Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
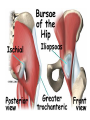
BIOMECHANICS AND ERGONOMICS 1 DPT BIOMECHANICS OF Hip joint • LECTURE # 01 Objective • • • To identify the structure of the HIP JOINT , including joint type, articular shape, and the surrounding tissues To describe joint motions occurring at the hip joint , including osteokinematic and arthrokinematic movements, muscle actions, and factors checking hip motions To understand the hip joint stability and the possible mechanisms of injury Basic function of lower extremity • Upper limb is specific for more specialized activities in large ROM • Lower Limb main function is weight bearing. • Maintenance of balance • Also involved in activities such as kicking, performing lower and high jump. Functions of the Hip • To allow mobility of the leg • To transmit the loads from the upper body to the thigh and then to the lower leg • Participate in elevating and lowering the body as in • Climbing • Raising from chair • Bringing the foot towards the body or hand • For total mobility hip motion is accompanied by the movement of the lumber spine Structure of the Hip joint •ball-and-socket joint • head of femur • acetabulum • heavy joint capsule • many reinforcing ligaments • less freedom of movement than shoulder joint Hip Joint vs. Shoulder Joint Hip Joint is a weight bearing joint, shoulder is not Acetabular fossa deeper than glenoid fossa so hip has more bony support than shoulder Hip has much stronger ligamentous support In the hip joint mobility is sacrificed for the sake of stability Both are ball and socket joints Each has a laburm to increase socket depth The Hip Joint Articular Surfaces Femoral Head •Approx. 70% of the femoral head articulates with the acetabulum Acetabular Labrum & Acetabulum . Type: Synovial Ball-and-Socket Joint The Hip Joint- ligaments Ligament of the Head of the Femur (Lig. Teres) Transverse Acetabular Lig. Ligaments iliofemoral ligament (Y ligament) • Cover the hip joint anteriorly and superiorly • taut in hip hyperextension (both slips) and full external rotation (lateral fasciculus) Ligaments • • • • pubofemoral ligaments Anterior and inferior to the hip joint taut in hip abduction and hyperextension Limit the motion of external rotation Ligament • ischiofemoral ligament – taut in hip full internal rotation and hyperextension – Limit the internal rotation • ligamentum teres – no help for the stability of the hip – from the fovea of the femoral head to the transverse acetabular ligament of the acetabulum • Abduction of the hip is limited by tension on the pubofemoral and ischiofemoral ligament • Adduction in limited by tension of the superior portion of y ligament Factors Affecting Stability of the Hip Joint bony configuration: the most important cartilage • cartilage at acetabulum thicker peripherally • acetabulum labrum deepens the shape of the acetabulum ligaments • iliofemoral ligament (Y ligament of Bigelow or Y-ligament) Motion of the Hip Joint Flexion Hyperextension Abduction Extension Adduction Motion of the Hip Joint cont. Medial Rotation Lateral Rotation Types of Movement • • different bones will move depending upon whether the limb is in weight bearing or non weight bearing Weight bearing (fixed) -foot in contact with ground and the limb is supporting weight of body – – • Pelvis moves on a fixed femur Bending down to touch toes Non Weight bearing (free) - foot free of ground and the limb is unable to support weight of body – – Femur free to move on a fixed pelvis Kicking a ball joint Structure of the Hip • proximal component: pelvis – concave acetabulum that faces anterior, inferior, and lateral • distal component: femur – Convex femoral head that faces anterior, superior, and medial • joint type: ball-and-socket joint • motions: convex on concave – hip flexion/ extension – hip abduction/ adduction – hip external/ internal rotation Hip Joint – Capsule Most Capsular Fibers Run Longitudinally and Obliquely 5-6 mm. proximal to • the acetabular margins Intertrochanteric line Ant. view Midway along femoral neck Post. view Anatomic and mechanical axes of femur Anatomical axis • Represent by a line through the femoral shaft • The neck of the femur form an angle of about 125 degree with the anatomic axis of the femur Angle of Inclination (Between the femoral neck and shaft) Approx. 125o •The angle of inclination is measured in the frontal plane and typically ranges from 115 to 140 degrees. Angle of Inclination • synonym: head-neck angle • angle between the longitudinal axis of the femoral neck to that of the femoral shaft in the frontal plane • statistics – normal adults: 125º – newborn: 140-150º • frontal plane deformities – coxa valga: angle of inclination > 125º – coxa vara: angle of inclination < 125º Angle of Inclination Coxa Vara • An angle between femoral neck and shaft less than 115°; increases stress on femoral neck. • This: 1. shortens the limb; 2. decreases the effectiveness of the abductors; 3. increases the load on the femoral neck; 4. reduces the load on the femoral head. Coxa Valga • An angle between femoral neck and shaft greater than 140°; increases pressure into the joint • This: 1. lengthens the limb; 2. mimics contracture of the hip abductors; 3. reduces the load on the femoral neck; 4. increases the load on the femoral head. Angle of Torsion The angle between the axis of the neck and the transverse axis that passes through the femoral condyles a Normal b 12o -14o Retroversion <12o c Anteversion >15o Angle of Ante version • angle of the longitudinal axis of the femoral neck to the line connecting posterior aspect of both femoral condyles in the transverse plane • statistics – normal adults and child > 6 years old: 12-15º – newborn: 30-40º Excessive Anteversion •An increase in the angle of torsion (anteversion) influences the rotation of the limb and produces a toe in gait (pigeon toes). Retroversion •A decrease in the angle of torsion (retroversion) influences the rotation of the limb and produces a toe out gait (duck feet). transverse plane deformities • anteversion: resulting in toeing-in gait • retroversion: resulting in toeing-out gait Toeing in gait