Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
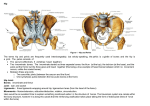
Pelvis and Hip: Evaluation and Treatment of Somatic Dysfunction Description Pelvic anatomy -hip is a region the articulation of the femoral head with the acetabulum; a “ball & socket” joint or enarthrosis which allows 360 degrees motion -joint stability deep fit of the head of the femur into the acetabulum, a strong fibrous articular capsule, & strong fibrous articular capsule , & strong muscles crossing the joint & inserting below the femoral head -synovial membranes lines the articular capsule -referred pain is commonly felt in the buttock, thigh, groin, knee, & even foot Hx PE of hip Pain - location, intensity, quality Numbness - tingling, note distribution, intensifiers Weakness - motor difficulties, gait Trauma Hx - position, audible pops, deformation, bruising, swelling, fractures, falls -attention should be on structure & function -initial survey of patient general appearance, body proportions, & ease of movement *consider the abilities of the patient & their corresponding ADLs -systematic exam including visual inspection of anatomy, palpation of bony landmarks/joint/soft tissue structures; ROM testing Pictures/Misc. Description -evaluate the inguinal region for hernias (direct & indirect) as well as vascular competency (femoral artery/vein) -palpate & evaluate the bursa of the hip region *most common is the trochanteric bursa -inspect hips anteriorly & posteriorly (standing) -note any asymmetry in the iliac crest height, the size of the buttocks, or the number & level of gluteal folds -palpate the hips & pelvis w/patient supine note any instability, tenderness, or crepitus -not any anatomical landmarks iliac crests, iliac tubercle, ASIS, PSIS, greater trochanter, ischial tuberosity, & sciatic nerve distribution GAIT OBSERVATION -ambulate the patient observation of gain can give many clues to the etiology hip/pelvic area pain -normal goat has a smooth & continuous rhythm width of the base (heel-towidth space) should be 2-4 inches -weight-bearing phase is where the majority of hip associated problems are exhibited constitutes 60% of the total ambulatory cycle -contralateral abductor contraction assists in stabilizing the pelvis & to maintain balance results in raising of the ipsilateral hip -always look above & below any joint!! is it a back or lumbar (spinal) etiology? A knee or even ankle etiology? NEUROLOGIC EXAM -DTRs -sensation (dermatomes) -muscle strength (L4, L5 & S1) Pictures/Misc. Description -special tests -Straight Leg Raise Assessment for sciatic nerve compression/irritation *Sciatic pain vs. hamstring pain *Normal straight leg raise ≈90° without pain/symptoms *Keeping knee extended, Dr flexes hip until pt reports pain -Braggards test assessment for sciatic n. compression (sciatic vs. hamstring pain) * Lower leg 5 degrees, then dorsiflex foot to stretch sciatic nerve -Laseque’s test Tests for pain specific to sciatic n. origin *Once pain is reported on SLR, Dr flexes knee & hip about 5° further. At new endpoint Dr. extends knee. Some actually bring the flexed knee to 90 and THEN straighten the knee to stretch the sciatic n. *This removes hamstring pain while adding stress onto sciatic n. *Considered abnormal if pt reports return of pain, especially if pain radiates past knee -Heel walk/toe walk Pictures/Misc. Description ROM exam Pictures/Misc. -Examine the range of motion of the hips by asking the patient to perform the following movements: -While supine, raise the leg with the knee extended above the body Expect up to 90 degrees of hip flexion -While either standing or prone, swing the straightened leg behind the body without arching the back Expect hip hyperextension of 30 degrees or less -While supine, raise one knee to the chest while keeping the other leg straight Expect hip flexion of 120 degrees -While supine, swing the leg laterally and medially with knee straight. With the adduction movement, passively lift the opposite leg to permit the examined leg full movement Expect some degree of both abduction and adduction -While supine, flex the knee keeping the foot on the table and then rotate the leg with the flexed knee toward the other leg Expect internal rotation of 40 degrees -While supine, place the lateral aspect of the foot on the knee of the other leg; move the flexed knee toward the table (Patrick test) Expect 45 degrees of external rotation Neuro exam -To test hip flexion strength, apply resistance while the patient maintains flexion of the hip when the knee is flexed and then extended Muscle strength can also be evaluated during abduction and adduction, as well as by resistance to uncrossing the legs while seated L4 -motor muscles responsible for foot inversion -DTR patellar reflex -sensory medial aspect of leg and foot SCIATIC NERVE: L4-5/S1-2-3 -The combination of 2 nerves: Tibial branch (L45/S1-3) and the Common Fibular or Peroneal branch (L4-5 / S1-2). Bifurcation occurs at the approximate level of the popliteal fossa -Largest nerve in the body Description Pictures/Misc. -Exits the pelvis through the Greater Sciatic Foramen just below the piriformis m No gluteal branches but does have a branch to the hip joint -Travels just lateral to the ischial tuberosity and along the posterior midline deep to the musculature. Localized at the midway point between the greater trochanter of the hip and the ischial tuberosity. L5 -motor = extension of extensor hallucis longus m. against resistance (ask pt to walk on heels) -no reflex! -sensory = lateral side of leg and dorsum of foot -“Walk on heels” -Origins – L4-S3 -Components Tibial nerve & Common peroneal nerve -Pathway Through greater sciatic notch, Beneath piriformis into posterior thigh (10% through), Just proximal to popliteal fossa, it branches off into common peroneal and tibial nerves -Somatic Dysfunction Piriformis: innervated S12 Description S1 -motor muscles responsible for eversion (ask pt to walk on their toes) -Achilles tendon reflex -sensory lateral malleolus and lateral aspect of foot -“Walk on your toes” Pictures/Misc. Description Hip exam summary -Inspect the hips for symmetry and level of gluteal folds -Palpate hips and pelvis for the following Instability Tenderness Crepitus -Test range of motion by the following maneuvers Flexion (120 degrees), extension (90 degrees) and hyperextension (30 degrees) Adduction (30 degrees) and abduction (45 degrees) Internal rotation (40 degrees) External rotation (45 degrees) Special testing for hip & pelvis -Test muscle strength of hips with the following maneuvers Knee in flexion and extension Abduction and adduction -Thomas Test *iliopsoas tightness (thigh off table) *rectus femoris tightness (knee flexion >90 degrees) *tensor fascia latae (knee lateral to ASIS) *IT band (foot external rotation) *key is to hold opposite knee tightly to chest -FABERE/Patrick’s *Flexion, ABduction, External Rotation *Pain reproduced before the SI joint is engaged (early ROM) indicates pain is in the acetabulum/femoral joint *Pain after the SI joint is engaged (late ROM) indicates SI as source of pain -Ely’s test *rectus femoris tightness *flexion of knee flexes or pulls hip off table -Hibb’s Test *pt prone- flex knee to 90 degree *IR & ER hip while monitoring pelvis *can use monitoring hand to confirm engagement of SI joint Pictures/Misc. Description *pain early probably from hip, later is more likely SI -Scrub test *Pt supine & hip flexed *Compress femoral head into acetabulum and maintain compressive force as you move hip through circular range of motion *Reproduction of pain indicates intra-articular source of pain -leg length discrepancy functional vs anatomic *check below both medial malleoli after balancing/straightening pelvis *treat any dysfunctions you find, & reassess OMM TESTING -standard flexion test *positive on side where the thumb moves further superiorly Pictures/Misc. Description Hip pain overview -When evaluating patients with hip pain it is likely to be from these sources: *hip joint, soft tissues around the hip and pelvis, pelvic bones, sacroiliac joint, referred pain from lumbar spine -The hip joint is one part of the pelvic girdle: (ilium, pubic ramus, and sacrum) and contains two joints the SI and the acetabular (hip) joint Imaging studies -Watch the patient walk! -Plain film X-rays: most useful for bony-severe arthritic abnormalities, trauma, and late course inflammatory disorders -CT Scan: provides superior detail of osseous structures, identifies intra-articular loose bodies, early changes of osteonecrosis Snapping Hip Syndrome -MRI: test of choice to identify soft tissue, meniscal, cartilaginous, ligamentous, tendinous, and bony abnormalities -AKA coxa saltans -IT band slips over the greater trochanter producing a “snap” or “click” *hip flexion & extension can cause voluntary “snap” -often has associated bursitis & resultant pain *pain is posterolateral area -more common in young women d/t greater Q-angle -Etiology Several causes: Bursitis, Labral tear, Physiological -Tendons around the hip subluxates over bony prominences, most commonly Iliotibial band over greater trochanter, may also be from Iliopsoas tendon subluxates over the pectineal eminence -Mechanism Iliopsoas bursitis, overuse, prominence of pelvic brim, muscle tightness -History Pain and snapping around the trochanteric area; Iliopsoas felt in groin area, both experience pain but movement not hampered Pictures/Misc. Description Fascia lata syndrome -lateral thigh pain -pain to palpation & trigger points -enlargement/inflammation of the tensor fascia lata d/t overuse or as a result of protection in injury Pictures/Misc. Description Osteitis pubis -midline pelvis & groin pain w/radiation toward the hip -common to athletes, pregnancy, post-op bladder & prostate surgery -inflammatory d/t overuse of the adductors & gracilis mm -XR will demonstrate widening of the pubic symphysis & sclerosing -tx w/NSAIDs & rest Meralgia Paresthetica -Compressive inflammation of the Lateral Femoral Cutaneous Nerve -Pain distribution: hip, thigh, groin (proximal anterior aspect of the leg/thigh), gains a “burning” or “tingling” quality -May be reproducible by tapping over the ASIS as the nerve enters the thigh under the inguinal ligament near the ASIS -Risk factors: obesity, tight belts, pregnancy, focal trauma, post-op appendectomy or hysterectomy, sports w/ repetitive hip flexion -Treatment: rest / ice / NSAIDs Pictures/Misc. Description Obturator & ilioinguinal nerve entrapment -both result from direct pressure to the nerve involved -Obturator N. aggravated most by hip flexion -ilioinguinal N. aggravated most by hip hyperextension -common reasons to develop overuse, trauma to area, sx to the area Piriformis syndrome -Compression of the Sciatic Nerve or irritation of the nerve due to piriformis activation (active or passive/spasm) *can be d/t lack of stretching, sitting on wallet -Pain localized to the buttocks and hamstring mm *May be able to palpate a hypertonic piriformis m -Hip flexion and internal rot will reproduce the pain Groin strain (adductors) -Tx: rest, ice, NSAIDs -tearing of adductor muscle -powerful over stretch, abduct, external rotation common in soccer -pain which mediates along the medial thigh, inability to run, cut, start & stop -PE pain over muscle group, incr. w/resistance, possible defect -MRI -Tx rest, ice, stretch Pictures/Misc. Description Avulsion fxs -Etiology ASIS (sartorius), AIIS (rectus), Ischial (hamstring) -Mechanism Chronic, Acute concentric/eccentric -History: Males, adolescents, local pain, limit motion -Physical Findings: tenderness, limit ROM & weakness on MMT -Imaging: AP pelvis, Oblique (iliac crest), CT -Treatment: Ice, stretch, gradual return (>2cm ORIF) Bursitis -synovial lined sacs found at areas of friction in the body designed to reduce friction between muscle & bone, ligaments, tendons, etc. -w/trauma or prolonged inflammation, communication between the bursa & a joint may occur -may require joint aspiration to assess inflammatory vs infectious quality as a “septic joint” may present with sx very similar to bursitis GREATER TROCHANTERIC BURSITIS -Pain that originates over the greater trochanteric bursa that may radiate the entire length of the leg (knee and ankle but not foot) -Etiology: Trauma to the bursa Pictures/Misc. Description -Mechanism: trauma acute or repetitive -History: Localized pain, worse rising from chair, lessens with early movement then worsens with extended movement; patients report night pain and cannot lay on affected side ;increases with hip flex/ext -Physical Findings: Local pain, swelling at greater trochanter, pain cephalad to this suggest tendinosis of gluteus medius tendon (Trendelenburg test is positive and limp) -Imaging: x-ray only to rule out other injury -Treatment: Rest, Ice, NSAIDS, Injection, Correct biomechanics OA -a gradual & progressive pain -pain increases w/motion & improves at rest -may be assoc. w/a previous injury (fx or recurrent dislocations) or an underlying rheumatologic, metabolic, or endocrine disorder -Tx rest, NSAIDs, gentle exercises to main ROM Pictures/Misc. Description Hip pointer -etiology direct trauma to ASIS, iliac crest -commonly a collision in sports -anterior/lateral pain after direct blow, pain localized -local swelling, pain, ecchymosis -XR R/o fx Osteomyelitis -Tx pain control, NAIDs, injections -A fungal or bacterial infection of the bone: Staph & Stept, Tuberculosis (M.tuberculosis) in developing nations -80% spreads from contiguous structures *20% hematogenous spread: more common in Peds (long bones) and if in an adult is more common in the spine -Pain at the site and often w/ erythema & edema -Imaging will be normal at the start; w/ progression will show demineralization & lytic lesions *MRI is preferred study Biopsy is conformational Psoas abscess -Tx IV Abx -presents as abdominal pain w/radiation toward the hip *may also have nausea, flank pain, fever, limp -w/hip flexion, it will increase pain as this engages the Psoas -muscle thought to be susceptible to infection d/t rich blood supply & proximity to lymphatic channels -most common bacteria isolated is S. aureus (80%) -CT definitive for dx -Tx IV abx & surgical incision and drainage (open vs precut) Pictures/Misc. Description Hip dislocation - Dislocation of femoral head from acetabulum -anterior, posterior, or central *10% are anterior usu. d/t MVA extremity effected is often held in abduction & external rotation *90% are posterior usu. d/t MVA (slamming your flexed knee into the seat or dash w/resultant posterior forces) extremity is shortened, internally rotated, & adducted -Etiology Genetic, instability of joint Mechanism Direct blow with hip abducted (i.e. impact while slamming on brakes), non-contact -History Pain, inability to move, numbness -Physical Findings Short leg, hip adducted, severe pain, inability to move; Evaluate sciatic nerve function by asking patients to move toes and ankle and checking sensation on plantar and dorsal aspects of foot -tx closed reduction Hip fx -a traumatic event - Falls account for ~90% of femoral neck fx’s (namely in the elderly) -May or may not accompany a dislocation -It is possible to ambulate on a hip fracture -Disruption of the blood flow to the femoral head is a consideration Pictures/Misc. Description -Plain XR of Pelvis / Hip is the study of choice -Treatment is surgical v non-surgical: orthopedist’s choice in relation to type/severity of fx, age of pt, etc. Acetabular fx -traumatic etiology often MVA w/associated femur, hip dislocation, knee injury *traumatic force driven toward the acetabular surface -XR may demonstrate the fx but CT more definitive -may have concomitant sciatic nerve injury -Tx surgical vs. non-surgical Avascular necrosis -bone infarction d/t disrupted or lack of blood flow -acute trauma -chronic stress/repetitive injury -pain radiation can be universal to hip region -XR may demonstrate one loss/decr. Density *MRI more definitive -often requires joint replacement Pictures/Misc. Description Slipped capital femoral epiphysis “SCiFE” -Pediatric condition -A loss of the alignment of the femoral epiphysis -Symptoms include early fatigue/pain w activity. Pain in hip and/or knee with even mild activity *Develop a limp -Arises due to rapid bone growth and activity in prepubescent children -May lead to avascular necrosis, increasing slippage, or degenerative arthritis -Treatment may be conservative v surgical fixation depending on the severity Pictures/Misc. Description Septic arthritis -can be a rapid development w/resultant joint destruction -hematogenous etiology - Commonly Staph aureus but need to consider gonococcal and chlamydial in the sexually active patient *Sickle Cell Pts susceptible to Salmonella -An acute hot, swollen, and tender joint (with pain on ROM testing) is septic arthritis until proven otherwise -Joint aspiration may or may not prove or disprove: aspirate WBC Ct > 50,000 cells/mm3 (~64% sensitive) +/- ESR > 30mm/h (~96% sensitive but non-specific) Anterior hip pain -Tx antibiotic (often Vancomycin IV + organism directed additional) DEGENERATIVE JOINT DISEASE (OA, COXALGIA, DJD) -Loss of articular cartilage at the hip joint -Etiology: Trauma, infection genetic , idiopathic -History: Gradual onset, anterior groin pain but may be buttock or lateral thigh, initially relieved by rest ,worse with weight bearing may proceed to night pain and limited motion -Physical Findings: Limited ROM (Internal rotation), then loss of flexion and extension; antalgic gait and abductor lerch; Positive Trendelenburg -Imaging: x-ray -Treatment: Strengthening, physical therapy for ROM – Surgical replacement OSTEONECROSIS -Loss of trabecular bone in the femoral neck usually during 3rd and 4th decade -Etiology?: Trauma (hip dislocation or femoral neck fracture), alcohol abuse steroid use, RA, SLE; other risks: sickle cell, radiation, Crohn’s, Caisson’s Pictures/Misc. Description -History: Gradual onset, groin pain but may be buttock or lateral to hip, may be sudden if femoral neck collapses LABRAL TEAR -Etiology tear of the fibrocartilaginous labrum usually due to high impact trauma; tear usually anterior labrum -Mechanism: Running, Hyperextension at hip, trauma -History: Deep sharp anterior hip pain, deep clicking or snapping, sense of instability -Physical Findings: Anterior hip pain with hip into extension, pain with anterior stress -Imaging: MRI Lateral femoral cutaneous nerve entrapment -Treatment: Rest, Surgical repair -Pain and burning (dysesthesia) or hypoesthesia over lateral thigh they may complain of groin pain and pain at SI joint *no motor involvement this is sensory nerve -Risks: obesity, tight clothing, surgery, trauma; nerve exits pelvis near ASIS -Effects young muscular women who extend their hips, women with scoliosis and joggers -rarely pathologic intra-abdominal/pelvic process Pictures/Misc. Description Psoas Syndrome General Osteology Major Extensors of the Hip Patient forward bent Leans ipsilateral to psoas spasm Ipsilateral foot everted Non-neutral L1 or L2 sidebent ipsilaterally Marked Ipsilateral psoas spasm Sacral rotation on Ipsilateral oblique axis Contralateral pelvic side shift Contralateral piriformis spasm with tender point Pain in contralateral hip -Innominate, Femur, Patella, Tibia, Fibula, Tarsals (7- Talus, Calcaneus, Navicular, Cuboid, Cuneiforms (3)), Metatarsals (5), Phalanges (14) -Gluteus Maximus strongest -Adductor Magnus -Hamstrings Biceps Femoris (red), Semitendinosus (blue), Semimembranosus (green) *Origin: Ischial Tuberosity *Insertion: Fibula/ Tibia Pictures/Misc. Description Hip Flexors -Iliopsoas Strongest flexor of thigh *Composition- Psoas major & Iliacus *Origin – T12-L5 (lateral surface of vertebral bodies) *Insertion – Lesser trochanter of femur -Rectus Femoris (blue) *Origin: AIIS/ Ilium *Insertion: Patellar Tendon *Crosses both Hip and Knee *Action: Flexes thigh at hip and extends leg at the knee What muscles comprise the quadriceps? Rectus femoris, Vastus lateralis, Vastus medialis, Vastus intermedius Abductors -Gluteus Medius (L4-S1) Sup Gluteal N (light blue) *Origin: Outer surface of Ilium *Insertion: Greater trochanter of femur -Gluteus Minimus (L4-S1) Sup Gluteal N (white) *Origin: Outer surface of Ilium, below origin of gluteus medius *Insertion: Greater trochanter of femur -Piriformis *Origin: Anterior surface of sacrum *Insertion: Greater trochanter of femur *Action: Abducts flexed thigh; Externally rotates extended thigh *Sciatic Nerve passes anterior to piriformis! Pictures/Misc. Description Adductors -Minor muscles: Gracilis, Gluteus Maximus, Pectineus -Adductor Magnus *Origin: Inferior pubic ramus; Ischial Tuberosity *Insertion: Adductor Tubercle of Femur *Action: -Adductor portion: adducts and med rotates hip. -Hamstring portion: extends hip -Adductor longus *Origin: superior pubic ramus & ant side of symphysis *Insertion: femur (medial lip in middle third) -Adductor Brevis *Origin: Inferior pubic ramus *Insertion: Femur (medial lip in upper middle third) Pictures/Misc. Description External Rotators -Piriformis (green) *Origin: Anterior surface of sacrum & sacrotuberous ligament *Insertion: Superior border of greater trochanter of femur *Action: Laterally rotate extended thigh; abduct flexed thigh; steady femoral head in acetabulum -Obturator Internus (orange) *Origin: Pelvic surface of obturator membrane & surrounding bones *Insertion: Medial surface of greater trochanter -Superior and Inferior Gemelli (yellow) *Origin: ischial tuberosity (i) & ischial spine (s) *Insertion: Medial surface of greater trochanter -Quadratus Femoris (purple) *Origin: Lateral border of ischial tuberosity *Insertion: Quadrate tubercle on intertrochanteric crest of femur & area inferior to it *Action: Laterally rotates thigh; steadies head in acetabulum Pictures/Misc. Description -Sartorius (light blue) *Origin: ASIS & superior part of notch inferior to it *Insertion: Superior part of medial surface of tibia *Action: Flexes, abducts, lat rotates thigh at hip. Flexes, med rotates leg at knee -Obturator Externus (yellow) *Origin: Margins of obturator foramen & obturator membrane *Insertion: Trochanteric fossa of femur *Action: Laterally rotates thigh; steadies head of femur in acetabulum -Gluteus Maximus (purple) *Origin: Ilium posterior to posterior gluteal line; dorsal surface of sacrum & coccyx; & sacrotuberous ligament *Insertion: Iliotibial tract & gluteal tuberosity of femur *Action: Extends thigh and assists in lateral rotation; steadies thigh & assists in rising from sitting position Internal Rotators -Tensor Fascia Lata (orange) *Origin: ASIS, anterior part of iliac crest *Insertion: Iliotibial tract, which attaches to lateral condyle of tibia *Action: Abducts and medially rotates thigh -Anterior Fibers of Gluteus Minimus (green) *Origin: External surface of ilium between anterior & inferior gluteal lines *Insertion: Anterior surface of greater trochanter of femur *Action: Abducts and med rotates thigh. Tilts pelvis on walking. -Pectineus (light blue) *Origin: Superior ramus of pubis *Insertion: Pectineal line of femur, just inferior to lesser trochanter *Action: Adducts and flexes thigh; assists with medial rotation of thigh Pictures/Misc. Description Acetabulum -Ball-and-Socket Joint -Acetabular fossa – path for hip joint to receive arterial supply via the Ligamentum capitus femoris (round ligament) -Common dislocation Posterior & Inferior FEMOROACETABULAR JOINT -Iliofemoral Ligament *Anterior aspect *Y-shaped (“Bigelow”) *Tenses with full hip extension *Strongest ligament in the body -Pubofemoral Ligament Anterior aspect -Ischiofemoral Ligament Posterior aspect; Prevents hyperextension Iliotibial Band -Thickened portion of deep fascia -Extends from Iliac crests, past the knee, to the lateral side of proximal tibia -Tendon insertion for tensor fasciae latae & gluteus maximus -Location for viscerosomatic reflexes colon, bladder DIAGNOSTIC TESTS -Ober’s Test tests for contractures of iliotibial tract *Patient lateral recumbent with tested side facing up *Knee is flexed 90˚, hip abducted 40˚ and extended to its limit *While hip extension & knee flexion maintained with pelvis stabilized, limb is gently adducted toward the examination table TREATMENT -Supine Direct Myofascial Release for Tight Iliotibial band *Palpate along iliotibial band for tightest point Pictures/Misc. Description *Using pad of thumb (reinforcing with other thumb), press medially and posteriorly on this point, using 10-30 lbs. of pressure *Maintain pressure until release is felt -kneading type treatment *Stand side opposite extremity to be treated *Flex knee to 90 degrees *Use fingers of cephalad hand to pull IT band towards you *Simultaneously carry foot away from self, increasing tension on IT band *Continue with kneading motion Pictures/Misc.