Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
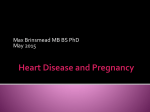
Brief Review Aortic Diameter, Aortic Stiffness, and Wave Reflection Increase With Age and Isolated Systolic Hypertension Michael F. O’Rourke, Wilmer W. Nichols T Downloaded from http://hyper.ahajournals.org/ by guest on May 7, 2017 he October 2004 High Blood Pressure Research Council meeting of the American Heart Association included a debate on the proposition that “aortic diameter, aortic stiffness, and wave reflection all increase with age and in isolated systolic hypertension.” This was stimulated by a series of articles1–5 that took a contrary position to change in aortic diameter and wave reflection and placed emphasis on aortic stiffness over wave reflection with aging and isolated systolic hypertension. The purpose of this review is to summarize the conventional view that has evolved over decades6 –12 but is not precisely argued in recent literature. According to this view, early wave reflection from peripheral arteries is the dominant ill effect of aging and the most logical target for therapy.12–14 between ages 20 and 80 years. Recent studies on central and aortic pressure allow for the normally high amplification of upper limb systolic pressure in youth and show that central (aortic) systolic and pulse pressure increase by 35 to 40 mm Hg between 20 and 80 years of age (ie, systolic by ⬇40% and pulse pressure by ⬎100%12,17 (Figure 2). Such change is generally attributed to arterial stiffening with age and return of reflected waves from the periphery to the heart.12 When stiffening is measured as “aortic” pulse wave velocity, there is an ⬇100% increase between ages 20 and 80 years18 (Figure 3). However, in contrast, there is little increase with age in pulse wave velocity within muscular conduit arteries of the limbs.5,18,19 There is also little difference between males and females.5,18,19 Increase in aortic diameter with age is usually invoked to explain progressively increasing prominence of the aortic knuckle in routine chest radiographs. Autopsy studies have shown a clear-cut increase in aortic surface area with age20 (Figure 4), whereas cross-sectional studies of aortic diameter by angiography21 and ultrasound22–26 have shown lesser, but still definite, increase with age, except in the most proximal part of the ascending aorta. Gender differences are largely explicable on the basis of smaller body size in women.12,19 There is some controversy on the competing effects of age, and of blood pressure change accompanying age, on aortic dilation. Cross-sectional studies cannot be expected to resolve this issue. A comparison between hypertensive and matched normotensive subjects showed a greater degree of aortic dilation in the latter.26 Longitudinal studies in patients with Marfan syndrome and cystic aortic necrosis have shown progressive aortic dilation with age but with rate of dilation decreased by antihypertensive therapy.27 Cross-sectional studies have shown aortic dilation in cystic aortic necrosis with Marfan syndrome related to central but not brachial pulse pressure.28 Pathological studies of the aging human aorta29,30 have shown that thickness of the load bearing media remains relatively constant throughout life and that wall thickening is attributable predominantly to increased width of the intimal layer. There is thinning, fraying, and fracture of the elastin fibers, together with collagenous remodeling (Table), and Observations and Measurements “Premature arterial senility” as a cardiovascular risk factor has long been of intense interest in actuarial studies, even before introduction of the cuff sphygmomanometer,6 as it had been in clinical medicine. The latter is apparent in the textbooks of Osler and Mackenzie ⬎100 years ago.7,8 In these, premature arteriosclerotic change was assessed from the pulse waveform palpated at the wrist or measured from the radial artery by sphygmography. The first graphic recording studies of the arterial pulse by Marey in 18639 noted characteristic differences between young and old persons (Figure 1), with prominent late systolic augmentation (“tidal wave”) in the latter. Mahomed10,11 confirmed these changes in the 1870s, stressing that “the tidal wave is prolonged and too much sustained,” and noting similar pulse waveform changes in asymptomatic persons with elevated arterial pressure as well as in the elderly. By 1900, these findings were used by life insurance companies to decline applicants on the basis of premature arterial senility.6 The cuff sphygmomanometer was introduced in the early 1900s, and by 1916, data had been presented to show the relationship between risk of death and systolic pressure in asymptomatic persons.6 For decades thereafter, aging change in arteries was gauged by change in arterial pressure, especially systolic and pulse pressure.15,16 But brachial systolic pressure increases by only ⬇25 mm Hg on average (⬇22%) Received October 10, 2004; first decision November 11, 2004; revision accepted December 8, 2004. From the VCCRI/University of New South Wales/St. Vincent’s Clinic (M.O.), Sydney, Australia; and the Departments of Medicine and Physiology (W.N.), University of Florida, Gainesville. Correspondence to M. O’Rourke, Suite 810, St. Vincent’s Clinic, 438 Victoria St, Darlinghurst, NSW 2010, Australia. E-mail [email protected] (Hypertension. 2005;45[part 2]:652-658.) © 2005 American Heart Association, Inc. Hypertension is available at http://www.hypertensionaha.org DOI: 10.1161/01.HYP.0000153793.84859.b8 652 O’Rourke and Nichols Aortic Change With Age 653 Downloaded from http://hyper.ahajournals.org/ by guest on May 7, 2017 Figure 1. Tracings from Marey’s original publication on the sphygmogram.9 Top, The original instrument, with base-plate applied over the radial artery, with long stylus, pivoting near the site of recording, drawing an amplified signal on smoked paper that was moved by a wind-up, clockwork mechanism. Inset is a “square wave” test to establish frequency response and instrumental artifact. Center, Sphygmograph tracings in 2 young adults, showing patterns still regarded as typical for the radial artery. Bottom, Sphygmograph tracings in 4 old men (left) and old women (right), showing typical patterns of senescence with accompanying arteriosclerosis. progressive disorganization of the media with, ultimate development of cystic medial necrosis. Such medial necrosis in the elderly is described in pathology textbooks as similar to that seen in an early age in Marfan syndrome and to be the substrate of aortic dissection, dilation, and rupture.31,32 Interpretations and Explanations Conventional explanations of all aortic changes with age are based on the physical principles of fatigue and fracture because these affect the inert elastin fibers within the aortic media.12 Elastin is the most inert substance in the body, with a chemical half life measurable in decades. The same principles of a material fatigue, as applied to natural rubber, predict fracture after some 109 cycles of 8% stretch, which is achieved in the proximal aorta within 40 years of life. Fracture is not expected within this time span, when stretch is ⬍5%, which explains relative immunity of the peripheral muscular arteries from this process.5,18,33 Fracture of the elastin fibers readily explains dilation and stiffening of the aorta with age.12 Elastin fibers normally bear aortic stresses. When they give way, the wall stretches and the vessel dilates; stresses are then transferred to the less extensible collagenous elements in the wall, just as stresses are so transferred when pressure rises in the normal artery. The latter phenomenon explains the well-known nonlinear pressure/diameter relationship in arteries. Increased stiffness of the aortic wall causes corresponding increase in aortic pulse wave velocity. Such increase in wave velocity causes the reflected wave from the peripheral arterioles to return earlier to the heart and to boost (augment) pressure in late systole rather than in early diastole.12 Such increase in wave velocity, with movement of the reflected wave from diastole into systole, explains the change in pulse waveform with age, as described by Marey, Mackenzie, Mahomed et al, and referred to above. Mahomed pointed out in 1872 that late systolic augmentation of the pulse was always greater in the brachial than radial artery and greater still in the carotid artery. This was confirmed by Kelly et al,34 who also showed in normal subjects that from 30 years onward, the late systolic peak dominates over the early systolic peak in the carotid and other central arteries;35,36 whereas the early peak or shoulder corresponds with peak 654 Hypertension April 2005 Part II Downloaded from http://hyper.ahajournals.org/ by guest on May 7, 2017 Figure 2. Change in brachial systolic pressure with age in multiple population studies70 –74 shows a steep rise from age 5 years to plateau when full body height is reached at age 18, then a subsequent rise after age 45. Aortic systolic pressure, measured at cardiac catheterization,19 increases progressively with age. After Nichols and O’Rourke.12 systolic flow. In older subjects, this shoulder on the upstroke of the pressure wave is followed by a surge of pressure in late systole caused by early return of wave reflection (Figure 5). In the elderly, the reflected wave arrives even earlier in systole and merges (or blends) with the incident (or forward) pressure wave so that there is no inflection point.12,21 These clinical studies confirmed earlier studies in experimental Figure 3. Changes in aortic pulse wave velocity (PWV; between the aortic root and the femoral artery at the groin) with age in a group of 480 human subjects with low prevalence of atherosclerosis in urban Beijing. From Avolio et al.18 animals and in computer models of the systemic arterial tree.37– 40 These expressed pulsatile pressure/flow relationships as vascular impedance and showed that the ill effects of aortic stiffening could be explained on the basis of increase in stiffness of the proximal aorta (increased characteristic impedance) and early wave reflection, which shifted impedance curves to higher frequencies12,37– 41 (Figure 5). The combined effect was to increase markedly the impedance to left ventricular ejection over the frequency band (1 to 4 Hz), which normally contains the greatest energy of the left ventricular ejection (flow) wave. Figure 4. Increase in surface area of the thoracic aorta with age in men (left) and in women (right), from the unselected autopsy study of Mitchell and Schwartz.20 O’Rourke and Nichols Aortic Change With Age 655 Age-Related Changes of Elastin Lamellae in the Human Mid-Thoracic Aorta for Young (18 – 40 years) and Old (56 –58 years) Persons who Died From Noncardiovascular Disease Young Old Measurement Mean SE Mean SE D (mm) 17.0 1.1 22.4 0.7 31.8 0.03 49.1 ⬍0.001 P ⬍0.01 WT (mm) 0.94 0.01 ILS (m) 8.7 1.1 12.0 0.9 37.8 ⬍0.05 EFD (LU/mm) 125 15 36 6 ⫺71.2 ⬍0.05 0.79 0.01 1.00 0.02 26.4 ⬍0.001 1236 162 1891 107 53.0 ⬍0.01 MT (m) T/LU (dyne/cm2 1.40 Change % D indicates, pressure-fixed external diameter; WT, wall thickness; ILS, interlaminar spacing; EFD, elastin fiber density (lamellar units/ mm); MT, medial thickness; T/LU, calculated (at mean pressure 100 mm Hg) tension per lamellar unit. *From O’Rourke et al.30 Downloaded from http://hyper.ahajournals.org/ by guest on May 7, 2017 Implications Effects of wave reflection are readily measured in terms of augmentation of the central (carotid, aortic, and left ventricular) pressure waveform. The aortic and left ventricular waveforms may be measured invasively during cardiac catheterization41– 43 or synthesized from the radial pressure waveform recorded by applanation tonometry using a Food and Drug Administration–approved process.12,44 The carotid waveform may be recorded directly by applanation tonometry1–5,34 –36,44,45 or approximated from the carotid diameter waveform.46 Measurement of augmentation requires identification of the localized peak, systolic shoulder, or inflection, which corresponds to peak aortic flow34,41 (Figure 5). This requires accurate dynamic frequency response of sensor, recorder, and convolutional process and has not been achieved in some clinical studies, as discussed specifically by Chen et al47 and Smulyan et al.43 The principal implications of aortic change with age relate to their magnitude, their effects on left ventricular function, and opportunities for therapeutic modification. It is clear (Figure 2) that conventional measurements of brachial systolic and pulse pressure underestimate the aging effect, and that aortic systolic and especially aortic pulse pressure increase far more with age than is usually perceived.12,16,17 Such changes are largely responsible for development of left ventricular hypertrophy and left ventricular dysfunction with age48 as well as renal dysfunction49,50 and progression of atherosclerosis.51 Changes can be best quantified from measurements of vascular impedance or inferred from augmentation of the central arterial pressure pulse. Augmentation of the pulse depends on the pattern of left ventricular ejection as well as on wave reflection and is decreased when left ventricular systolic function is impaired.52 Inability to maintain late systolic ejection with age12,21 may be responsible for the relative flattening of carotid34 and of calculated aortic augmentation53 with age. Knowledge of arterial change with age permits a more logical approach to drug therapy of the diseases associated with age, such as isolated systolic hypertension, cardiac failure, and angina pectoris. From what has been described Figure 5. Effects of aging on aortic pressure wave contour (time domain) and aortic impedance modulus (frequency domain). Top shows aortic pressure waves (above) and flow waves (below) in a young (left) and old (right) adult. Bottom shows impedance modulus (vertical axis) plotted against frequency in a young (at left) and old subject (at right). Increased proximal aortic stiffness with age causes increased amplitude of the initial pressure peak and increase in characteristic impedance (arrow 1). Earlier return of reflected waves from arterial terminations causes the pressure peak to move into late systole and the impedance curve to shift to the right (arrow 2). The peak of flow corresponds to the early systolic pressure peak in the young subject and to the inflection on the rising limb of pressure in the older subject. After O’Rourke.39 from pathological aortic change, it is difficult to envisage that drugs would have any major direct effect on the disorganized aged aorta. Such beneficial effects have been sought and described for the vasopeptidase inhibitor omapatrilat2 and for the age cross-link breaker AT711,54 but effects have not been substantial. No direct effect on aortic stiffness has been found for nitrates in older human adults.55–57 In very carefully controlled experimental studies on animals, nitrates have shown no direct effect on aortic characteristic impedance, despite marked effect on peripheral muscular arteries.58 In contrast to inefficacy on aortic stiffness, nitrates and other arterial dilators have marked effects on wave reflection and can virtually eliminate the late systolic augmentation 656 Hypertension April 2005 Part II caused by early wave reflection.56,59 Because this effect is confined to wave reflection, it may not be apparent when pressure is measured in the upper limb.60,61 Beneficial effect of nitrates on wave reflection14,56 can be explained on the basis of arterial dilation and of “trapping” of reflected waves in the peripheral vessels so that they do not return to the heart. Such reduction in wave reflection is achievable in low dosage without any effect on arterioles or on peripheral resistance.56,59 Most data on wave reflection have come from use of nitrates because the effect is immediate and dramatic. However, similar effects been described for perindopril and other drugs used for treatment of hypertension.13,62 Reservations on a Contrary View Downloaded from http://hyper.ahajournals.org/ by guest on May 7, 2017 There is no argument that the aorta and proximal arteries stiffen with age, whereas peripheral muscular arteries are less affected.5,18,19 There is no argument that the more distal segments of the proximal thoracic aorta dilate with age, but there is debate over whether this change is induced by age or by arterial pressure. Mitchell et al3,63 argue that “effective aortic diameter” measured indirectly using the water hammer equation is reduced in persons with isolated systolic hypertension. Such a view gains some support from Framingham data,24 which showed, after correction for age, that there is an inverse relationship between aortic diameter and brachial pulse pressure; similar findings were reported by Agmon et al from Mayo.25 In both of these studies, any pressure effect was trivial after correction for age, body size, and gender. Such a pressure-related effect may have been related to therapy (more than one third of the Agmon study group were receiving antihypertensives) or to the measuring site for pressure. Jondeau et al28 found no association between aortic diameter and brachial pulse pressure but a definite relationship of diameter with aortic pulse pressure in patients with Marfan syndrome. The Framingham group24 noted that an initially narrow aorta predisposes to higher pulsatile flow and higher pulse pressure. The concept of effective aortic diameter and its derivation was challenged by us64 on multiple grounds. The water hammer formula is only valid in a reflectionless system and must have pressure and flow measure at the same site and pulse wave velocity measured locally.12,64 Mitchell et al3 measured pressure in the carotid artery, blood flow velocity in the left ventricular outflow tract, and pulse wave velocity from the central aorta to the femoral artery. Mitchell et al5 downplayed the effect of wave reflection with age, noting in a select healthy population within the Framingham group (⬍20% of all) that carotid augmentation index decreased with age in women, although increasing in men, whereas amplitude of the forward wave increased in both genders with age. Such discordant gender differences for augmentation have not been reported previously, nor has decrease in augmentation with age. There were other anomalies in this article that we have questioned,64 – 66 including the calculation of forward pressure amplitude, reflected wave transit time, and greater distance to reflecting site (rather than reduced distance that we have described).12,21 All of these measurements depend on correct determination of the inflection point34,41 (Figure 5). Anomalies in the Mitchell articles may be methodological and related to the detection of the initial systolic shoulder in the carotid tracing (or inflection point; Figure 5). We have experienced problems with our processing of the carotid pressure waveform and have noted far greater variability with such waveforms than when we have synthesized the aortic waveform from the radial wave.67 In the second Australian High Blood Pressure (ANBP2) study, the experienced group of Cameron et al45 noted wide variation in the time from wave foot to inflection point of 5 to 300 ms and corresponding wide variation in calculated augmentation index. Their average value of 80 ms was half the value for their invasive study of aortic pressure in which augmentation index was unusually low.68 As reported by the ANBP2 group, there was no relationship between augmentation index and cardiovascular events, whereas others69 have found a positive association. This important issue comes down to the accuracy with which one can identify the inflection point or shoulder that corresponds to the peak of flow in the artery and that may be blended with the foot of the reflected wave.12,21 If this is identified too early, augmentation will be calculated high and characteristic impedance low; if identified too late, augmentation will be low and characteristic impedance falsely high. It is not possible to exclude such problems in interpretation of the Mitchell data. Until and unless the problems raised above can be excluded, the conventional approach, discussed here (with mutually supportive data from a variety of sources, all logically explicable) remains strong. References 1. Mitchell GF, Tardif JC, Arnold JMO, Marchiori G, O’Brien TX, Dunlap ME, Pfeffer MA. Pulsatile hemodynamics in congestive heart failure. Hypertension. 2001;38:1433–1439. 2. Mitchell GF, Izzo JL, Lacourciere Y, Ouellet JP, Neutel J, Qian C, Kerwin LJ, Block AJ, Pfeffer MA. Omapatrilat reduces pulse pressure and proximal aortic stiffness in patients with systolic hypertension. Circulation. 2002;105:2955–2961. 3. Mitchell GF, Lacourciere Y, Oellet JP, Izzo JL, Neutel J, Kerwin LJ, Block AJ, Pfeffer MA. Determinants of elevated pulse pressure in middle-aged and older subjects with uncomplicated systolic hypertension. Circulation. 2003;108:1592–1598. 4. Mitchell GF, Izzo JL. Evaluation of arterial stiffness. In: Hypertension Primer. 3rd ed. Dallas, Tex: American Heart Association; 2003:351–355. 5. Mitchell GF, Parise H, Benjamin EJ, Larson MG, Keyes MJ, Vita JA, Vasan RS, Levy D. Changes in arterial stiffness and wave reflection with advancing age in healthy men and women: the Framingham Heart Study. Hypertension. 2004;43:1239 –1245. 6. Postel-Vinay N. A Century of Arterial Hypertension 1896 –1996. Chichester, UK: John Wiley & Sons; 1996. 7. Osler W. The Principles and Practice of Medicine. 6th ed. Edinburgh, UK: Young J Pentland; 1898. 8. Mackenzie J. The Study of the Pulse: Arterial, Venous and Hepatic, and of the Movements of the Heart. Edinburgh, UK: Young J Pentland; 1902. 9. Marey EJ. Physiologie Medicale de la Circulation du Sang. Paris, France: Adrien Delahaye; 1863. 10. Mahomed FA. The physiology and clinical use of the sphygmograph. Med Times Gazette. 1872;II:62. 11. Mahomed FA. The aetiology of Bright’s disease and the prealbumenuric stage. Med Chir Trans. 1874;57:197–228. 12. Nichols WW, O’Rourke MF. McDonald’s Blood Flow in Arteries. 5th ed. London, UK: Arnold; 2005. 13. O’Rourke MF, Safar ME, Dzau V, eds. Arterial Vasodilation: Mechanisms and Therapy. Philadelphia, Pa: Edward Arnold; 1993. O’Rourke and Nichols Downloaded from http://hyper.ahajournals.org/ by guest on May 7, 2017 14. Stokes GS, Barin ES, Gilfillan KL. Effects of isosorbide mononitrate and AII inhibition on pulse wave reflection in hypertension. Hypertension. 2003;41:297–301. 15. Rutan GH, Kuller LH, Neaton JD, Wentworth DN, McDonald RH, Smith WM. Mortality associated with diastolic hypertension and isolated systolic hypertension among men screened for Multiple Risk Factor Intervention Trial. Circulation. 1988;77:504 –514. 16. Franklin SS, Gustin WIV, Wong ND, Larson MG, Weber MA, Kannel WB, Levy D. Hemodynamic patterns of age-related changes in blood pressure. Circulation. 1997;96:308 –315. 17. Vlachopoulos C, O’Rourke MF. Diastolic pressure, systolic pressure or pulse pressure. Curr Hypertens Rep. 2000;2:271–279. 18. Avolio AP, Chen SG, Wang RP, Zhang CL, Li MF, O’Rourke MF. Effects of aging on changing arterial compliance and left ventricular load in a northern Chinese urban community. Circulation. 1983;68:50 –58. 19. Lakatta EG, Levy D. Arterial and cardiac aging: major shareholders in cardiovascular disease enterprises: Part I: aging arteries: a “set up” for vascular disease. Circulation. 2003;107:139 –146. 20. Mitchell JRA, Schwartz CJ. Arterial Disease. Philadelphia, Pa: FA Davis; 1965. 21. Nichols WW, O’Rourke MF, Avolio AP, Yaginuma T, Murgo P, Pepine CJ, Conti CR. Effects of age on ventricular–vascular coupling. Am J Cardiol. 1985;55:1179 –1184. 22. Gerstenblith G, Frederiksen J, Yin FCP, Fortuin NJ, Lakatta EG, Weisfeldt ML. Echocardiographic assessment of a normal aging population. Circulation. 1977;56:273–278. 23. Roman MJ, Rosen SE, Kramer-Fox R, Devereux RB. Prognostic significance of aortic root dilation in the Marfan syndrome. J Am Coll Cardiol. 1993;22:1470 –1476. 24. Vasan RS, Larson MG, Levy D. Determinants of echocardiographic aortic root size: the Framingham Heart Study. Circulation. 1995;91: 734 –740. 25. Agmon Y, Khandheria BK, Meissner I, Schwartz GL, Sicks JD, Fought AJ, O’Fallon WM, Wiebers DO, Tajik AJ. Is aortic dilatation an atherosclerosis-related process? J Am Coll Cardiol. 2003;42:1076 –1083. 26. Kim M, Roman MJ, Cavallini C, Schwartz JE, Pickering TG, Devereux RB. Effect of hypertension on aortic root size and prevalence of aortic regurgitation. Hypertension. 1996;28:47–52. 27. Shores J, Berger KR, Murphy EA, Pyeritz RD. Progression of aortic dilatation and the benefit of long-term beta-adrenergic blockade in Marfan’s syndrome. N Engl J Med. 1994;330:1335–1341. 28. Jondeau G, Boutouyrie P, Lacolley P, Laloux B, Dubourg O, Bourdarias JP, Laurent S. Central pulse pressure is a major determinant of ascending aorta dilatation in Marfan syndrome. Circulation. 1999;99:2677–2681. 29. Virmani R, Avolio AP, Mergner WJ, Robinowitz M, Herderick EE, Cornhill FJ, Guo SY, Liu TH, Ou DY, O’Rourke MF. Effect of aging on aortic morphology in populations with high and low prevalence of hypertension and atherosclerosis. Am J Pathol. 1991;139:1119 –1129. 30. O’Rourke MF, Avolio AP. Lauren PD, Yong J. Age-related changes of elastin lamellae in the human thoracic aorta. J Am Coll Cardiol. 1987; 9:53A. 31. Underwood J. General and Systematic Pathology. 3rd ed.. Edinburgh, UK: Churchill Livingstone; 2000:278 –279. 32. Rubin E, Farber J. Pathology. 3rd ed. Philadelphia, Pa: Lippincott-Raven; 1999:522. 33. Hayoz D, Rutschmann B, Perret F, Niederberger M, Tardy Y, Mooser V, Nussberger J, Waeber B, Brunner HR. Conduit artery compliance and distensibility are not necessarily reduced in hypertension. Hypertension. 1992;20:1– 6. 34. Kelly RP, Hayward CS, Avolio AP, O’Rourke MF. Non-invasive determination of age-related changes in the human arterial pulse. Circulation. 1989;80:1852–1859. 35. Kelly RP, Karamanoglu M, Gibbs HH, Avolio AP, O’Rourke MF. Noninvasive carotid pressure wave registration as an indicator of ascending aortic pressure. J Vasc Med Biol. 1989;1:241–247. 36. Chen CH, Ting CT, Nussbacher A, Nevo E, Kass DA, Pak P, Wang SP, Chang MS, Yin FCP. Validation of carotid artery tonometry as a means of estimating augmentation index of ascending aortic pressure. Hypertension. 1996;27:168 –175. 37. O’Rourke MF. Steady and pulsatile energy losses in the systemic circulation under normal conditions and in simulated arterial disease. Cardiovasc Res. 1967;1:313–326. 38. O’Rourke MF. Arterial hemodynamics in hypertension. Circ Res. 1970; (suppl 2):123–133. Aortic Change With Age 657 39. O’Rourke MF. Pulsatile arterial haemodynamics in hypertension. Aust N Z J Med. 1976;6(suppl 2):40 – 48. 40. O’Rourke MF, Taylor MG. Input impedance of the systemic circulation. Circ Res. 1967;20:365–380. 41. Murgo JP, Westerhof N, Giolma JP, Altobelli SA. Aortic input impedance in normal man: relationship to pressure waveforms. Circulation. 1980;62:105–116. 42. Takazawa K. A clinical study of the second component of left ventricular systolic pressure. J Tokyo Medical College. 1987;45:256 –270. 43. Smulyan H, Siddiqui DS, Carlson RJ, London GM, Safar ME. Clinical utility of aortic pulses and pressures calculated form applanated radialartery pulses. Hypertension. 2003;42:150 –155. 44. O’Rourke MF. From theory into practice: arterial hemodynamics in clinical hypertension. J Hypertens. 2002;20:1901–1915. 45. Gatzka CD, Cameron JD, Dart AM, Berry KL, Kingwell BA, Dewar EM, Reid CM, Jennings GLR, for the ANBP2 investigators. Correction of carotid augmentation index for heart rate in elderly essential hypertensives. Am J Hypertens. 2001;14:573–577. 46. van Bortel LM, Balkenstein EJ, van der Heijden-Spek JJ, Vanmolkot FH, Staessen JA, Kragten JA, Vredeveld JW, Safar ME, Struijker-Boudier HA, Hoeks AP. Noninvasive assessment of local arterial pulse pressure: comparison of applanation tonometry and echo-tracking. J Hypertens. 2001;19:1037–1044. 47. Chen CH, Nevo E, Fetics B, Pak PH, Yin FCP, Maughan WL, Kass DA. Estimation of central aortic pressure waveform by mathematical transformation of radial tonometry pressure: validation of generalized transfer function. Circulation. 1997;95:1827–1836. 48. Hundley WG, Kitzman DW, Morgan TM, Hamilton CA, Darty SN, Stewart KP, Herrington DM, Link KM, Little WC. Cardiac cycledependent changes in aortic area and distensibility are reduced in older patients with isolated diastolic heart failure and correlate with exercise intolerance. J Am Coll Cardiol. 2001;38:796 – 802. 49. Safar ME, Levy BI, Struijker-Boudier HA. Current perspectives on arterial stiffness and pulse pressure in hypertension and cardiovascular diseases. Circulation. 2003;107:2864 –2869. 50. Safar ME, Smulyan H. Coronary ischemic disease, arterial stiffness, and pulse pressure. Am J Hypertens. 2004;17:724 –726. 51. Nissen SE, Tuzcu EM, Libby P, Thompson PD, Ghali M, Garza D, Berman L, Shi H, Buebendort E, Topol EJ. Effect of antihypertensive agents on cardiovascular events in patients with coronary disease and normal blood pressure. J Am Med Assoc. 2004;292:2217–2226. 52. Westerhof N, O’Rourke MF. The hemodynamic basis for the development of left ventricular failure in systolic hypertension. J Hypertens. 1995;13:943–952. 53. Adji A, O’Rourke M. Disparate effects of aging on indices of arterial stiffness and wave reflection. J Am Coll Cardiol. 2004;43(suppl A):528A. 54. Kass DA, Shapiro CP, Kawaguchi M, Capriotti AR, Scuteri A, deGroof RC, Lakatta EG. Improved arterial compliance by a novel advanced glycation end-product crosslink breaker. Circulation. 2001;104: 1464 –1470. 55. Fitchett DH, Simkus G, Beaudry JP, Marpole DG. Reflected pressure waves in the ascending aorta: effect of glyceryl trinitrate. Cardiovasc Res. 1988;22:494 –500. 56. Yaginuma T, Avolio AP, O’Rourke MF, Nichols WW, Morgan JJ, Roy PR, Baron DW, Branson J, Feneley MP. Effect of glyceryl trinitrate on peripheral arteries alters left ventricular hydraulic load in man. Cardiovasc Res. 1986;20:153–160. 57. Carroll JD, Shroff S, Wirth P, Halsted M, Rajfer SI. Arterial mechanical properties in dilated cardiomyopathy: aging and the response to nitroprusside. J Clin Invest. 1991;87:1002–1009. 58. Latson TW, Hunter WC, Katoh N, Sagawa K. Effect of nitroglycerine on aortic impedance, diameter, and pulse wave velocity. Circ Res. 1988;62: 884 – 890. 59. Jiang XJ, O’Rourke MF, Jin W, Liu I, Li C, Tai P, Zhang X, Liu L. Quantification of glyceryl trinitrate effect through analysis of the synthesised ascending aortic pressure waveform. Heart. 2002;88:143–148. 60. Kelly RP, Gibbs HH, O’Rourke MF, Daley JE, Mang K, Morgan JJ, Avolio AP. Nitroglycerine has more favourable effects on left ventricular afterload than apparent from measurement of pressure in a peripheral artery. Eur Heart J. 1990;11:138 –144. 61. Simkus GJ, Fitchett DH. Radial arterial pressure measurements may be a poor guide to the beneficial effects of nitroprusside on left ventricular systolic pressure in congestive heart failure. Am J Cardiol. 1990;66: 323–326. 658 Hypertension April 2005 Part II 62. London GM, Asmar RG, O’Rourke MF, Safar ME; REASON Project Investigators. Mechanism(s) of selective systolic blood pressure reduction after a low-dose combination of perindopril/indapamide in hypertensive subjects: comparison with atenolol. J Am Coll Cardiol. 2004;43:92–99. 63. Mitchell GF, Izzo JL, Lacourciere Y. Proximal aortic diameter and aortic pressure-flow relationship in systolic hypertension. Circulation. 2004; 109:e227–228. 64. O’Rourke MF, Safar ME, Nichols WW. Proximal aortic diameter and aortic pressure-flow relationship in systolic hypertension. Circulation. 2004;109:e227. 65. Harada A, Okada T, Niki K, Chang D, Sugawara M. On-line noninvasive one-point measurements of pulse wave velocity. Heart Vessels. 2002 Dec;17:61– 68. 66. O’Rourke MF, Nichols WW. Changes in wave reflection with advancing age in normal subjects. Hypertension. 2004;44:e10 –11. 67. Adji A, Hirata K, O’Rourke MF. Repeatability of indices determined from the carotid and radial waveforms, using SphygmoCor and Millar applanation tonometry. Heart, Lung and Circulation. 2004;13(suppl 2):S69 –S70. 68. Hope SA, Tay DB, Meredith IT, Cameron JD. Comparison of the generalized and gender-specific transfer functions for the derivation of aortic waveforms. Am J Physiol. 2002;283:H1150 –H1156. 69. O’Rourke MF. Ascending aortic pressure wave indices and cardiovascular disease. Am J Hypertens. 2004;17:721–723. 70. National Heart Foundation of Australia Report: Heart and Stroke Facts. Canberra, Australia: National Heart Foundation of Australia; 1995. 71. Burt VL, Whelton P, Roccella EJ, Cutler JA, Higgins M, Horan MJ, Labarthe D. Prevalence of hypertension in the US adult population: results from the Third National Health and Nutrition Examination Survey. Hypertension. 1995;25:305–313. 72. Uiterwaal CS, Anthony S, Launer LJ, Witteman JC, Trouwborst AM, Hofman A, Grobbee DE. Birth weight, growth and blood pressure: an annual follow-up of children aged 5 through 21 years. Hypertension. 1997;30:267–271. 73. Staessen J, Amery A, Fagard R. Isolated systolic hypertension in the elderly. J Hypertens. 1990;8:393– 405. 74. Report of the Second Task Force on Blood Pressure Control in Children–1987. Task Force on Blood Pressure Control in Children. National Heart, Lung, and Blood Institute, Bethesda, Maryland. Pediatrics. 1987;79:1–25. Downloaded from http://hyper.ahajournals.org/ by guest on May 7, 2017 Aortic Diameter, Aortic Stiffness, and Wave Reflection Increase With Age and Isolated Systolic Hypertension Michael F. O'Rourke and Wilmer W. Nichols Downloaded from http://hyper.ahajournals.org/ by guest on May 7, 2017 Hypertension. 2005;45:652-658; originally published online February 7, 2005; doi: 10.1161/01.HYP.0000153793.84859.b8 Hypertension is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 2005 American Heart Association, Inc. All rights reserved. Print ISSN: 0194-911X. Online ISSN: 1524-4563 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://hyper.ahajournals.org/content/45/4/652 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Hypertension can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Hypertension is online at: http://hyper.ahajournals.org//subscriptions/