Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Kawasaki disease wikipedia , lookup
Molecular mimicry wikipedia , lookup
Germ theory of disease wikipedia , lookup
Psychoneuroimmunology wikipedia , lookup
Immunosuppressive drug wikipedia , lookup
Pathophysiology of multiple sclerosis wikipedia , lookup
Behçet's disease wikipedia , lookup
Autoimmune encephalitis wikipedia , lookup
African trypanosomiasis wikipedia , lookup
Globalization and disease wikipedia , lookup
Management of multiple sclerosis wikipedia , lookup
Neuromyelitis optica wikipedia , lookup
Adoptive cell transfer wikipedia , lookup
Multiple sclerosis research wikipedia , lookup
X-linked severe combined immunodeficiency wikipedia , lookup
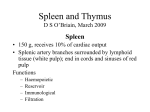
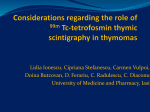
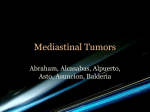
Case Report Graft-Versus-Host-Like Disease - A Case of Thymoma-Related Erythroderma Yu-Ta Yen Ji-Chen Ho Cheng-Yu Wang Graft-versus-host disease (GVHD) is a T-cell-mediated reaction that most commonly develops after transplantation of hematopoietic stem cells. In rare conditions, GVHD-like symptoms are observed in patients with thymoma. We present the case of a 58-year-old man with thymoma noted 6 years earlier who initially presented with myasthenia gravis and subsequently developed GVHD-like disease with symptoms of generalized itching, scaly erythroderma, and liver dysfunction. The histopathological features of a skin biopsy were consistent with those noted in the case of GVHD. We assume that the altered thymic microenvironment in thymoma patients causes immune dysregulation, leading to GVHD-like disease. (Dermatol Sinica 27: 241-247, 2009) Key words: Thymoma, Erythroderma, Myasthenia gravis, Graft-versus-host disease, GVHD INTRODUCTION Graft-versus-host disease (GVHD) occurs most commonly after immunocompetent hematopoietic stem cells are transplanted into an immunocompromised recipient. It also occurs through maternal-fetal transfer of lymphocytes; blood transfusion; and solid organ transplantation-particularly transplantation of a liver containing numerous immunocompetent lymphocytes. In most cases, GVHD first affects the skin, but hepatic and gastrointestinal manifestations aid in establishing the diagnosis. However, symptoms/ signs resembling those of GVHD may develop in some cases despite the lack of a history of transplantation or transfusion. The thymus plays an important role in immune maturation. In thymoma patients, the altered microenvironment of the thymus may induce immune dysregulation and autoreactivity. Several autoimmune disorders, including myasthenia gravis, pure red-cell aplasia, and acquired hypogammaglobulinemia are reported to be associated with thymoma. We report the case of a patient who had thymoma accompanied with myasthenia gravis for 6 years, but no history of blood transfusion or transplantation. The patient developed generalized erythroderma, liver dysfunction, and histopathological features of GVHD. From the Department of Dermatology, Chang Gung Memorial Hospital - Kaohsiung Medical Center, and Chang Gung University College of Medicine Corresponding author: Cheng-Yu Wang, Department of Dermatology, Chang Gung Memorial Hospital-Kaohsiung Medical Center, Ta-Pei Road 123, Niao-Sung Hsiang, 83301 Kaohsiung, Taiwan TEL: 886-7-7317123 ext. 2299 FAX: 886-7-7337612 E-mail: [email protected] Funding source: none Conflict of interest: none declared 241 Received: December 29, 2008 Revised: March 05, 2009 Accepted: March 12, 2009 Graft-Versus-Host-Like Disease A B C F D E Fig. 1 A 58 year-old male patient presented with generalized erythroderma. (A) Face showing papulosquamous lesions over eyelids and erosions over lips, but the scalp and mucosa were not involved. (B, C) Confluent erythematous scaly papulosquamous eruptions with pain and an itching sensation involving most of his trunk. (D, E) Severe scaly erythroderma involving lower limbs. (F) Closer view of left upper arm showing scaly papulosquamous eruptions. CASE REPORT A 58-year-old man visited our dermatology outpatient department, presenting with generalized erythroderma with scales and an itching sensation involving 90% of his body surface. Six years earlier, he had been diagnosed with thymoma accompanied with myasthenia gravis and had refused surgical intervention. The patient was lost to followup. Subsequently, he was prescribed prednisolone and pyridostigmine by another medical professional and had been receiving this treatment until he gradually began to develop generalized erythroderma 6 months ago. The patient had no history of atopy or treatment with any other drug. Skin examination Dermatol Sinica, Dec 2009 revealed a confluent erythematous and scaly papulosquamous eruption with pain and an itching sensation involving 90% of the body surface. The scalp and mucosa were not involved, but papulosquamous lesions over the eyelids and erosions over the lips were noted (Fig. 1). Skin biopsy was performed and the specimen was examined considering psoriasis, drug eruption, and mycosis fungoides. Pathological analysis of a section revealed parakeratosis; mild acanthosis; dyskeratosis of the epidermis; vacuolar degeneration and cleft formation at the dermoepidermal junction; perivascular lymphocytic infiltration into the superficial dermis; and periadnexal infiltration of lymphocytes, 242 Yu-Ta Yen, et al A B C D Fig. 2 Histopathology of a skin biopsy from left upper arm was consistent with GVHD. (A, B) Low-power magnification showing hyperkeratosis, parakeratosis in the stratum corneum; acanthosis with dyskeratotic cells in the epidermis; vacuolar degeneration and cleft formation at the dermoepidermal junction; solar elastosis and perivasular as well as periadnexal inflammatory infiltrate in superficial dermis. (H&E, original magnification x40, x100) (C) Prominent periadnexal infiltration of lymphocytes, histiocytes, and plasma cells. (H&E, original magnification x400) (D) High-power magnification showing parakeratosis, apoptotic keratinocytes in the epidermis, subepidermal cleft formation, and melanin incontinence at papillary dermis. (H&E, original magnification x400) histiocytes, and plasma cells. All these findings were consistent with those in the case of GVHD (Fig. 2). The patient was admitted for an additional systemic survey. Computed tomography (CT) of the chest and abdomen revealed a 4.75 cm lobular mass in the right anterior mediastinal region (Fig. 3), where a 1 cm nodule was noted 6 years earlier. A laboratory examination revealed the following values: white blood cell count, 10.6 x 10 3 cells/mm 3 (normal range, 3.910.6 x103 cells/mm3); hemoglobin, 16.4 g/dL (normal range, 13.5-17.5 g/dL); hematocrit, 48.3% (normal range, 41-53%); platelet count, 333 x 103 cells/mm3 (normal range, 150-400 x 10 3 cells/mm 3); eosinophil, 3% (normal range, 0-5%); IgE, 826 IU/ml (normal < 100 U/L); aspartate aminotransferase, 159 U/L (normal range, 0-37 U/L); alanine 243 aminotransferase, 310 U/L (normal, 0-40 U/L); alkaline phosphate, 96 U/L (normal range, 28-94 U/L ); albumin, 3.4 gm/dL (normal, 3.0-5.0gm/dL); acetylcholine receptor antibody, 67.1 nmol/mL (normal, <0.2); C-reactive protein, 9.59 mg/L (normal, <5 mg/L); and erythrocyte sedimentation rate, 7 mm/h (normal, 0-20 mm/h). On admission, the patient was administered prednisolone (up to 30 mg/d), pyridostigmine (60 mg t.i.d.), and topical applications containing keratolytic agents and corticosteroids. Although the scaly eruption showed an improvement, erythroderma persisted. Computed tomography revealed that the thymoma was large, and surgery was scheduled. Unfortunately, the thoracic surgeon postponed the surgery because of the patient’s skin conditions, and the patient was Dermatol Sinica, Dec 2009 Graft-Versus-Host-Like Disease A B Fig. 3 Images of computed tomography on chest showed an enlarged thymoma. (A) Coronal view showing a lobular contour mass over right anterior mediastinum. (B) Horizontal view showing the tumor measured 47.49 mm in the long axis, consistent with an enlarged thymoma. discharged. Two weeks later, the patient had an emergency condition of bleeding in the upper gastrointestinal region, and he expired despite intensive rescue procedures. DISCUSSION GVHD is a T-cell-mediated reaction that most commonly develops after transplantation of hematopoetic stem cells. Acute cutaneous GVHD develops in 20% to 80% of patients who undergo allogeneic bone marrow transplantation. In most cases, the skin is the first organ targeted, with faint erythematous macules developing initially. The macules then become confluent over a larger surface, and the condition may progress to erythroderma or bulla formation in the advanced stages. Involvement of the liver and the gastrointestinal system is also commonly noted. The presence of diarrhea and the detection of elevated bilirubin levels may serve as the diagnostic criteria; however, the possibility of GVHD should be considered even in the absence of such signs/symptoms.1 Previous reports have described thymoma-associated conditions with symptoms/ signs identical to GVHD, where the patients had no history of either transfusion or transplantation. Various terms such as graft-verDermatol Sinica, Dec 2009 sus-host-like disease complicating thymoma, thymoma-associated multiorgan autoimmunity, GVHD-like syndrome in malignant thymoma, and thymoma-associated graftversus-host-like reaction, have been coined for such conditions.2-5 The thymus is a primary lymphoid organ whose function is to “educate” thymocytes.6 In the course of migration from the bone marrow to the thymus, hematopoietic progenitor cells proliferate to generate a large population of immature thymocytes. In the thymic cortex, each of these cells develops distinct T-cell receptors through gene rearrangement. Thymocytes that can bind strongly to cell-surface molecules such as major histocompatibility complex/human leukocyte antigen (MHC/HLA), undergo positive selection, while the other cells that can only bind weakly to these receptors undergo apoptosis. The selected thymocytes then enter the thymic medulla where cells that exhibit an affinity for self-antigens undergo negative selection. This process for the development of central tolerance mainly depends on the autoimmune regulator gene (AIRE). It has been reported that 3 patients with thymoma presented with GVHD-like disease associated with the absence of AIRE expression.3 244 Yu-Ta Yen, et al Thymoma is a rare type of neoplasm that arises from the epithelial cells of the thymus. Approximately 40% of all thymoma patients develop a parathymic syndrome; of such syndromes, myasthenia gravis is the most common, followed by pure red-cell aplasia and acquired hypogammaglobulinemia. 7 A few cases of thymoma-associated skin eruption have been reported; the underlying conditions in these cases included pemphigus vulgaris, paraneoplastic pemphigus, dermatomyositis, and subcorneal pustular dermatosis. Wadhera et al. reviewed 7 cases of thymoma-associated GVHD-like disease2 and found that all the patients had diarrhea as a clinical symptom; however, this symptom was absent in the present case. Moreover, all the patients in the study by Wadhera et al.2 underwent surgical resection of the thymoma; however, surgery was not performed in the present case because of hesitation on the part of both, the patient and the surgeon. On the basis of the clinical features and histopathological findings of the present case, we considered several disease entities for differential diagnosis. Psoriasis was histopathologically ruled out owing to the absence of Munro and Kogoj microabscess, regular epidermal acanthosis, and dilated and tortuous capillaries in the papillary dermis. Further, we did not observe epidermotropism, large convoluted lymphocytes, or fibrotic expansion of the papillary dermis; therefore, cutaneous T-cell lymphoma was ruled out. In addition, epidermal spongiosis was absent, dyskeratotic keratinocytes were observed, and the patient showed a poor clinical response to prednisolone treatment; on these grounds, eczematous dermatitis was also ruled out as a differential diagnosis. The findings of hyperkeratosis and parakeratosis in the stratum corneum, acanthosis with dyskeratotic keratinocytes in the epidermis, vacuolar degeneration and cleft formation at the dermoepidermal junction, and solar elastosis 245 as well as perivasular and periadnexal mononuclear infiltrates in the superficial dermis were consistent with GVHD; but, they could also have been attributed to drug eruption or paraneoplastic pemphigus. However, drug eruption was ruled out because the patient did not have a history of treatment with drugs except prednisolone and pyridostigmine, which he had continually been receiving for 6 years for myasthenia gravis. Paraneoplastic pemphigus has been reported in association with Hodgkin’s lymphoma, thymoma, chronic lymphocytic leukemia, and Castleman’s disease. In all these cases, this condition is associated with painful oral ulcers and generalized, polymorphous eruption of blisters and lichenoid papules. Although we did not perform immunohistochemistry for diagnosis, we considered a diagnosis of paraneoplastic pemphigus to be less likely because the patient did not have painful oral ulcers or blisters. Transfusion and transplantationassociated GVHD may also be considered in the differential diagnosis of conditions with GVHD-like symptoms; however, since the patient had no history of transfusion and transplantation, this diagnosis was also ruled out. Although the elevated IgE levels of our patient were indicative of atopic dermatitis, this possibility was also ruled out owing to the absence of a previous atopic history and the discordance between the patient’s pathological features and those of atopic dermatitis. As in the case of our patient, elevated IgE levels have been previously noted in patients with acute GVHD after bone marrow trans8-9 plantation had been reported; this finding may further indicate a diagnosis of GVHDlike disease. Computed tomography revealed that the thymoma had enlarged from 1 cm (6 years earlier) to 4.75 cm at the time of the present study; hence, thymoma associated with GVHD-like disease was considered the appropriate diagnosis. We assume that the aberrant thymic microenvironment in the Dermatol Sinica, Dec 2009 Graft-Versus-Host-Like Disease case of thymoma patients may induce immune dysregulation and autoimmunity leading to GVHD-like disease. In summary, we report a case of thymoma, wherein the patient presented with erythroderma. Examination of a biopsy specimen revealed interface dermatitis, which is consistent with GVHD. Thus, when a patient clinically presents with erythroderma, myasthenia gravis, liver function impairment, and any other symptoms/signs, thymomaassociated GVHD-like disease should be included in the differential diagnosis, even if the patient does not have a history of transplantation or transfusion. REFERENCES 1. Sharp MT, Horn TD: Graft-versus-host disease. In: Wolff K, Goldsmith LA, Katz SI, et al., eds. Fitzpatrick’s Dermatology in General Medicine. 7th ed. New York: McGraw-Hill, 258-267, 2008. 2. Wadhera A, Maverakis E, Mitsiades N, et al.: Thymoma-associated multiorgan autoimmunity: Dermatol Sinica, Dec 2009 3. 4. 5. 6. 7. 8. 9. a graft-versus-host-like disease. J Am Acad Dermatol 57: 683-689, 2007. Offerhaus GJ, Schipper ME, Lazenby AJ, et al.: Graft-versus-host-like disease complicating thymoma: lack of AIRE expression as a cause of non-hereditary autoimmunity? Immunol Lett 114: 31-37, 2007. Holder J, North J, Bourke J, et al.: Thymomaassociated cutaneous graft-versus-host-like reaction. Clin Exp Dermatol 22: 287-290, 1997. Wang MH, Wong JM , Wang CY: Graft-versusHost disease-like syndrome in malignant thymoma. Scand J Gastroenterol 35: 667-670, 2000. Baldwin TA, Hogquist KA, Jameson SC: The fourth way? Harnessing aggressive tendencies in the thymus. J Immunol 173: 6515-6520, 2004. Rosenow EC, Hurley BT: Disorders of the thymus. A review. Arch Intern Med 144: 763-770, 1984. Saarinen U, Strandjord S, Warkentin P, et al.: Differentiation of presumed sepsis from acute graft-versus-host disease by C-reactive protein and serum total IgE in bone marrow transplant recipients. Transplantation 44: 540-546, 1987. Abedi MR, Backman L, Persson U, et al.: Serum IgE levels after bone marrow transplantation. Bone Marrow Transplant 4: 255-260, 1989. 246 Yu-Ta Yen, et al 移植物抗宿主病樣疾病 -胸腺瘤關連紅皮症的病例報告 顏育達 何宜承 高雄長庚紀念醫院皮膚科 王振宇 長庚大學醫學院 移植物抗宿主病為T細胞所引起之反應,最常發生於造血幹細胞移植後。在少數情形下,胸 腺瘤的病人被觀察到有類似移植物抗宿主病反應。我們描述一位58歲男性病人,在六年前被發現 胸腺瘤合併重症肌無力,在未接受器官移植或輸血情形下,後來發展成移植物抗宿主病樣疾病, 形成全身性癢而有鱗屑之紅皮症,併有肝功能異常。皮膚切片符合移植物抗宿主病之病理表現。 我們認為胸腺瘤微環境的改變造成免疫異常,進而造成移植物抗宿主病樣疾病。(中華皮誌:27: 241-247, 2009) 247 Dermatol Sinica, Dec 2009