Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Coronary artery disease wikipedia , lookup
Remote ischemic conditioning wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Heart failure wikipedia , lookup
Electrocardiography wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Myocardial infarction wikipedia , lookup
Heart arrhythmia wikipedia , lookup
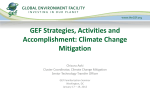
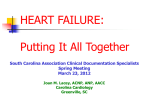
Journal of Cardiac Failure Vol. 17 No. 9 2011 Subgroup Analysis of a Randomized Controlled Trial Evaluating the Safety and Efficacy of Cardiac Contractility Modulation in Advanced Heart Failure WILLIAM T. ABRAHAM, MD,1 KOONLAWEE NADEMANEE, MD,2 KENT VOLOSIN, MD,3 STEVEN KRUEGER, MD,4 SURESH NEELAGARU, MD,5 NIRAV RAVAL, MD,6 OWEN OBEL, MD,7 STANISLAV WEINER, MD,8 MARC WISH, MD,9 PETER CARSON, MD,10 KENNETH ELLENBOGEN, MD,11 ROBERT BOURGE, MD,12 MICHAEL PARIDES, PhD,13 RICHARD P. CHIACCHIERINI, PhD,14 ROCHELLE GOLDSMITH, PhD,15 SIDNEY GOLDSTEIN, MD,16 YUVAL MIKA, PhD,17 DANIEL BURKHOFF, MD, PhD,15,17 AND ALAN KADISH, MD,18 ON BEHALF OF THE FIX-HF-5 INVESTIGATORS AND COORDINATORS* Columbus, Ohio; Inglewood, California; Philadelphia, Pennsylvania; Lincoln, Nebraska; Amarillo, Dallas, and Tyler, Texas; Atlanta, Georgia; Fairfax and Richmond, Virginia; Washington, DC; Birmingham, Alabama; New York and Orangeburg, New York; Detroit, Michigan; and Chicago Illinois ABSTRACT Background: Cardiac contractility modulation (CCM) signals are nonexcitatory electrical signals delivered during the absolute refractory period intended to improve contraction. We previously tested the safety and efficacy of CCM in 428 NYHA functional class III/IV heart failure patients with EF #35% and narrow QRS randomized to optimal medical treatment (OMT) plus CCM (n 5 215) versus OMTalone (n 5 213) and found no significant effect on ventilatory anaerobic threshold (VAT), the study’s primary end point. In the present analysis, we sought to identify if there was a subgroup of patients who showed a response to CCM. Methods and Results: The protocol specified that multiregression analysis would be used to determine if baseline EF, NYHA functional class, pVO2, or etiology of heart failure influenced the impact of CCM on AT. Etiology and baseline pVO2 did not affect efficacy. However, baseline NYHA functional class III and EF $25% were significant predictors of increased efficacy. In this subgroup (comprising 97 OMT and 109 CCM patients, w48% of the entire population) VAT increased by 0.10 6 2.36 in CCM versus 0.54 6 1.83 mL kg1 min1 in OMT (P 5 .03) and pVO2 increased by 0.34 6 3.11 in CCM versus 0.97 6 2.31 (P 5 .001) at 24 weeks compared with baseline; 44% of CCM versus 23% of OMT subjects showed improvement of $1 class in NYHA functional class (P 5 .002), and 59% of CCM versus 42% of OMT subjects showed a $10-point reduction in Minnesota Living with Heart Failure Questionnaire (P 5 .01). All of these findings were similar to those seen at 50 weeks. Conclusions: The results of this retrospective hypothesis-generating analysis indicate that CCM significantly improves objective parameters of exercise tolerance in a subgroup of patients characterized by normal QRS duration, NYHA functional class III symptoms, and EF O25%. (J Cardiac Fail 2011;17:710e717) Key Words: Cardiac contractility modulation, cardiopulmonary stress testing, peak VO2, ventilatory anaerobic threshold, Minnesota Living With Heart Failure Questionnaire, New York Heart Failure Classification six minute hall walk test. From the 1Ohio State University Heart Center, Columbus, Ohio; 2Pacific Rim EP, Inglewood, California; 3University of Pennsylvania, Philadelphia, Pennsylvania; 4Bryan LGH, Lincoln, Nebraska; 5Lone Star Arrhythmia, Amarillo, Texas; 6St. Joseph’s Research Institute, Atlanta, Georgia; 7University of Texas Southwestern, Dallas, Texas; 8Tyler Cardiovascular Consultants, Tyler, Texas; 9Inova Arrhythmia Associates, Fairfax, Virginia; 10 Washington Veterans Administration Hospital, Washington, DC; 11 Virginia Commonwealth University School of Medicine, Richmond, Virginia; 12 University of Alabama, Birmingham, Alabama; 13Mount Sinai, New York, New York; 14R. P. Chiacchierini & Associates, New York, New York; 15Columbia University, New York, New York; 16Henry Ford Hospital, Detroit, Michigan; 17Impulse Dynamics, Orangeburg, New York and 18 Northwestern University, Chicago, Illinois. Manuscript received January 24, 2011; revised manuscript received April 12, 2011; revised manuscript accepted May 9, 2011. Reprint requests: William T. Abraham, MD, Ohio State University, 473 West 12th Avenue, Room 110P, Columbus, Ohio, 43210-1252. Tel: 614-292-9560; Fax: 614-292-9761. E-mail: [email protected] Funding: Impulse Dynamics. See page 716 for disclosure information. * FIX-HF-5 Investigators and Coordinators are listed in Appendix 1. 1071-9164/$ - see front matter Ó 2011 Elsevier Inc. All rights reserved. doi:10.1016/j.cardfail.2011.05.006 710 CCM in NYHA III Patients With EF $ 25% Cardiac contractility modulation (CCM) is an electrical deviceebased approach developed for the treatment of chronic heart failure (CHF).1,2 CCM signals are nonexcitatory electric signals applied during the myocardial absolute refractory period that enhance the strength of cardiac muscular contraction.3 CCM signal application is associated with normalization of phosphorylation of key proteins and improved expression of genes coding for proteins involved in regulation of calcium cycling and contraction.1,4,5 In a prior double-blind double-crossover study of 164 subjects with ejection fraction (EF) !35% (the FIX-HF-4 study), 3 months of CCM treatment improved exercise tolerance as judged by peak VO2 and improved quality of life.6 More recently, a randomized unblinded study involving 428 subjects randomized to either continued optimal medical therapy (OMT) or OMT in addition to CCM (the FIX-HF-5 study) was performed.7,8 Although that study’s primary safety end point was met (a noninferiority analysis between groups of the composite of all-cause mortality and allcause hospitalization), the primary efficacy end point (a superiority analysis of the impact of treatment on ventilatory anaerobic threshold [VAT]) was not met. The FIX-HF-5 protocol prespecified a plan for analyzing effects in specific patient subgroups.9 The purpose of the present analysis was to determine, based on this prespecified plan and the predefined primary end point (VAT), whether a subgroup of patients enrolled in the FIX-HF-5 study exhibited a beneficial effect of CCM. Such a subgroup, composed of about one-half of the entire cohort, was indeed identified. These findings have led to the Abraham et al 711 initiation of a prospective confirmatory study that will be conducted in this subgroup of patients. Methods The FIX-HF-5 study was a prospective, randomized, parallelgroup, controlled trial of OMT versus OMT plus CCM. The details of the protocol, device implantation procedure, primary and secondary end points, and statistical analysis plan have been detailed previously.7 In brief, the study included subjects $18 years old with EF #35%, with NYHA functional class III or IV symptoms despite medical treatment with diuretics, angiotensinconverting enzyme inhibitor and/or angiotensin receptor blocker and b-blockers for $3 months with a baseline peak VO2 on cardiopulmonary stress testing (CPX) $9 mL O2 kg1 min1 who were in normal sinus rhythm and not indicated for a cardiac resynchronization therapy (CRT) device (ie, QRS duration !130 ms). Unless there were extenuating circumstances, subjects were required to have an implantable cardioverter/defibrillator. Subjects were excluded if they were hospitalized within 30 days of enrollment, were inotropic dependent, had O8,900 premature ventricular contractions per 24 hours on a baseline Holter monitor, had permanent atrial fibrillation, or had a myocardial infarction within 90 days, percutaneous coronary intervention within 30 days, or coronary artery bypass surgery within 90 days of enrollment. After informed consent, all subjects underwent baseline evaluation which included a CPX test, Minnesota Living with Heart Failure Questionnaire (MLWHFQ), 6-minute hall walk test (6MWT), NYHA functional class determination by a clinician not otherwise involved in the care of the patient (blinded to therapy assessment), an echocardiogram, and a 24-hour Holter monitor. After meeting inclusion criteria, a device implantation date Randomized n=428 Death Prior to SSD n=2 EF≥25 and NYHA III n=206 WD Prior to SSD n=3 Control n=97 Treatment n=109 Not Implanted n=1 5 W/D 1 Death 12Wk n=91 12Wk n=1 Successful Implant n=101 2 Deaths 12Wk n=99 2 W/D Failed Implant n=2 12Wk n=2 1 Death 24Wk n=89 24Wk n=1 2 W/D 1 Death 24Wk n=98 24Wk n=2 1 Death 50Wk n=86 50Wk n=1 50Wk n=97 50Wk n=2 Fig. 1. CONSORT diagram showing flow of patients during the study for the subgroup characterized by baseline EF $ 25% and NYHA III. 712 Journal of Cardiac Failure Vol. 17 No. 9 September 2011 Table 1. Baseline Characteristics Variable Age (y) Male White CHF ischemic etiology Prior MI Prior CABG Prior PCI Diabetes NYHA (site) functional class III QRS Duration (ms)y Holter (PVCs/24h) LVEF (%) (site) LVEDD (mm) (site)z MLWHFQ 6MWT (m)x CPX (site){ Peak VO2 (mL kg1 min1) VAT (mL kg1 min1) RER Exercise Time (min) Physical exam Weight (kg) Height (cm) BMI (kg/m2) Resting HR (beats/min) Mean blood pressure Control, Mean (SD) or n/N (%) (n 5 97) 60.3 76/97 72/97 71/97 61/97 48/97 35/97 49/97 97/97 101.7 947.6 28.9 60.1 53.9 333.6 (12.1) (78.4) (74.2) (73.2) (62.9) (49.5) (36.1) (50.5) (100.0) (13.5) (1518.2) (4.5) (6.7) (23.6) (87.8) Optimizer, Mean (SD) or n/N (%) (n 5 109) 58.7 77/109 83/109 79/109 73/109 47/109 48/109 53/109 109/109 99.6 1143.9 28.9 59.7 59.8 330.6 (12.0) (70.6) (76.2) (72.5) (67.0) (43.1) (44.0) (48.6) (100.0) (14.3) (1840.1) (5.1) (8.0) (23.0) (79.1) P Value .2872* .2637* .8717* 1.0000* .5610* .4019* .2583* .8890* 1.000 .1576* .8205* .7608* .9323* .0719* .6698* 15.0 11.2 1.11 11.7 (2.7) (2.2) (0.09) (3.4) 14.6 10.6 1.14 11.4 (2.9) (2.1) (0.09) (3.10) .2494* .0521* .0174* .3666* 96.8 174.2 31.9 72.1 86.2 (23.4) (9.7) (7.4) (11.6) (12.32) 92.4 173.3 30.7 70.9 86.3 (22.6) (9.4) (7.1) (11.9) (11.9) .1057* .3855* .1411* .3994* .7754* CHF, chronic heart failure; MI, myocardial infarction; CABG, coronary artery bypass graft; PCI, percutaneous coronary intervention; NYHA, New York Heart Association; PVC, premature ventricular contraction; LVEF, left ventricular ejection fraction; LVEDD, left ventricular end-diastolic diameter; MLWHFQ, Minnesota Living with Heart Failure Questionnaire; 6MWT, 6-minute walk test; CPX, cardiopulmonary stress testing; VO2, maximal oxygen consumption, VAT, ventilatory anaerobic threshold; RER, respiratory exchange ratio; BMI, body mass index; HR, heart rate. *Two-sided Wilcoxon rank sum test. y One control patient did not report a QRS duration. z One control patient did not report LVEDD. x One control patient did not have a 6-minute walk test at baseline. { One control patient did not have any variable reported for the site CPX. was scheduled. This scheduled implantation date served as the study start date (SSD) for all subjects. Subjects were then randomized (1:1) to either the OMT group or to the CCM group. Subjects randomized to the CCM group underwent Optimizer device implantation on the SSD. The implantation procedure and electrical characteristics of CCM signals have been detailed previously.7 To eliminate bias and optimize consistency of results, all CPX tests were assessed in a central core laboratory (Appendix 2). VAT values were determined with the V-slope method9 by 2 independent readers blinded to treatment group. Data Analysis Plan The data analysis plan has been detailed previously.7 In brief, the primary effectiveness end point was the change from baseline in the VAT measured on CPX testing. This end point was required by the U.S. Food and Drug Administration because of the unblinded nature of this study and the concern that all other functional end points are subject to placebo effect. The primary analysis was based on a comparison of ‘‘responder’’ rates10 between the CCM and OMT groups at the 24-week follow-up visit, with an individual subject defined as a responder if VAT increased by $20% at 24 weeks (Fisher exact test). The primary analysis was based on the intention-to-treat population; imputation was used to account for missing data as detailed previously.7 Secondary efficacy end points were peak VO2 and quality of life assessed by MLWHFQ, each also assessed by a responder analysis with a 20% increase in peak VO2 and a 10-point reduction in MLWHFQ used to define responders. Additional end points included changes in NYHA functional class (with a change of 1 class considered to be a response) and 6MWT (with a 40-m increase considered to be a response).These comparisons were made using 1-sided Student t tests. Baseline characteristics were compared with appropriate tests as specified in the text. P values of #.025 for 1-sided tests and #.05 for 2-sided tests were considered to be statistically significant. To explore the relationships between baseline covariates and treatment efficacy (assessed by the difference in VAT at 24 weeks), a mixed-modeling procedure was used to assess the covariates and their interactions with treatment. Eligible covariates in the initial model included baseline values for NYHA functional class, peak VO2, EF (!25%, $25%), left ventricular end-diastolic diameter (!61 mm, $61 mm), all 2-way interactions with treatment, and the 3-way interaction of NYHA functional class, EF, and treatment. By backward elimination, terms were removed from the model until all remaining terms in the model had a P value of #.10. The primary safety end point was the composite event rate of all-cause mortality and all-cause hospitalization through 50 weeks. An independent Events Adjudication Committee (EAC) and Data and Safety Monitoring Board (DSMB; Appendix 3) were used to adjudicate safety end points and monitor composite safety during the study conduct. CCM in NYHA III Patients With EF $ 25% Table 2. Baseline Medications, n (%) Medication Angiotensin-converting enzyme inhibitor (ACEi) Angiotensin receptor blocker (ARB) ACEi or ARB Beta-blocker Loop diuretic Second diuretic Aldosterone inhibitor Hydralazine Digoxin Nitrates Calcium channel blocker Antiarrhythmic Control (n 5 97) Optimizer (n 5 109) 68 (70.1) 82 (75.2) 24 90 92 84 6 42 5 41 32 4 13 (24.7) (92.8) (94.9) (86.6) (6.2) (43.3) (5.2) (42.0) (33.0) (4.1) (13.4) 25 100 105 98 8 50 5 37 39 12 18 (22.9) (91.7) (96.3) (89.9) (7.3) (45.9) (4.6) (34.0) (35.8) (11.0) (16.5) No significant difference between control and optimizer groups for any medication by 2-sided Fisher exact test. Results Abraham et al 713 those with EF !25%. Further investigation revealed that within this subgroup, the patients with baseline NYHA functional class IV symptoms had high variability in response, and if the subgroup was further limited to patients with NYHA 3 symptoms, there was a statistically significant impact of CCM on VAT (P 5 .031). Therefore, we tested the effect in patients falling within the cross-section of these 2 criteria. From the overall population of 428 patients, this included 97 OMT and 109 CCM patients (48% of the overall population). The remainder of this report will summarize the effects of CCM in this population. The overall flow of patients falling within the defined subgroup is summarized in Figure 1. As summarized in Table 1, all baseline characteristics were balanced between the CCM and OMT groups except for the respiratory equivalent ratio (RER), which was slightly higher in the CCM group. Baseline medications (Table 2) were similar in the 2 groups. Identification of Subgroup With Best Response to CCM Efficacy Results The baseline characteristics and efficacy results in the overall cohort have been described in detail previously.9 The results of the mixed-modeling procedure used to assess the covariates and their interactions with treatment showed that the final model included baseline peak VO2, EF, and the interaction of EF and treatment. The interaction indicated that treated patients with EF $25% had a better response that There were statistically and clinically significantly greater improvements in VAT (0.64 mL kg1 min1; P 5 .03 for the completed cases; P 5 .024 for the ITT population with imputed missing data), peak VO2 (1.31 mL kg1 min1; P 5 .001), MLWHFQ (10.8 points; P 5 .003) and NYHA functional class (0.29; P 5 .001) in the CCM group compared to the control group at 24 weeks (Fig. 2). Responder 1.5 0.75 p=0.001 Difference VAT (ml/kg/min) CCM -0.5 0.25 0.00 -0.50 -1.5 -0.75 OMT CCM Difference -5 -10 p=0.0003 -20 CCM Difference 50 (% -15 OMT -0.25 -1.0 0 MLWHFQ OMT NYHA Patients with >= 1 Point Reduction ) Peak VO2 (ml/kg/min) 0.5 0.0 p=0.03 0.50 1.0 40 30 p=0.0023 20 10 0 OMT CCM Difference Six Minute Walk (m) 30 p=0.044 20 10 0 OMT CCM Difference Fig. 2. Efficacy results at 24 weeks of follow-up in the completed cases population in the subgroup of patients with baseline EF $25% and NYHA functional class III symptoms. OMT, optimal medical therapy; CCM, group receiving cardiac contractility modulation signals. 714 Journal of Cardiac Failure Vol. 17 No. 9 September 2011 Table 3. Results of responders analyses for primary and secondary study end points at 24 Week follow up in the subgroup of subjects with baseline EF $ 35% and NYHA Class III symptoms Parameter OMT n/N (%)* VAT VAT (ITT) Peak VO2 MLWHFQ NYHA functional class 6MWT 4/69 9/97 3/76 35/84 19/82 20/79 (5.8%) (9.4%) (3.95%) (41.7%) (23.2%) (25.3) CCM n/N (%)* 17/83 23/109 18/94 60/101 43/97 36/97 CCM-OMT P Valuey 14.7% 12.1% 15.2% 17.7% 21.1% 11.8% .0073 .026 .002 .0119 .0023 .065 (20.5%) (21.5%) (19.15%) (59.4%) (44.3%) (37.1%) ITT, intention-to-treat population based on imputation of missing data; other abbreviations as in Table 1. All data are based on completed cases population except for VAT, for which both completed cases and intent-to-treat populations are included. *n denotes number of patients meeting success criteria, N the total number of patients in the group for which paired baseline and 24-week data exist, and % the percentage of patients meeting success criteria. y P values by one-sided Fisher’s exact test. 60 (seconds) 0 -20 -40 -60 0.050 0.025 Prior studies provided evidence of safety and efficacy of 3 months’ CCM treatment in subjects with medically refractory NYHA functional class III and IV heart failure with EF #35% and normal QRS duration.11,12 The overall results of the more recent FIX-HF-5 study showed CCM to be safe, and although mean peak VO2 was increased, there was no increase in the primary efficacy end point, VAT measured during cardiopulmonary stress testing.9 In the present prespecified analysis of the FIX-HF-5 data, CCM was shown to be particularly effective in the less sick half Δ RER 0.000 -0.025 Δ Peak VO2 (ml/kg/min) -0.050 1.0 * 0.5 * 0.0 -0.5 -1.0 -1.5 0.75 Δ VAT (ml/kg/min) Discussion * 20 Safety in the Subgroup Regarding the primary safety end point, there were 42 events in the 97 OMT subjects (43.3%) compared with 52 events in the 109 CCM subjects (47.7%, Blackwelder test: P 5 .12). From among these subjects, there were 2 deaths in the OMT group (0.9%) and 4 deaths in the CCM group from SSD to 1 year (2.0%; P 5 .69, Fisher exact test). Serious adverse events, summarized in Table 4, were reasonably balanced between groups, with trends toward reduced rates of heart failureerelated events in the CCM group. Overall, there was no statistically significant difference in the overall rate of events (P 5 .3285 by 2-sided Fisher exact test). Devicerelated serious adverse events were very infrequent in this group (Table 5), with the 2 most-common events being lead dislodgments and 2 instances of Optimizer System replacements for a device malfunction that was corrected. * 40 Δ Exercise Duration rates were also significantly better in the CCM group (Table 3). Despite the relatively small number of subjects, these improvements were evident in both the responder analyses and the comparison of mean changes from baseline in most comparisons. These results were also maintained through 50 weeks, as shown in Figure 3, which further details several exercise parameters. Exercise duration increased over time in the CCM group and declined in the OMT group, although RER was similar between groups and did not differ from baseline. VAT increased over time and peak VO2 plateaued at 24 weeks in the CCM group, whereas both declined in the OMT group. 0.50 * 0.25 * 0.00 -0.25 -0.50 -0.75 -1.00 12 24 50 Follow Up (W eeks) Fig. 3. Exercise parameters over time in the subgroup of patients with baseline EF $25% and NYHA functional class III symptoms. Circles, CCM group; squares, OMT group.* P ! 0.05. CCM in NYHA III Patients With EF $ 25% Abraham et al 715 Table 4. Serious Adverse Events Events (Patients) Category General cardiopulmonary event Arrhythmias Worsening heart failure ICD/pacemaker system related Bleeding Localized infections* Sepsis Neurologic dysfunction General medical Total OMT (n 5 97) Events/Patient-Year CCM (n 5 109) 23 (19) 10 (8) 27 (16) 3 (3) 6 (6) 20 (15) 0 8 (7) 33 (26) 130 (46) 30 11 18 5 2 15 2 2 50 135 (21) (8) (14) (4) (2) (14) (2) (2) (34) (60) OMT (p-y 5 86.4) CCM (p-y 5 100.9) 0.266 0.116 0.313 0.035 0.069 0.231 0.000 0.093 0.382 1.505 0.297 0.109 0.178 0.050 0.020 0.149 0.020 0.020 0.496 1.338 *Localized infections were all nonseptic infections with a documented location, e.g., upper respiratory bronchitis, pneumonia, ottitis media, urinary tract infection, gastrointestinal, cellulitis, etc. of overall patient population, ie, in patients characterized by baseline EF $25% and NYHA functional class III symptoms (comprising 48% of the overall population). A study has therefore been initiated to prospectively test CCM in this subgroup of patients. There are several key findings of the present analysis related to exercise tolerance. Both peak VO2 and VAT were improved by clinically and statistically significant amounts. These findings were identified independent of whether the analysis was a comparison of mean changes or a responder analysis in which a 20% improvement in each parameter was used to define a ‘‘responder.’’ There is significant evidence that these findings are not due to a placebo effect. First, VAT is not known to be subject to placebo effect, because neither patient nor test administrator has knowledge of VAT during the test and the value was assigned in a blinded core lab after the test. Second, the RER values did not vary significantly between time points and between groups. Finally, regarding these parameters, the improvements in the CCM relative to the control group persists through the 50-week time point. The magnitude of improvements in peak VO2 is greater than observed in prior studies of other treatments for heart failure such as CRT, albeit in a different group of patients (ie, with prolonged Table 5. Device-Related Serious Adverse Events Optimizer Systemerelated overall Optimizer lead fracture Optimizer RV lead dislodgement IPG problem/change Optimizer RA lead dislodgement Optimizer pocket dehiscence/erosion Dehiscence/erosion Optimizer pocket infection Optimizer pocket stimulation Lead perforation Optimizer pocket bleeding Sensation due to CCM Extracardiac stimulation Events (Patients) Events/ Patient-Year 10 (9) 1 4 (4) 2 (1) 1 0 0.099 0.010 0.040 0.020 0.010 0.000 0 0 1 1 0 0 0.000 0.000 0.010 0.010 0.000 0.000 RV, right ventricular; IPG, implantable pulse generator; RA, right atrial; CCM, cardiac contractility modulation. QRS duration). Other efficacy parameters (MLWHFQ and NYHA functional class) also showed strong positive effects of CCM, but these are more prone to placebo effect. It is further noteworthy that despite what are considered rather large improvements in peak VO2 (at least regarding what is observed with CRT) and, by inference, large improvements in VAT, the rate of response indicated by the formal responders analysis was only w20%. As pointed out previously,7,10 it should be noted that the use of responder analysis has not been used previously in the context of continuous variables such as peak VO2 and VAT. As noted, and as is self-evident, the rate of response is highly dependent on the criterion for defining success. In our case, we chose a rather high threshold (20% increase from baseline) largely to overcome inherent uncertainties in quantifying VAT.8 In a prior evaluation, we showed that if the same type of analysis had been applied to data available from studies of CRT, similar rates of response would also have been identified.10 Mortality and severe adverse events were reasonably well balanced between treatment and control groups in the target subgroup. One point to note was the reduced rate of adverse events attributed to heart failure exacerbations in the CCM group. The mechanisms of CCM have been studied in several earlier animal and clinical studies,4,13 in which CCM has been shown to normalize gene expression, protein expression, and protein phosphorylation in failing myocardium. These effects are evident within hours of initiating signal delivery in the region where CCM signals are delivered. Improvements in the remote areas are evident sometime within 3 months of treatment. Such effects can be speculated to improve the ability of the myocardial cells to cycle calcium (during both systole and diastole) and to improve myofilament efficacy, among other things, thus leading to improved contractile reserve during stress. There are several possible reasons why CCM would be more effective in the patients with EF $25% and NYHA functional class III symptoms. First, it may be that there are limits to the degree of myocardial dysfunction that can be overcome by CCM delivered to 2 electrodes in the right 716 Journal of Cardiac Failure Vol. 17 No. 9 September 2011 ventricular (RV) septum, so that patients with very low EFs may exhibit less of an effect. Second, patients with lower EFs have significantly larger hearts and it may be that CCM delivered with 2 electrodes only to the RV septum does not reach a large enough proportion of the entire heart. Finally, the number of patients enrolled with NYHA functional class IV was very small, only 33 patients. Therefore, it would not be possible to make any conclusions about this class of patients. Interestingly, Cleland et al14 pointed out that there have been earlier studies in which less sick patients showed greater responses to device-based therapies. Those authors note that in SCD-HeFT, patients in NYHA functional class II benefited but those in NYHA functional class III did not15; that in the CORONA study, patients in the lowest tercile of N-terminal proeB-type natriuretic peptide who had the best prognosis also benefited most from intervention; and that the REVERSE14 and CARE-HF16 studies suggest that benefits of CRT are at least as great in NYHA functional class I/II as in class III/IV.17 The limitations of subgroup analyses are well known, and therefore the present findings should be viewed as hypothesis generating. A new study, designed to prospectively test the effectiveness of CCM in the target population, has recently been initiated. In the overall FIX-HF-5 study cohort, CCM improved peak VO2 by 0.65 mL kg1 min1, similar to what is typically observed with CRT in the wide-QRS cohort. However, because peak VO2 would not be accepted by the U.S. Food and Drug Administration as the primary efficacy end point in this unblinded trial, the study could not be considered to provide sufficient evidence of efficacy. The results of the present study suggest that in a subgroup of the overall heart failure population with narrow QRS duration, CCM significantly improved VAT, the prospectively defined primary end point. In this subgroup, CCM appears to be particularly promising. This is being pursued in a prospective study. Disclosures Yuval Mika is an employee and shareholder of Impulse Dynamics. Daniel Burkhoff, Alan Kadish, and William T. Abraham are consultants to Impulse Dynamics. All other authors report no potential conflicts of interest. References 1. Burkhoff D, Ben Haim SA. Nonexcitatory electrical signals for enhancing ventricular contractility: rationale and initial investigations of an experimental treatment for heart failure. Am J Physiol Heart Circ Physiol 2005;288:H2550e6. 2. Lawo T, Borggrefe M, Butter C, et al. Electrical signals applied during the absolute refractory period: an investigational treatment for advanced heart failure in patients with normal QRS duration. J Am Coll Cardiol 2005;46:2229e36. 3. Brunckhorst CB, Shemer I, Mika Y, ben Haim SA, Burkhoff D. Cardiac contractility modulation by nonexcitatory currents: studies in isolated cardiac muscle. Eur J Heart Fail 2006;8:7e15. 4. Imai M, Rastogi S, Gupta RC, et al. Therapy with cardiac contractility modulation electrical signals improves left ventricular function and remodeling in dogs with chronic heart failure. J Am Coll Cardiol 2007;49:2120e8. 5. Butter C, Rastogi S, Minden HH, Meyhofer J, Burkhoff D, Sabbah HN. Cardiac contractility modulation electrical signals improve myocardial gene expression in patients with heart failure. J Am Col Cardiol 2008;51:1784e9. 6. Borggrefe MM, Lawo T, Butter C, et al. Randomized, double blind study of nonexcitatory, cardiac contractility modulation electrical impulses for symptomatic heart failure. Eur Heart J 2008;8:1019e28. 7. Abraham WT, Burkhoff D, Nademanee K, et al. A randomized controlled trial to evaluate the safety and efficacy of cardiac contractility modulation in patients with systolic heart failure: rationale, design, and baseline patient characteristics. Am Heart J 2008;156:641e8. 8. Kadish A, Nademanee K, Volosin K, et al. A randomized controlled trial evaluating the safety and efficacy of cardiac contractility modulation in advanced heart failure. Am Heart J 2011;161:329e37. 9. Sue DY, Wasserman K, Moricca RB, Casaburi R. Metabolic acidosis during exercise in patients with chronic obstructive pulmonary disease. Use of the V-slope method for anaerobic threshold determination. Chest 1988;94:931e8. 10. Burkhoff D, Parides M, Borggrefe M, Abraham WT, Kadish A. ‘‘Responder analysis’’ for assessing effectiveness of heart failure therapies based on measures of exercise tolerance. J Card Fail 2009; 15:108e15. 11. Neelagaru SB, Sanchez JE, Lau SK, et al. Nonexcitatory, cardiac contractility modulation electrical impulses: feasibility study for advanced heart failure in patients with normal QRS duration. Heart Rhythm 2006;3:1140e7. 12. Borggrefe MM, Lawo T, Butter C, et al. Randomized, double blind study of nonexcitatory, cardiac contractility modulation electrical impulses for symptomatic heart failure. Eur Heart J 2008;29:1019e28. 13. Butter C, Rastogi S, Minden HH, Meyhofer J, Burkhoff D, Sabbah HN. Cardiac contractility modulation electrical signals improve myocardial gene expression in patients with heart failure. J Am Coll Cardiol 2008;51:1784e9. 14. Cleland JG, Coletta AP, Clark AL, Cullington D. Clinical trials update from the American College of Cardiology 2009: ADMIRE-HF, PRIMA, STICH, REVERSE, IRIS, partial ventricular support, FIX-HF-5, vagal stimulation, REVIVAL-3, pre-RELAX-AHF, ACTIVE-A, HF-ACTION, JUPITER, AURORA, and OMEGA. Eur J Heart Fail 2009;11:622e30. 15. Bardy GH, Lee KL, Mark DB, et al. Amiodarone or an implantable cardioverter-defibrillator for congestive heart failure. N Engl J Med 2005;352:225e37. 16. Cleland JG, Daubert JC, Erdmann E, et al. Longer-term effects of cardiac resynchronization therapy on mortality in heart failure [the Cardiac ResynchronizationeHeart Failure (CARE-HF) trial extension phase]. Eur Heart J 2006;27:1928e32. 17. Cleland JG, Freemantle N, Daubert JC, Toff WD, Leisch F, Tavazzi L. Long-term effect of cardiac resynchronisation in patients reporting mild symptoms of heart failure: a report from the CARE-HF study. Heart 2008;94:278e83. Appendix 1 Arizona Arrhythmia Research Center, Scottsdale, Arizona: Thomas Mattioni, MD, Vijay Swarup, MD, Sara Scrivano, Claudia Williams, RN; Arrhythmia Center for Southern Wisconsin/St. Luke’s Medical Center, Milwaukee, Wisconsin: Imran Niazi, MD, Nguyen Phan, MD, Rebecca Dahme, RN, Jo Ann Kiemen; Aurora Denver Cardiology Associates, CCM in NYHA III Patients With EF $ 25% Aurora, Colorado: Andrew I. Cohen, MD, Susan M. Polizzi, MD, Karen Bickett; Bryan LGH Heart Institute, Lincoln, Nebraska: Andrew Merliss, MD, Steven K. Krueger, MD, June Christy, RN; California Pacific Medical Center, San Francisco, California: Steven C. Hao, MD, Richard H. Hongo, MD, Eric J. Bernier, RN, Gina Im; Cardiovascular Associates, Kingsport, Tennessee: Greg Jones, MD, Arun Rao, MD, Tammy Dicken; Cardiovascular Medical Group of Southern California, Beverly Hills, California: Eli S. Gang, MD, Ronald P. Karlsberg, MD, Maria M.Thottam, Tracey S. Gerez; Center at St. Francis Hospital, Roslyn, New York: Steven M. Greenberg, MD, Rebecca Seeman, RN, Nedda Easterling; Center for Cardiac Arrhythmias, Houston, Texas: Hue-Teh Shih, MD, Candace Pourciau; Comprehensive Cardiovascular Care, Milwaukee, Wisconsin: Masood Akhtar, MD, Anthony Chambers, RN; Deborah Heart & Lung Center, Trenton, New Jersey: Raffaele Corbisiero, MD, Linda Dewey, RN; Emory University Hospital, Atlanta, Georgia: Jonathan Langberg, MD, Andrew Smith, MD, Sheila Heeke, RN, Jerilyn Steinberg, RN; Forsyth Medical Center, Winston-Salem, North Carolina: David Smull, DO, Mark Mitchell, MD, Janice Dickson, RN; Harper University Hospital, Detroit, Michigan: Randy A. Lieberman, MD, Anne B. Mick; Heart & Vascular Institute of Texas, San Antonio, Texas: Gregory A. Buser, MD, Armistead Lanford Wellford, IV, MD, Edwin L. Whitney, MD, Steven W. Farris, RN; Henry Ford Hospital, Detroit, Michigan: Barbara Czerska, MD, Karen Leszczynski, RN; Inova Heart and Vascular Institute/ Inova Fairfax Hospital, Fairfax VA: Marc Wish, MD, Ted Friehling, MD, Jessica Wolfe, RN, Marie Blake, RN; Lahey Clinic Medical Center, Burlington, Massachusetts: Roy M. John, MD, David T. Martin, MD, Bruce G. Hook, MD, Jean M. Byrne, RN; Lancaster Heart and Stroke Foundation, Lancaster, Pennsylvania: Seth J. Worley, MD, Douglas C. Gohn, MD, Diane Noll, RN; Lone Star Arrhythmia and Heart Failure Center, Amarillo, Texas: Suresh B. Neelagaru, MD, Tanya Welch, RN; Mayo Clinic, Rochester, MN: David L. Hayes, MD, Robert F. Rea, MD, Jane Trusty, RN, Mary (Libby) Hagen, RN; Midwest Heart Foundation, Lombard, Illinois: Maria Rosa Costanzo, MD, Lea Elder, RN; Moses Cone Hospital and Lebauer Cardiovascular Research Foundation, Greensboro, North Carolina: Steve Klein, MD, Daniel Bensimhon, MD, Paul Chase; Mount Sinai Medical Center, Miami, Florida: Gervasio A. Lamas, MD, Todd J. Florin, MD, Beatriz E. Restrepo, MD, MPH; Newark Beth Israel Medical Center, Newark, New Jersey; David A. Baran, MD, Laura Adams, RN; Northwestern University, Chicago, Illinois: Jeffrey Goldberger, MD, Dinita Galvez, RN, Katherine Small; NYU Medical Center, New York, New York: Jill Kalman, MD, Cristina Surach, RN; Ochsner Health Systems, New Orleans, Louisiana: Freddy Abi-Samra, MD, Timothy Donahue, MD, Melanie Lunn, Christine Hardy; Ohio State University, Columbus, Ohio: Charles C. Love, MD, Philip E. Binkley, MD, Garrie J. Haas, MD, Leah Sanuk, RN, Laura Yamokoski, RN; Hope Heart Institute, Bellevue, Washington: J. Alan Abraham et al 717 Heywood, MD, Amy Payne, RN; Pacific Rim EP, Inglewood, CA: Koonlawee Nademanee, MD, Carla Drew; Penn Presbyterian Medical Center, Philadelphia, Pennsylvania: Kent Volosin, MD, Janet Riggs, MSN, RN; Riverside Regional Medical Center, Newport News, Virginia: Allan L. Murphy, MD, Virginia M. Oehmann, RN; Southern California Heart Centers, Los Angeles, CA: Stanley K. Lau, MD, Nita Cheng, RN, Peter Yiu; Spokane Cardiology/Deaconess Medical Center, Spokane, Washington: Harold R. Goldberg, MD, Vickie Shumaker, RN; Stern Cardiovascular Center, Germantown, Tennessee: Frank McGrew, III, MD, Barbara Hamilton, RN; St. Joseph’s Research Institute, Atlanta, Georgia: Nirav Raval, MD, Nicolas Chronos, MD, Stephen P. Prater, MD, Sarah Conley; St. Lukes-Roosevelt Hospital Center, New York, New York: Jonathan S. Steinberg, MD, Marrick L. Kukin, MD, Robin Knox, RN, Cathleen B. Varley, RN; St. Paul Heart Clinic, St. Paul, Minnesota: Alan Bank, MD, Stuart Adler, MD, R. Dent Underwood, MD, Lisa Tindell, RN; Texas Cardiac Arrhythmia Research, Austin, Texas: Javier E. Sanchez, MD, G. Joseph Gallinghouse, MD, Deb S. Cardinal, RN, Chantel M. Scallon, RN; Tyler Cardiovascular Consultants, Tyler, Texas: Stanislav Weiner, MD, Linda Holt; University of Alabama, Birmingham, Alabama: Jose Tallaj, MD, Tom McElderry, Jr., MD, Karen Rohrer, RN; University of South Florida Heart Health, Tampa, Florida: Bengt Herweg, MD, Robyn Aydelott-Nuce, RN, Mary Ann K. Yarborough, RN; University of Texas Southwestern Medical Center, Dallas, Texas: Jose Joglar, MD, Owen Obel, MD, Carol Nguyen, RN, Dana Red, RN; University of Wisconsin, Madison, Wisconsin: Nancy Sweitzer, MD; Vanderbilt Heart and Vascular Institute, Nashville, Tennessee: Mark Wathen, MD, Darwood Darber, MD, Nancy M. McDonough, RN, Lindee D. Dye, RN; Virginia Commonwealth University Health System/MCV Hospitals, Richmond, Virginia: Mark Wood, MD, Kenneth Ellenbogen, MD, Michael Hess, MD, Kim Hall, RN. Appendix 2 Core Laboratories Cardiopulmonary Stress Test: Rochelle Goldsmith, Columbia University; Echocardiography: Marco DiTullio, Columbia University; NYHA Blinded Core Lab: Steven P. Schulman, Johns Hopkins University. Appendix 3 Committees Steering Committee: William T. Abraham (Cochairman), Alan Kadish (Cochairman), Koonlawee Nademanee, Peter Carson, Robert Bourge, Kenneth A. Ellenbogen and Michael Parides; Events Adjudication Committee: Peter Carson (Chairman), Christopher O’Connor, Inder Anand; Data Safety and Monitoring Board: Sidney Goldstein (Chairman), Stephen Gottlieb, Andrea Natale, David Naftel, David Callans.