Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
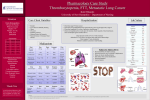
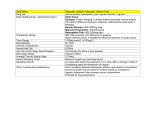
Student Name: Robyn Begalke 1045075 Nursing Assessment Form Client Name: J.M. Medical Diagnosis: SEE PATHOLOGY RECORD Client Perception of Health Needs: Assistance with ADL’s and hygiene. Client Goals for Health: To be assisted with toileting to avoid being incontinent. Allergies (food, medication, environmental) No known allergies. Medications Dietary considerations Vital Signs SEE MEDICATION RECORD - T 36.2 diet cut up, scheduled HS snack refused assist table fluids are regular (thin) 1 person assist for set up and supervision provide intermittent encouragement to improve consumption P 62 HEALTH ASSESSMENT DATA Physiological Variable R 12 BP 118/60 O2 sats 92% Pain rating 0 Student Name: Robyn Begalke 1045075 HEALTH ASSESSMENT DATA General Appearance/Mental State: Female, 90 years old. English speaking. Pleasant and quiet, doesn’t maintain eye contact when in conversation. Prefers to wear lipstick, have her hair combed in a specific way, likes to dress nicely and doesn’t like slippers/shoes. Lays/sits stiffly and isn’t able to reposition herself. Dry skin on legs and feet bilaterally. Oriented to person, place and time. Cooperative and enjoys attention from health care team. Speaks coherently and often. Likes to attend community activities and enjoys company. GCS of 15 but suffers from dementia and depression. Occasionally confused. Cardiovascular System: - Has been diagnosed with congestive heart failure, atrial fibrillation, dyslipidemia and benign hypertension - On anticoagulant therapy to minimize risk of clot formation - No bruising or signs of bleeding noted - BP: 118/60, P: 62 weak and irregular - Apical pulse 62, strong and irregular - S1 and S2 sounds identified on all cardio sites with no additional sounds noted, but muffled and slow - Popliteal, dorsalis pedis and posterior tibial pulses unpalpable bilaterally - All extremities warm to touch - Capillary refill < 3 seconds on upper and lower extremities bilaterally - Mild pitting edema to right foot < 2 seconds Student Name: Robyn Begalke 1045075 HEALTH ASSESSMENT DATA Respiratory System: - 12 respirations per minute deep and unlaboured - SPO2 of 92% on room air - Lung sounds clear in right and left upper lobes - Fine crackles noted in right middle lobe and right and left lower lobes bilaterally - Symmetrical chest expansion - Bronchial, bronchovesicular and vesicular sounds heard - Slight labour in breathing after too many deep breaths in a short period of time - No cough noted Gastrointestinal System: - Patient eats well, usually over 75% of her meal - Patient eats better with company and enjoys her meal mates - Appears hydrated, skin turgor < 2 seconds, no tenting noted, mucous membranes and lips moist - Has natural teeth - Hyperactive bowel sounds in all 4 quadrants, high pitched - History of frequent constipation and refuses suppository, but is able to go with adequate fluid intake and prune juice - Abdomen distended but soft on palpation - Has bowel incontinence and wears a large brief Urinary System: - Incontinent of urination and wears large sized brief - No distension of the bladder - Usually voids x 2 per shift - Drinks well when offered hot water - Urine is clear light yellow - Has history of UTI’s Sensory Systems: - Wears eyeglasses on a regular basis - No hearing aid and doesn’t show any significant signs of hearing deficit - Has no signs of peripheral neuropathy - Speech is slightly delayed but is able to speak and comprehend well - Reports some occasional nerve pain in the lower extremities Student Name: Robyn Begalke 1045075 HEALTH ASSESSMENT DATA Nervous System: Integumentary System: - Alert and oriented to person, place and - Skin pink and warm to touch time - Thin, dry hair - GCS of 15 - Skin turgor of < 2 seconds and no - Pupil size approximately 2mm, equal tenting noted and reactive - Many moles everywhere - No paralysis and has feeling in all - Has a rash under breasts from moisture extremities - Patient has a braden score of 16: mild - Occasionally confused due to dementia risk but is more often aware of - Is often moist in her brief and can only surroundings and situation make small positional adjustments without assistance Musculoskeletal System: - Limited mobility - Limited ROM - Has suffered a fracture to the right femur and tibia with a right sided knee replacement - Is very stiff in the mornings - Is able to sit up without much assistance but is unable to move limbs on her own - Unable to weight bear or walk - Requires full assistance with dressing, toileting, and is a mechanical lift transfer - Requires assistance in getting around in wheelchair, cannot use feet or arms to move herself - Has history of falls - Weak against resistance Endocrine System: - Patient is able to regulate hormones naturally Reproductive System: - Post menopausal - Has no symptoms that would indicate reproductive system pathology - Has two sons and a daughter - “Too many grandchildren to count” Client Resuscitation Status: MI: interventions appropriate excluding resuscitation and ICU care, transfer to acute care is considered if appropriate, surgery is considered with aim at symptom relief, deterioration should be discussed with family and power of attorney Student Name: Robyn Begalke 1045075 HEALTH ASSESSMENT DATA Spiritual Variable (Environment) - Client practices Pentecostal religion - Enjoys going to church as evidenced by her attending services often - Taught Sunday school before retirement Developmental Variable (Environment) - In Erickson’s stages of development, patient is in ego-integrity vs. despair - Hard to determine which end of the continuum client is leaning towards, diagnosed with depression and has occasional spurts of sadness but generally seems outwardly content - Does not seem to be afraid of her diagnoses Sociological Variable (Environment) Psychological Variable (Environment) - Client enjoys to have company - Suffers from dementia and depression - Enjoys meal times with her table mates - Enjoys interacting with others - Spends time watching TV alone in her - Has many photos of family in her room room - Takes pride in her appearance and - Likes to have her door open but enjoys wearing lipstick occasionally feels self conscious when - Feels self-conscious about herself and neighbouring residents have visitors her dependence on health care staff - Daughter visits multiple times a week to keep her company Determinants of health impacting client’s health (Environment) - Client is bed and wheelchair bound and cannot ambulate - Inability to perform daily activities without extensive assistance - At risk for falls, impaired skin integrity, emotional distress, loneliness, helplessness Interdisciplinary Team Members - Physician - RN, LPN, SPN - HCA - Dietary - Occupational therapy - Pharmacy - Family members (offspring), husband deceased Student Name: Robyn Begalke 1045075 HEALTH ASSESSMENT DATA Health Priorities - To maintain fluid balance, skin integrity, adequate perfusion, blood pressure - To stimulate the client to keep her occupied - To protect the client from falls - To ensure the client maintains adequate fluid intake to avoid dehydration related complications - To limit the risks for bleeding associated with anticoagulant therapy - To keep pain to a minimum - Avoid further decline in bladder control Client Strengths - Has a relatively happy outgoing demeanour and likes to be actively involved in maintenance of health - Very cooperative and trusting in health care staff - Client is able to feed independently - Is very polite to staff and other residents - Can remember her past and the life she has lived/accomplishments she is proud of - Is able to laugh and have fun in spite of her depression and dementia Laboratory/Radiology Reports Most recent April 16 2015 - RBC – L 97 - HCT – L 3.31 - Creatnine – H 117 - Pottassium H 5.2 - INR H 3.2 Student Name: Robyn Begalke 1045075 Pathophysiology Record Must be written in your own words (i.e., as if teaching a patient) Medical Diagnosis Congestive Heart Failure (CHF) (Primary Diagnosis) Atrial Fibrillation (Secondary Diagnosis) Pathophysiology The heart is unable to pump enough blood to sustain the body’s requirements, the blood moves through the body at a slower rate and pressure in the heart increases. The heart tries to compensate by thickening its walls to keep blood moving but it causes the heart to become weaker. This condition is usually caused by damage to the heart muscle. It is common for an individual to present with right sided or left sided failure. The symptoms and complications vary depending on which side of the heart is affected, but often failure in one side of the heart leads to failure in the other. A heart condition causing irregular heart beats or rhythm known as an arrhythmia that can cause a blood clot to form due to irregular blood flow or pooling in the upper chambers Signs and Symptoms Left sided CHF: shortness of breath at rest and/or when laying flat, cough, crackles in the lungs, bloody sputum Right sided CHF: pitting edema in the extremities, weakness Irregular fast heart rate, palpitations or thumping in the chest, chest pain, shortness of breath, fatigue, dizziness, lightheadedness Complications Left sided CHF: buildup of fluid in the lungs, decreased urine output, arrhythmias, hypertrophy of the heart and lungs Right sided CHF: buildup of fluid in the abdomen, decreased urine output, arrhythmias and hypertrophy of the heart, weight gain Atrial fibrillation increases the risk of a stroke due to the increased risk of clot formation, can cause heart failure, and can also cause the heart muscle to become weak. Student Name: Robyn Begalke of the heart. Benign Hypertension (Secondary Diagnosis) Dyslipidemia (Secondary Diagnosis) Hypertension is consistent high blood pressure of 140/90. It is usually caused by an increase in blood volume being pumped throughout the body causing the arteries to become less elastic. Benign hypertension is usually over a prolonged period of time and escalates more slowly than malignant hypertension. It is generally asymptomatic, but will likely cause similar complications as malignant hypertension and can present with the same symptoms. We have natural fats in our body that are essential for supplying and storing energy. These fats are called lipids, more commonly known as cholesterol levels. Dyslipidemia refers to an abnormal amount of lipids in our blood, either too high or too low. With hyperlipidemia, the lipids or fats can buildup in the arteries that may lead to a partial or full blockage that can 1045075 Headache, blurred vision, nausea, weakness, confusion, fatigue and change in mental status Cardiovascular disease, stroke, damage to the heart, kidneys and eyes. Hyperlipidemia symptoms include chest pain, cramping in one or both calves while walking, sores on the toes that do not heal, sudden stroke like symptoms including one side of the face to droop, trouble speaking, weakness of one arm or leg, and loss of balance. Hyperlipidemia or high cholesterol can cause a hardening of the arteries, a buildup of fats that can cause deficient blood flow and can lead to a stroke or myocardial infarction or heart attack. Hypolipidemia symptoms are few but include thin dry hair, tooth deformity and Hypolipidemia can cause a deficiency in normal blood clotting, inability to absorb and use fat and vitamins, and abnormalities in hormone Student Name: Robyn Begalke affect blood flow to the vital organs, with hypolipidemia, low lipid levels rarely cause a problem, but can indicate the prescense of another disorder. 1045075 malnutrition. levels. It can also cause poor wound healing, increased risk for infection Student Name: Robyn Begalke Ineffective peripheral tissue Client goal: Client will perfusion related to inadequate maintain tissue perfusion to distribution of circulating blood extremities. volume secondary to congestive heart failure as Client outcome: Client will evidenced by diminished have no decline in peripheral peripheral pulses and mild perfusion and maintain mild pitting edema in the lower pitting edema of 1+ to lower extremeties. extremities bilaterally within the next week. 1045075 1) Ensure the client remains warm throughout the day to encourage blood flow. (Day, Paul, Williams, Smeltzer & Bare, 2010, p. 926) 2) Sit with the client during meal times to promote and encourage proper nutrition with adequate protein and vitamin intake, which is essential for arterial health. (Day et. al., 2010, p. 926) 3) Ensure that the client does not cross her feet while in bed or in her wheelchair. (Day, et. al., p. 927) Goal ongoing, client has shown no signs of worsening perfusion including maintenance of peripheral pulses and edema. Intervention 1) Effective, student nurse is able to ensure that the client is always warm enough by adding sweaters as needed and ensuring that she always has an extra one on her chair. Ongoing. Intervention 2) Effective, student nurse is able to provide encouragement at meal times and has been able to promote intake of nutrients. Ongoing. Intervention 3) Effective, student nurse is able to place a pillow between her legs when the client is in bed and redirects her if she begins to cross her feet in her chair. Ongoing. Risk for imbalanced fluid volume related to deficient cardiac output secondary to congestive heart failure and daily administration of diuretics. Student Name: Robyn Begalke Client goal: Client will maintain a balanced fluid volume. Client outcome: Client will maintain urine output of > 30ml per hour and demonstrate no signs of dehydration throughout the 2 weeks in my care. 1045075 1) Ensure adequate fluid intake by client by encouraging fluids. (Potter & Perry, 2014, p. 948) 2) Assessment of hydration status including urine, mucous membranes, skin turgor, blood pressure and intake patterns. (Potter & Perry, 2014, p. 948) 3) “Obtain daily weight measurements” which may indicate extreme fluid retention or loss. (Potter & Perry, 2014, p. 954) Goal ongoing; client has shown no signs of dehydration or fluid overload in the past week but will have to continue to monitor over the upcoming week. Intervention 1) Effective, student nurse is able to encourage client to drink > 500ml of hot water per 8 hour shift. Ongoing. Intervention 2) Effective, student nurse is able to assess hydration status during AM assessment and monitor vital signs. Student nurse is also able to collaborate with other health care staff to determine amount of fluid intake per shift. Ongoing. Intervention 3) Student nurse has not been effective in this intervention thus far but will ensure to take daily weight measurements beginning next week. In progress. Risk for bleeding related to decreased amount of clotting factors in the blood as evidenced by anticoagulant therapy and INR lab value. Student Name: Robyn Begalke Client goal: Client 1) Assess skin and gums for will have no bruising which may incidence of indicate a hematoma. significant bleeding. (Vallerand & Sanoski, 2013, p. 1274) Client outcome: Client will have no 2) Take all vitals before and bruising or signs of during administration of bleeding in the next anticoagulant including week. blood pressure and pulse rate and rhythm. A low BP and thready pulse could indicate blood loss. (Vallerand & Sanoski, 2013, p. 1274) 3) “Monitor stool and urine for occult blood before and periodically during therapy” (Vallerand & Sanoski, 2013, p. 1274) 1045075 Goal ongoing; client has shown no evidence of bleeding thus far but will have to remain diligent in monitoring for signs and symptoms over the next week. Intervention 1) Effective, student nurse is able to watch for any bruising on the gums during AM oral care and assess for skin bruising during morning integumentary assessment. Ongoing. Intervention 2) Effective, student nurse is able to monitor vitals every morning to ensure that they are within normal range for the client and that anticoagulant therapy is therapeutic. Ongoing. Intervention 3) Effective, student nurse is able to monitor excretions during afternoon toileting. Ongoing. Student Name: Robyn Begalke 1045075 Medication Research Record Ensure you relate the medication information to the appropriate medical diagnosis. Please use lay terms as if you were teaching a patient. Medication/Reason for Medication Order Citalopram Metoprolol Dosage/Safe Dose Action as Related to Medical Diagnosis Dose Ordered: 30 Citalopram delays the mg PO daily break down of the neurotransmitter or Safe dose: 20 mg PO chemical in the brain once daily initially, that can affect mood, may be increased to social behavior, 40mg PO once daily appetite and digestion after 1 week and sleep and memory. The delay in the breakdown of this chemical decreases the feelings of depression. Dose Ordered: 12.5 Metoprolol decreases mg PO the heart rate and BID decreases the amount of oxygen needed to Safe Dose: 25sustain the heart 100mg daily as a while increasing the single dose initially oxygen delivery to or two divided doses, the heart. Lowers may be increased blood pressure. every 7 days as needed up to 450mg/day Common Side Effects Nursing Implications Confusion, drowsiness, insomnia, weakness, abdominal pain, anorexia, nausea, diarrhea, dry mouth Monitor mood changes during therapy, monitor electrolytes, reposition slowly to minimize dizziness, provide good oral hygiene to avoid dry mouth, watch for abnormal rhythm that may lead to ventricular fibrillation and serotonin syndrome (agitation, hallucinations, tachycardia) Fatigue, weakness, anxiety, depression, bradycardia, pulmonary edema, diarrhea, constipation, hypo/hyperglycemia Take apical pulse before administering and withhold if <50bpm, administer with meals or directly after eating, reposition patient slowly to avoid orthostatic hypotension, monitor for dyspnea, bradycardia, arrhythmias and wheezing. Student Name: Robyn Begalke (immediate release) or 400mg (extended release) Sennosides Dose ordered: 8.6mg PO every bedtime Safe dose: 12-50mg 1-2 times daily Spironolactone (Aldactone) Dose ordered: 12.5 mg PO daily Safe dose: HF: 2550mg PO daily Telmisartan (Micardis) Dose odered: 80mg PO once daily Safe dose: CV risk reduction: 80mg PO once daily 1045075 Increases the accumulation of fluid and peristalsis(movement) in the large intestine resulting in increased bowel movements Cramping, diarrhea, nausea, pink-red or black-brown discoloration of urine, electrolyte imbalance Ensure sennosides are taken with a full glass of water, administer at bedtime, may take 6-12 hours to take effect, administer on an empty stomach to speed up onset Promotes the absorption of water and sodium in the kidneys to increase urination Dizziness, headache, sedation, arrhythmias, GI irritation, hyperkalemia, hyponatremia Dilates the blood vessels causing a decrease in blood pressure Dizziness, fatigue, headache, hypotension, hyperkalemia, abdominal pain, diarrhea, impaired renal function Monitor intake and output and weight daily, BP should be monitored prior to administration when adjunctive to hypertension therapy, assess frequently for hyperkalemia Reposition slowly to avoid orthostatic hypotension, encourage fluids, monitor for signs of hyperkalemia Acetaminophen (Tylenol) Furosemide (Lasix) Vitamin D Student Name: Robyn Begalke Dose ordered: When used for 500mg PO twice analgesia, relieves daily pain by increasing the pain threshold and Safe dose: 325decreasing 650mg PO q 6 hours inflammation and or 1g 3-4 times daily swelling Dose ordered: 20mg Increases the PO once daily excretion of fluid and electrolytes by decreasing the reapsorption in the kidneys 1045075 Hepatotoxicity, renal failure, rash, constipation Blurred vision, dizziness, headaches, vertigo, hearing loss, hypotension, constipation, anorexia, dry mouth, muscle cramps May be administered with food or milk to reduce gastric irritation, tablets may be crushed, monitor for fall risk, monitor intake and output and blood pressure Dose ordered: 1000 units daily Promotes the absorption of calcium in the intestine Headache, irritability, weakness, conjunctivitis, arrhythmias, hypertension, constipation, dry mouth, nausea, hypercalcemia Assess for bone pain/weakness, observe closely for hypercalcemia, encourage dietary recommendations/orders Prevents the blood from clotting Cramps, nausea, dermal necrosis, bleeding, fever Assess for signs of bleeding (gums, stool, nosebleed, unusual bruising, tarry black stools, blood in urine), evaluate PT/INR before administering, withhold if bleeding occurs, administer at the same time each day, avoid activities that may cause injury, soft toothbrush only Safe dose: 400-1000 units daily Warfarin Dose ordered: 3 mg PO once daily Safe dose: 25mg/day for 2-4 days, then adjust to INR results Administer with full glass of water, may be taken with food or on an empty stomach, monitor frequency of bowel movements Cyanocobalamin Polythylene Glycol Student Name: Robyn Begalke Dose ordered: Improves metabolism 500mcg PO daily of fats and catbohydrates to support metabolism of Vitamin B12 Dose ordered: 17g PO daily Safe dose: 17g in 8oz water may be used up to 2 weeks Bisacodyl Dose ordered: 5mg PO every 3 days PRN Safe dose: 515mg/day up to 30mg/day as a single dose 1045075 Headache, heart failure, diarrhea, hypokalemia, pulmonary edema Assess patient for signs of Vitamin B12 deficiency(pallor, neuropathy, red inflamed tongue, psychosis) prior to and during administration, administer with meals to increase absorption Increases the Abdominal bloating, Dissolve powder into 8oz of absorption of water in cramping, flatulence, nausea water prior to the GI tract to administration, assess for promote bowel abdominal distension, movements presence of bowel sounds, and usual pattern of bowel movements, assess color, consistency and amount of stool excreted Increases fluid Abdominal cramps, nausea, May be administered before buildup in the colon diarrhea, rectal burning, bedtime for AM results, and increases hypokalemia with chronic taking on an empty stomach movement use, muscle weakness with will speed up onset, do not (peristalsis) in the chronic use crush or chew enteric coated intestines tablets, avoid administration within 1 hour of milk or antacid consumption, assess for bowel sounds, abdominal distension, colour, consistency and amount of stool excreted Salbutamol (Ventolin NEB) Student Name: Robyn Begalke Dose ordered: Causes relaxation of 2.5mg(ml) via smooth muscle and sidestream every 4 dilation of the airway hours PRN to improve breathing pattern Safe dose: 2.5-5mg every 20 minutes for 3 doses, then 2.510mg every 1-4 hours PRN 1045075 Restlessness, tremor, headache, insomnia, bronchospasm, palpitations, angina, arrhythmias, hypertension, nausea, vomiting, hyperglycemia, hypokalemia Allow 1 minute between inhalations, oxygen should be set to 6-10 LPM, assess lung sounds, pulse and BP before administration and after onset, monitor pulmonary function tests prior to and during therapy, observe for bronchospasm Student Name: Robyn Begalke Nursing Care Plan - Summary 1045075 Describe the benefits of using the nursing process and the nursing concepts in your assessment and nursing care. Assessment: During my assessment of my client I was really grateful for the nursing process. I was able to use the knowledge I obtained in theory to help me make the experience more enjoyable for my client and easier for me to gather information. I was able to use the nursing process to develop a strong rapport and therapeutic relationship with my client, which made it easier for her to disclose information to me and feel more comfortable in my care. During the assessment I was able to acquire information about her emotional well-being that I may not have if I wasn’t using the tools I learned to use through the nursing process. I was also able to determine what was pertinent information and what was irrelevant, what was normal and what was abnormal and what was supported by objective findings and what wasn’t. I am grateful for my knowledge in assessments to make a difference in my client’s health and well-being. For example, during my assessment of my client’s emotional state I learned that she served in the Air Force, and that’s how she met her husband who passed away in 2010. Being comfortable with me as her caregiver gives the client the confidence that I have her best interest in mind and that I am a competent and caring practitioner. Another benefit of using the nursing process in the assessment of my client was that I was able to recognize her abnormal findings and report to the LPN so that they can be closely monitored. For example, during my head to toe assessment of my client I noted that she had mild pitting edema on her right and left feet and foot drop and without my knowledge of health assessment and the nursing process that may have gone unnoticed. Using the nursing process during my assessment I was able to learn a lot about my client and determine my Student Name: Robyn Begalke 1045075 priorities for her care. Nursing Care: Providing nursing care for my client and other residents at the care center has been an incredible experience so far and I imagine it will continue to be exciting and rewarding. It is so enjoyable to see the difference you can make in a patients day just by spending time with them or doing the little things that they may not be able to do for themselves. I will always remember my first client, initiating my first g-tube feed, changing my first dressing and even giving my first bed bath. These things are not something that can be prepared for in the lab because it doesn’t include how you’re going to feel. I have never felt so good about what I’m doing everyday and I couldn’t imagine doing anything else. All the tedious hours spent in theory doing assignments and writing exams and lab pretending a water bottle was a g-tube were so worth it and I cant wait for more experience and time spent doing what I love. Student Name: Robyn Begalke 1045075 References Day, R. A., Paul, P., Williams, B., Smeltzer, S., & Bare, B. (2010). Brunner & Suddarth's textbook of Canadian medical-surgical nursing (2nd Canadian ed.). Philadelphia: Lippincott Williams & Wilkins. Potter, P., & Perry, A. (2013). In J. Ross-Kerr, M. Wood, B. Astle, & W. Duggleby (Eds.), Canadian fundamentals of nursing (5th ed.). Toronto, ON: Elsevier Canada. Valerand, A. H., & Sanoski, C. A. (2013). Davis’s drug guide for nurses (13th ed.). Philadelphia, PA: FA Davis Company.