Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
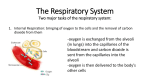
Developmental Anatomy of the Respiratory system << Mechanics of respiration Since the embryo develops in a craniocaudal (head- to- tail) direction, the upper respiratory structures (nose and pharynx) appear before the lower ones. By week 4, a thickened plate of ectoderm called the Olfactory placode (= plate) has appeared on each side of the future face. These placodes quickly invaginate to form olfactory pits that form the future nasal cavity. The nasal cavity then connects with the future Pharynx of the developing foregut. The lower respiratory organs develop from a tubular outpocketing off the foregut called the the Respiratory diverticulum or the laryngeotracheal bud . As the respiratory diverticulum elongates, its distal end enlarges to form a globular tracheal bud, which gives rise to the trachea. Soon after, the tracheal bud divides into bronchial buds, which branch repeatedly and develop with the bronchi. By 24 weeks, 17 orders of branches have formed and respiratory brochioles have developed. During weeks 6 - 16, all major elements of the lungs have been formed, except for those involved in gaseous exchange (i.e. respiratory bronchioles, alveolar ducts, and alveoli). During weeks 16 - 26, the lung tissue becomes highly vascular, and respiratory bronchioles, alveolar ducts, and some of the primitive alveoli develop. From 26 weeks to birth, many more primitive alveoli develop; they consist of type I alveolar cells (main site of gaseous exchange) and 1/3 Developmental Anatomy of the Respiratory system type II surfactant-producing cells ( surfactant is necessary to lower surface tension of alveolar fluid and thus reduce the tendency of alveoli to collapse on exhalation ) . Blood capillaries also establish close contact with the primitive alveoli. Although surfactant production begins by 20 weeks, it is present only in small quantities. Amounts sufficient to permit survival of a premature infant are not produced until 26 - 28 weeks of gestation. It is not until 26 - 30 weeks that a prematurely born baby can survive and breathe on its own. Infants born before 26 - 28 weeks are at high risk of Infant Respiratory Distress Syndrome (IRDS), in which the alveoli collapse ( due to lack of surfactant) during exhalation and must be reinflated during inhalation. At about 30 weeks, mature alveoli develop. However, it is estimated that only about one-sixth of the full complement of alveoli develop before birth; the remainder develop after birth during the first eight years of life. All the respiratory tubes are lined by endoderm and covered by splanchnic mesoderm. The endoderm becomes the lining epithelium and glands of the trachea, brochial tree, and the alveoli. The splanchnic mesoderm, by contrast, gives rise to all other layers of the tracheal and bronchial walls ( including cartilage and smooth muscle) and to the stroma (substance) of the lungs. As the lungs develop, they acquire their pleural sacs. The visceral pleura and the parietal pleura develop from Mesoderm. The space between the pleural layers is the pleural cavity. During fetal life, the lungs are filled with fluid, and all respiratory exchanges occur across the placenta.At birth, the first breaths bring air to the deflated lungs, and the alveoli inflate and begin to function. However, it takes nearly two weeks for the lungs to become fully inflated. At birth, only one-sixth of the final number of lung alveoli are present. The lungs continue to mature throughout childhood, and more alveoli are formed until young adulthood. 2/3 Developmental Anatomy of the Respiratory system CONGENITAL DEFECTS OF THE RESPIRATORY SYSTEM Other than the Infant respiratory distress syndrome (IRDS), these defects also include Agenesis of lungs, lung hypoplasia, and cystic fibrosis. Agenesis of lungs: It results from failure of the bronchial buds to develop. Agenesis of one lung is more common than bilateral agenesis, but mboth conditions are rare. Unilateral pulmonary agenesis is compatible with life. The heart and other mediastinal structures are shifted to the affected side and the existing lung is hyperexpanded. Lung hypoplasia: In infants with congenital diaphragmatic hernia, the lung is unable to develop normally because it is compressed by the abnormally positioned abdominal viscera. Lung hypoplasia is characterised by a markedly reduced lung volume. Most infants with congenital diaphragmatic hernia die of pulmonary insufficiency, despite optimal postnatal care, because their lungs are too hypoplastic to support extrauterine life. Cystic fibrosis is an inherited disease in which the function of exocrine glands are disrupted throughout the body. Cystic fibrosis affects the respiratory system by causing an oversecretion of a viscous mucus by the bronchial glands. This mucus clogs the respiratory passageways and predisposes the child to early death through repeated respiratory infections. Cystic fibrosis accounts for about 5% of childhood deaths. >> Respiratory system Quiz 3/3