Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Drug design wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
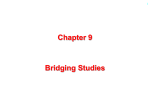
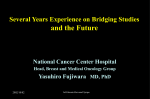
Drug interaction wikipedia , lookup
Polysubstance dependence wikipedia , lookup
Neuropharmacology wikipedia , lookup
Prescription drug prices in the United States wikipedia , lookup
Drug discovery wikipedia , lookup
Prescription costs wikipedia , lookup
Clinical trial wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Pharmacognosy wikipedia , lookup
Pharmacokinetics wikipedia , lookup
1 An Overview of Bridging Evaluations in Taiwan Chin-Fu Hsiao1, Mey Wang2, Herng-Der Chen2, Yu-Yi Hsu1 and Jen-pei Liu3 1 Division of Biostatistics and Bioinformatics National Health Research Institutes Zhunan, Taiwan 2Center 3Division for Drug Evaluation, Taipei, Taiwan of Biometry, Department of Agronomy National Taiwan University Taipei, Taiwan 2 Outline Introduction Taiwan’s Situations An Bayesian Approach Discussion 3 Introduction ICH (International Conference on Harmonisation) E5 Ethnic Factors in the Acceptability of Foreign Clinical Data The purpose of this guidance is to facilitate the registration of medicines among ICH regions by recommending a framework for evaluating the impact of ethnic factors upon a medicine’s effect, i.e., its efficacy and safety at a particular dosage and dose regimen. 4 Ethnic Difference? Targeted Clinical Trials and EGFR(Epidermal growth factor receptor) • Iressa (gefitnib) and Tarceva (Erlotinib) are targted at the EGFR pathway. • Efficacy is correlated to race number of gene copies protein expression EGFR mutation Gappuzzo et al. (JNCI, 2005), Tsao, et al (NEJM, 2005) 5 Ethnic Difference? Patients surviving (%) —— IRESSA® ------ Placebo 1.0 1.0 1.0 0.9 0.9 Asian (n = 342) 0.9 HR = 0.66 (0.48, 0.91), P = .011 0.8 0.8 0.8 RR = 12.0% 0.7 0.7 0.6 0.5 0.5 0.5 0.4 0.4 0.4 0.3 0.3 0.3 0.2 0.2 0.2 0.1 0.1 0.1 0 0 11 22 33 44 55 RR = 6.5% 0.7 0.6 0.6 0.0 0.0 Non-Asian (n = 1350) HR = 0.93 (0.81, 1.08), P = .364 0.0 6 7 8 9 10 11 12 13 14 6 7 8 9 10 11 12 13 14 15 1500 11 22 33 Time, mo 44 55 6 77 88 99 10 10 11 1112 12 13 1314 14 15 15 6 6 Objectives of ICH E5 To describe the characteristics of foreign clinical data that will facilitate their extrapolation to different populations and support their acceptance as a basis for registration of a medicine in a new region To describe regulatory strategies that minimize duplication of clinical data and facilitate acceptance of foreign clinical data in the new region To describe the use of bridging studies, when necessary, to allow extrapolation of foreign clinical data to a new region To describe development strategies capable of characterizing ethnic factor influences on safety, efficacy, dosage, and dose regimen 7 Bridging Data Package A bridging data package consists of 1) Selected information from the complete clinical data package (CCDP) that is relevant to the population of the new region, including pharmacokinetic data, and any preliminary pharmacodynamic and dose-response data, and 2) If needed, a bridging study to extrapolate the foreign efficacy and/or safety data to the new region. 8 Complete Clinical Data Package A clinical data package intended for registration containing clinical data that fulfill the regulatory requirements of the new region and containing pharmacokinetic data relevant to the population in the new region 9 Bridging Study A bridging study is defined as a supplemental study performed in the new region to provide pharmacodynamic or clinical data on efficacy, safety, dosage, and dose regimen in the new region that will allow extrapolation of the foreign clinical data to the new region. 10 Extrapolation and Similarity • If the bridging study shows that dose response, safety and efficacy in the new region are similar, then the study is readily interpreted as capable of “bridging” the foreign data • If a bridging study, properly executed, indicates that a different dose in the new region results in a safety and efficacy profile that is not substantially different from that derived in the original region, it will often be possible to extrapolate the foreign data to the new region, with appropriate dose adjustment, if this can be adequately justified (e.g., by pharmacokinetic and/or pharmacodynamic data). 11 Ethnic Factors Intrinsic Ethnic Factors are more genetic and physiologic in nature e.g., genetic polymorphism, age, gender, height, weight, lean body mass, body composition, and disease conditions, etc. Extrinsic Ethnic Factors are more social and cultural in nature e.g., environment, culture, medical practice, health insurance, practices in clinical trials or conduct 12 Bridging Studies • ICH E5 • Only after the medicine is approved in the original region • Performed in the new region 13 No Need to Bridge • Ethnically insensitive medicine: Similar medical practice and conduct of clinical trials • Ethnically sensitive medicine: Ethnically similar regions and sufficient clinical experience. 14 What to Bridge? • Data from the new region Pharmacodynamic, efficacy, safety, dosage, dose regimen • Ability to extrapolate to new region Similar in dose response, efficacy, safety either with the same doses or with dose adjustment. 15 Taiwan’s Situations 16 Taiwan Before Bridging Study An approved local clinical trial study report is required for the new drug application in Taiwan—July 7 Announcement in 1993 Disadvantage: A sample size of 40 as required would be difficult to demonstrate significant importance clinically or statistically The study design of the local trial usually only repeated a study that has been done in the foreign countries but in a smaller sample size;The study has not been designed based on the medical situation in Taiwan 17 Taiwan’s Strategy to Implement Bridging Study Smoothly convert compulsory Local Clinical Trial (LCT) to meaningful bridging study Gradually, stepwise announce waived local clinical trial Create an environment: (1) meet international regulation, ICH (2) require optimized dosage for Taiwanese patient Communicate with local and international pharmaceutical industry Announce new regulation according to the international norm and the consensus from communications Create an international platform “APEC – Taipei” Implement Double Twelve Announcement – Bridging Study 18 Stepwise Implementation 1998 Announce: two years later, switch from LCT to bridging study Many communications and negotiations with local and international pharmaceutical industry 2000, Dec.12, (Double Twelve Announcement) – public announce bridging study regulation 1998 Five announcements of LCT wavier Two years transition periods: both LCT and bridging studies acceptable from 2000 ~ 2002 Many international conferences held in Taipei and other Asian countries, regarding BS, through the APEC platform Ask CDE to complete the practical issues related to implementation of BS 2004, Jan. 1, Bridging evaluation 19 Available Statistical Methods 1. Hierarchical Model (Liu, Hsueh, and Chen, 2002, Biometrical Journal, 44: 969-981) 2. Takeuchi, M. Controlled Clinical Trials 23: 55-57, 2002 3. Shao, J. and Chow, S. C. Statistics in Medicine, 21: 1727-1742, 2002 4. Population Similarity (Chow, Shao, Hu, 2002, JBS, 12: 385-400) 5. Consistency Approach (Shih, 2001, Controlled Clinical Trials, 22: 357-366) 6. Bayesian Positive Treatment Approach (Liu, Hsiao, and Hsueh, 2002, JBS 12: 297-294) 7. Bayesian Noninferiority Approach (Liu, Hsueh and Hsiao, 2004, JBS accepted) 8. Group Sequential Approach (Hsiao, Xu and Liu, 2003, JBS, 13: 793-801) 9. Two-Stage Approach (Hsiao, Xu and Liu, 2004, submitted) 20 Products Requiring No Verification of Ethnic Insensitivity Drugs for treatment of AIDS Drugs for organ transplantation Topical agents Nutrition supplements Cathartics prior to surgery Radiolabelled diagnostic pharmaceuticals The drug is the only choice of treatment for a given severe disease Drugs for life-threatening disease have demonstrated a breakthrough efficacy Lacking adequate trial subjects for any drug used for rare disease 21 Products Requiring Verification of Ethnic Insensitivity Anticancer drugs Drugs with breakthrough efficacy Drugs of single use Drugs with different salt of the same composition and the same administered route have been approved internal Drugs for chronic psychologic or immunological diseases and conducting clinical trails internal difficultly Each compounds of new combination drug have been proved internal, and the efficacy is the same as the single compound Drugs with the mechanism, administered route, efficacy and adverse effect, similar to the approved drugs New combination composed of single compound of approved combination or compounds of approved combination has the same efficacy as approved combination Checking List for Sponsors (1 of 3) Checking List for the evaluation of Bridging Study by the Sponsor INFO Data Package Y3 N Vol., page1 I. The current status of clinical study of the drug in the world □□ II. NDA expert report or Investigator’s Brochure2 □□ III. Pharmacokinetics, safety and efficacy data related to Asian population □□ IV.Comparative analysis of Pharmacokinetics, safety and efficacy data between Asian population and others. □□ V. Self evaluation (please provide reference materials or literature) Y N U □□ □□□ □□ 2. Is the drug with a steep pharmacodynamic curve for both efficacy and safety (a small change in dose results in a large change in □□□ effect) in the range of the recommended dosage and dose regimen? □□ □□□ □□ 1. Does the drug show a Non-linear pharmacokinetics at the therapeutic dose? 3. Is the drug with narrow therapeutic dose range? Note: 1. To speed up reviewing process, please clearly indicate the volume and page number as requested. In addition to the page number, the related paragraph may be highlighted when necessary. 2. Please provide the comparative analysis of different ethnic groups, if it’s available. Please also explain if there is no comparative analysis of different ethnic groups in NDA expert report. 3. Y=yes; N=no; U=unknown 22 23 Checking List For Sponsors (2 of 3) Checking List for the evaluation of Bridging Study by the Sponsor V. Self evaluation (please provide reference materials or literature) 4. Is the drug highly metabolized, especially through a single pathway, thereby increasing the potential for drug-drug interaction ? 5. Is the drug metabolized by enzyme known to show genetic polymorphism? INFO Data Package Y2 N Vol., page1 Y N U □□ □□□ □□ □□□ □□ 6. Is the drug administered as a prodrug, with the potential for ethnically variable enzymatic conversion ? □□□ □□ 7. Is the drug with high inter-subject variation in bioavailability ? □□□ □□ 8. Is the drug with low bioavailability, thus more susceptible to dietary absorption effects? □□□ □□ 9. Is the drug with high likelihood of use in setting of multiple comedications ? □□□ □□ □□□ □□ 10. Is the drug with high likelihood for inappropriate use, e.g. analgesics and tranquilizers ? Note: 1. To speed up reviewing process, please clearly indicate the volume and page number as requested. In addition to the page number, the related paragraph may be highlighted when necessary. 2. Y=yes; N=no; U=unknown Checking List for Sponsors (3 of 3) Checking List for the evaluation of Bridging Study by the Sponsor V. Self evaluation (please provide reference materials or literature) INFO Data Package Y3 N Vol., page1 Y N U □□ 11. Is there any difference in epidemics of applied indication between the major study population and our population (including medical □□□ history, mechanism of disease development and the rate of occurrence, the efficacy and safety of other drugs in the same class)? □□ 12. Other important ethnic sensitive factors, such as “Is there any difference in the medical practice?” □□ □□□ VI. Post-marketing surveillance information □□ Overall conclusion of self evaluation (Is it clinically insignificant? What is the risk and benefit of the drug applied (such as, “Does the indication applied belong to severe disease”, “Is there a alternative therapy?”, “Are the differences of the data in ethnic factors acceptable ?) □□ Summary3 □□ Note: 1. To speed up reviewing process, please clearly indicate the volume and page number as requested. In addition to the page number, the related paragraph may be highlighted when necessary. 2. Y=yes; N=no; U=unknown 3. Please according the checking list provide an integrate summary or a brief description of all the information submitted. 24 25 Sponsor •Bridging Data Package •Summary for the Consideration of Bridging Study BoPA Accept submission Checking List Expert Consultants (Statistical, Clinical, Pharmacokinetics reviewers) CDE CDE acceptance verification Technical Review (Designate reviewer) Review meeting Schedule Sponsor meeting Supplement Result of Evaluation: 1. No Bridging study required 2. Bridging study is required – Type of Bridging study Sponsor meeting Clinical Review Committee Notification Review report and Recommendation: 1. No Bridging study required 2. Bridging study is required – Type of Bridging study 26 m ph ar ne eq u at e /in rie n su f fi xp e cie n lo gy rn at a 40 td As ia io in em ce ep id ct er n nc ef fe co nc e co d 21.1 ef fic ac y sa fe ty fo o ic s tio n ac te r 21.1 in ad in et ic s od yn am ac m ug ok in Reasons for not waived/total cases (%) 60 re s/ ph ar tic dr ug - dr ac m 80 un fa m ilia ok i ac ph ar 27 100 71.1 55.3 47.4 31.6 21.1 20 5.3 2.6 0 28 Does bridging strategy of ICH E5 warrant further implementation? Is Taiwan on the right way? 29 Case I Drug A is a fixed combination of 200mg dipyridamole/25mg aspirin 1bid for prevention of recurrent stroke After the standard process of BSE, we decided to request a bridging study due to an ethnic difference in medical practice (much lower dose for one of the components in Taiwan) and higher headache-associated dropout rate in previous Philippine study 30 Case I Headache drop out rate: Phillipino > Caucasian Local Bridging Study Result : first 4 weeks Group Placebo Reduced Dose 2wk Full Dose Full Dose 2wk 4wk Headache 8.7% 6.7% 16.3% drop out rate Risk Management: Change labeling’s instruction for use 31 Case II Drug B is a new potent lipid-lowering agent The PK study in Japanese shows that Cmax of Japanese is 1.9~2.5 times of that for Caucasian while AUC is 2~2.5 times Although the mean interracial difference is not substantial, Taiwan approved the drug with reduced maximal dosage due to the dose-dependent, drug-related rare SAE of rhabdomyolysis 32 Case II The decision is further echoed by US FDA After reviewing the results of a Phase IV PK study in Asian-Americans, FDA urged the physician to reduce the starting dose and prescribe high dose with caution for Asians in Labeling in March, 2005 33 Bayesian Approach 34 Bayesian Approach For bridging studies Small sample size No power Information on dose response, efficacy and safety of the original region can not be concurrently obtained from the local bridging studies but are available in the trials conducted in the original region Need to borrow “strength” from CCDP of the original region Information on dose response, efficacy and safety of the original region can and should be incorporated in a statistically sound manner to evaluate bridging evidence by local bridging studies 35 Assumption, Notation and Hypotheses We focus on the trials for comparing a test product and a placebo control Xi and Yj are some efficacy responses for patients i and j receiving the test product and the placebo control respectively in the new region Xi’s and Yj’s are normally distributed with known variance σ2 μNT and μNP are the population means of the test and placebo, respectively, and let ΔN = μNT - μNP H0: ΔN 0 vs. HA: ΔN > 0 36 Use of Prior distribution The proposed mixture model of the prior distribution for ΔN is a weighted average of the noninformative and normal priors as given below π(ΔN) =γπ1(ΔN) + (1-γ)π2(ΔN) π1(.) ≡c is a non-informative prior π2(.) is a normal prior with mean θ0 and variance σ02 which summarizes the foreign clinical data about the treatment difference provided in the CCDP 0≦γ≦1 37 Marginal Density Based on the clinical responses from the bridging study in new region, ΔN can be estimated by ˆ x y . N N N The marginal density is (ˆ N 0 ) 2 m(ˆ N ) (1 ) exp , 2 2 ~ 2( 0 ) 2 ( 02 ~ 2 ) 1 where ~ 2 2 / nT 2 / nP . 38 Posterior Distribution Given the bridging data and prior distribution, the posterior distribution of ΔN is 1 ˆ ( N | N ) m(ˆ ) ( N ˆ N ) 2 exp 2 ~ ~ 2 2 1 2 2 ˆ ( ) ( ) 1 N 0 N N (1 ) exp . 2 2 ~ ~ 2 0 2 2 0 39 Bridging Evaluation Similarity on efficacy in terms of a positive treatment effect for the new region can be concluded if the posterior probability of Similarity PSP P( NT NP 0 | bridging data and prior ) ( N | ˆ N )d N 0 1, for some pre-specified 0 < < 0.5. 40 Example The CCDP provides the results of three randomized, placebo controlled trials for a new antidepressant (test drug) conducted in the original region The primary endpoint is the change from baseline of sitting diastolic blood pressure (mmHg) at week 12 A bridging study was conducted in the new region to compare the difference in efficacy between the new and original region 41 Three Scenarios The first scenario presents the situation where no statistically significant difference in the primary endpoint exists between the test drug and placebo (2sided p-value = 0.6430 The second situation is that the mean reduction of sitting diastolic blood pressure at week 12 of the test drug is statistically significantly greater than the placebo group (2-sided p-value < 0.0001) The third scenario is the situation where due to the insufficient sample size of the bridging study, no statistical significance is found between the test drug and placebo although the magnitude of the difference between the test drug and placebo observed in the original region is preserved in the new region (2-sided p-value = 0.0716) Region Statistics 42 Treatment Group Drug Placebo N 138 132 Mean -18 -3 Standard Deviation 11 12 N 185 179 Mean -17 -2 Standard Deviation 10 11 N 141 143 Mean -15 -5 Standard Deviation 13 14 New 1 N 64 65 (Example 1) Mean -4.7 -3.8 Standard Deviation 11 11 New 2 N 64 65 (Example 2) Mean -15 -2 Standard Deviation 11 11 New 3 N 24 23 (Example 3) Mean -11 -4 Standard Deviation 13 13 Original 1 Original 2 Original 3 43 0.0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1.0 Example 1 1.0000 0.6789 0.6789 0.6789 0.6789 0.6789 0.6789 0.6789 0.6789 0.6789 0.6789 Psp Example 2 1.0000 0.9999 0.9999 0.9999 0.9999 0.9999 0.9999 0.9999 0.9999 0.9999 0.9999 Example 3 1.0000 0.9727 0.9700 0.9690 0.9685 0.9682 0.9680 0.9678 0.9677 0.9676 0.9675 44 Scenario I If the regulatory agency allows all information of the original region to be used for evaluation of similarity between the new and original region, γ is set to be 0 and hence PSP 1.00 If γ ≧ 0.1, then PSP always drops to around 0.6789 45 Scenario II The values of PSP in Example 2 appear to be close to 1.00 regardless of the choice of γ 46 Scenario III • The values of PSP are all greater than 0.9675 for all values of γ between 0 and 1 • With the strength of the substantial evidence of efficacy is borrowed from the CCDP of the original region, our procedure can prove the similarity of efficacy between the new and original region when a non-significant efficacy result but with a similar magnitude is observed in the bridging study 47 Final Remarks The proposed prior is a weighted average of a non-informative prior and a normal prior The proposed procedure can avoid the situation of concluding similarity between the new and original region when the efficacy result of the test drug observed the bridging study of the new region is same as or even worse than that of the placebo group Our proposed procedure can reach a conclusion that is more consistent with the results obtained from the bridging study 48 Final Remarks Selection of weight γ by the regulatory agency in the new region should consider all differences in both intrinsic and extrinsic ethnical factors between the new and original regions and at the same time should also reflect their belief on the evidence of efficacy provided in the CCDP of the original region 49 Final Remarks We use a normal prior for summarization of the results in CCDP of the original region We also use other prior distributions I) double exponential distribution II) lognormal distribution Other different distributions used for π2 reach the same conclusion 50 Thanks for your attention!