MG, Rosenstein NE, Capparella JM, et al. Risk factors for meningococcal disease in college students. JAMA 2001; 286:688-693. 24. Tunkel AR, Scheld WM. Pathogenesis and pathophysiology of bacterial meningitis. Clin Microbiol Rev 1993; 6:118-136. 25. Goldschneider I, Gotschlich EC, Artenstein MS. Human immunity to the meningococcus: I. The role of humoral antibodies. J Exp Med 1969; 129:1307-1326. 26. Goldschneider I, Gotschlich EC, Artenstein MS. Human immunity to the meningococcus: II. Development of natural immunity. J Exp Med 1969; 129:1327-1348. 27. Figueroa JE, Densen P. Infectious diseases associated with complement deficiencies. Clin Microbiol Rev 1991; 4:359-395. 28. Franke EL, Neu HC. Postsplenectomy infection. Surg Clin N Am 1981; 61:135-155. 29. Van Dueren M, Brandtzaeg P, van der Meer JW. Update on meningococcal disease with emphasis on pathogenesis and clinical management. Clin Microbiol Rev 2000; 13:144-156. 30. Cartwright KA, Jones DM, Smith AJ, Stuart JM, Kaczmarski ER, Plamer SR. Influenza A infection and meningococcal disease. Lancet 1991; 338:554-557. 31. Moore PS, Hierholzer J, DeWitt W, et al. Respiratory viruses and mycoplasma as cofactors for epidemic group A meningococcal meningitis. JAMA 1990; 264:1271-1275. 32. Hibberd ML, Sumiya M, Summerfield JA, Booy R, Levin M. Association of variant of the gene mannose-binding lectin with susceptibility to meningococcal disease. Lancet 1999; 353:1049-1053. 33. Nadel S, Newport MJ, Booy R, Levin M. Variation in the tumor necrosis factor-alpha gene promotor region may be associated with death from meningococcal disease. J Infect Dis 1996; 174:878-880. 16 34. Meningococcal Disease Surveillance Group. Analysis of endemic meningococcal disease by serogroup and evaluation of chemoprophylaxis. J Infect Dis 1976; 134:201-204. meningitis: Analysis of features of the disease according to the age of 255 patients. J Infect 1997; 34:227-235. 35. Brundage JF, Ryan MA, Feighner BH, Erdtmann FJ. Meningococcal 51. Tunkel AR, Scheld WM. Acute meningitis. In: Mandel GL, Bennett disease among United States military service members in relation to routine uses of vaccines with different serogroup-specific components, 1964-1998. Clin Infect Dis 2002;35(11):1376-1381. JE, Dolin R, eds, Principles and Practice of Infectious Diseases. 5th ed. Philadelphia, PA: Churchill Livingstone; 2000:959-997. 36. Jackson LA, Wenger JD. Laboratory-based surveillance for meningococcal disease in selected areas, United States, 1989-1991. MMWR 1993; 42(SS-2):21-30. 37. Fischer M, Hedberg K, Cardosi P, et al. Tobacco smoke as a risk factor for meningococcal disease. Pediatr Infect Dis J 1997; 16:979-983. 38. Imrey PB, Jackson LA, Ludwinski PH, et al. Meningococcal carriage, alcohol consumption, and campus bar patronage in a serogroup C meningococcal disease outbreak. J Clin Microbiol 1995; 33:3133-3137. 39. Imrey PB, Jackson LA, Ludwinski PH, et al. Outbreak of serogroup C meningococcal disease associated with campus bar patronage. Am J Epidemiol 1996; 143:624-630. 40. Cookson ST, Corrales JL, Lotero JO, et al. Disco fever: Epidemic meningococcal disease in Northeastern Argentina associated with disco patronage. J Infect Dis 1998; 178:266-269. 41. Centers for Disease Control and Prevention. Immunization of 17 50. Anderson J, Backer V, Voldsgaard P, et al. Acute meningococcal Adolescents — Recommendations of the Advisory Committee on Immunization Practices, the American Academy of Pediatrics, the American Academy of Family Physicians, and the American Medical Association. MMWR 1996;45(RR-13):1-17. 42. Soriano-Gabarró M, Stuart JM, Rosenstein NE. Vaccines for the prevention of meningococcal disease in children. Semin Pediatr Infect Dis 2002;13:182-189. 43. Tondella MLC, Popovic T, Rosenstein NE, et al. Distribution of Neisseria meningitidis serogroup B sero-subtypes and serotypes circulating in the United States. J Clin Microbiol 2000;38:3323-3328. 44. Sacchi CT, Whitney AM, Popovic T, et al. Diversity and prevalence of PorA types in Neisseria meningitidis serogroup B in the United States, 1992-1998. J Infect Dis 2000;182:1169-1176. 45. Centers for Disease Control and Prevention. Progress toward elimination of Haemophilus influenzae type b invasive disease among infants and children — United States, 1998-2000. MMWR 2002;51(11):234-237. 46. Trotter CL, Andrews NJ, Kaczmarski EB, Miller E, Ramsay ME. Effectiveness of meningococcal serogroup C conju-gate vaccine 4 years after introduction. Lancet 2004; 364:365-367. 47. Maiden MCJ, Stuart M, for the UK Meningococcal Carriage Group. Carriage of serogroup C meningococci 1 year after meningococcal C conjugate polysaccharide vaccine. Lancet 2002; 359:1829-1830. 48. Balmer P, Borrow R, Miller E. Impact of meningococcal serogroup C conjugate vaccine 4 years after introduction. Lancet 2004;364:717-722. 49. Roos KL, Tunkel AR, Scheld WM. Acute bacterial meningitis in children and adults. In: Scheld WM, Whitley RJ, Durack DT, eds. Infections of the Central Nervous System. 2nd ed. Philadelphia, PA: Lippincott-Raven;1997:335-401. 52. Saez-Llorens X, McCracken GH Jr. Bacterial meningitis in neonates and children. Infect Dis Clin North Am 1990; 4:623-644. 53. Gorse GJ, Thrupp LD, Nudleman KL, et al. Bacterial meningitis in the elderly. Arch Intern Med 1989; 149:1603-1606. 54. Racoosin JA, Whitney CG, Conover C, Diaz PS. Serogroup Y meningococcal disease in Chicago, 1991-1997. JAMA 1998; 280:2094-2098. 55. Griffiss JM, Yamasaki R, Eastbrook M, Kim JJ. Meningococcal molecular mimicry and the search for an ideal vaccine. Trans R Soc Trop Med Hyg 1991; 85 (suppl 1):S32-S36. 56. Broome CV. The carrier state: Neisseria meningitidis. J Antimicrob Chemother 1986;18 (suppl A):25-34. 57. Gaunt PN, Lambert SE. Single dose ciprofloxacin for the eradication of pharyngeal carriage of Neisseria meningitidis. J Antimicrob Chemother 1988; 21:489-496. 58. Dworzack DL, Sanders CC, Horowitz EA, et al. Evaluation of single-dose ciprofloxacin in the eradication of Neisseria meningitidis from nasopharyngeal carriers. Antimicrob Agents Chemother 1988; 32:1740-1741. 59. Schwartz B, Al-Tobaiqi A, Al-Ruwais A, et al. Comparative efficacy of ceftriaxone and rifampin in eradicating pharyngeal carriage of group A Neisseria meningitidis. Lancet 1988; 2:1239-1242. 60. American Academy of Pediatrics. Meningococcal infections. In: Pickering LK, ed. Red Book: 2003 Report of the Committee on Infectious Diseases. 26th ed. Elk Grove, IL: American Academy of Pediatrics; 2003. 61. Girgis N, Sultan Y, Frenck RW Jr, El-Gendy A, Farid Z, Mateczun A. Azithromycin compared with rifampin for eradication of nasopharyngeal colonization by Neisseria meningitidis. Pediatr Infect Dis J 1998;17:816-819. 62. Abramson JS, Spika JS. Persistence of Neisseria meningitidis in the upper respiratory tract after intravenous antibiotic therapy of systemic meningococcal disease. J Infect Dis 1985; 151:370-371. 63. Shepard CW, Ortega-Sanchez I, Corso P, Scott RD, Rosenstein N, ABCs team. Cost-effectiveness of conjugate meningococcal vaccination strategies in the United States. In: Abstracts of the 42nd Annual Meeting of the Infectious Diseases Society of America, Boston, Massachusetts, September 30-October 3, 2004: p.60. 64. Scott RD, Meltzer MI, Erickson LJ, De Wals P, Rosenstein N. Vaccinating first-year college students living in dormitories for meningococcal disease, an economic analysis. Am J Prev Med 2002;23:98-105. 65. Levine OS, Shaffer P, Haddix A, Perkins BA. Cost-effectiveness analysis for routine immunization with a quadrivalent meningococcal polysaccharide (A, C, Y, W-135) protein conjugate vaccine in the United States. Presented at the Tenth International Pathogenic Neisseria Conference, Baltimore, MD, September 1996. SELF-ASSESSMENT EXAMINATION Please circle the correct answer. (At least seven of the ten answers must be correct to obtain a CME certificate.) See mailing instructions on next page. 1. What percent of meningococcal disease cases in the U.S. are fatal? a) <4 b) 4 to 6 c) 6 to 10 d) 10 to 14 6. Which factors affect whether N. meningitidis crosses the mucosal barrier and gains access to the bloodstream, CNS and other organs? a) Bacterial virulence b) Host defense mechanisms c) Neither A nor B d) Both A and B 2. What percent of meningococcal disease survivors experience permanent sequelae (e.g., hearing loss, brain damage, renal failure or limb amputation)? 7. Which symptom is absent in neonates with meningococcal meningitis? a) 4 to 7 a) Change in affect or alertness level b) 8 to 10 b) Fever c) 11 to 19 c) Headache d) ≥20 d) Meningismus 3. What is the most common cause of bacterial meningitis in the U.S.? a) Haemophilus influenzae type b b) Neisseria meningitidis c) Staphylococcus aureus d) Streptococcus pneumoniae 8. Incidence of invasive Hib disease has fallen by what percent following widespread uptake of the conjugate Hib vaccine? a) 50 b) 70 c) 90 d) >99 4. Which serogroup, commonly responsible for U.S. epidemics a century ago, now rarely causes infection in this country? 9. Which benefit is not associated with use of the polysaccharide meningococcal vaccine? a) A a) Highly effective in older children and adults b) C b) Favorable safety profile c) Y c) Lifelong immunity d) W-135 d) Protection against serogroups A, C, Y and W-135 5. Which serogroup caused 2% of cases in the early 1990s, but nearly 40% by the end of the decade? 10. Conjugate vaccines are associated with which benefit(s) versus polysaccharide vaccines? a) A a) Herd effect b) C b) Improved duration of activity c) Y c) Induction of immunologic memory d) W-135 d) All of the above 18 CME EVALUATION Your input is extremely important and valuable to us. Please take the time to complete the following evaluation giving us your assessment of this CME activity. 1. This content meets the educational objectives 4. The format is clear, readable and useful a) agree b) neutral c) disagree a) agree b) neutral c) disagree 5. There was commercial bias in this activity a) yes b) no 2. Considering my experience, the material presented was ________________________________________________ a) satisfactory ________________________________________________ b) too elementary ________________________________________________ c) too technical ________________________________________________ 3. I gained information which will be useful to me 19 If yes, please give examples: a) agree Suggested topics for future issues or other comments about this publication: ________________________________________________ b) neutral ________________________________________________ c) disagree ________________________________________________ ________________________________________________ Instructions for obtaining CME credits To receive CME credits after reading the publication, complete the self-assessment examination, the CME evaluation, and your contact information. Return the examination and evaluation form, including your complete contact information, via fax to 301-907-0878 or by mail to: NFID Office of CME 4722 Bethesda Avenue, Suite 750 Bethesda, Maryland 20814 No fee is required. Please allow 4-6 weeks for processing your certification. Inquiries may be directed by phone to 301-656-0003 ext. 19 or by e-mail to info@nfid.org. Requests for credit must be received no later than November 2007. Name____________________________________________ Degree: ___________________________________________ Title: ____________________________________________ Organization: ______________________________________ Street Address: ____________________________________ E-mail Address: _____________________________________ City:_____________________________________________ State: _______________ Zip Code:_____________________ Signature: _______________________________________________________________ Date:_________________________ (Please print legibly or we will be unable to process your certificate.) National Foundation for Infectious Diseases 4733 Bethesda Avenue, Suite 750 Bethesda, Maryland 20814