Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Neuropsychopharmacology wikipedia , lookup
Metalloprotease inhibitor wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Psychopharmacology wikipedia , lookup
Discovery and development of ACE inhibitors wikipedia , lookup
Discovery and development of cyclooxygenase 2 inhibitors wikipedia , lookup
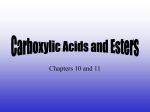
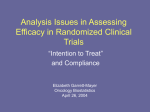
The role of COX-2 inhibitors in the perioperative setting: Efficacy and safety— A systematic review Melissa Holmes Zemmel, CRNA, MSNA Miami, Florida 2004 Student Writing Contest Honorable Mention A new class of nonsteroidal anti-inflammatory drugs (NSAIDs) selective for cyclooxygenase-2 (COX-2) offers new options for managing perioperative pain. However, new and conflicting data have emerged regarding all nonsteroidal anti-inflammatory drugs, including those selective for COX-2. The data highlight the potential for increased risks of adverse cardiovascular events associated with all NSAIDs and of potential serious skin reactions and gastrointestinal bleeding with specific agents. As of June 2005, the National Institutes of Health and Food and Drug Administration suspended all clinical trials involving NSAIDs. This article reviews 30 prospective studies on the role of COX-2 selective inhibitors in the perioperative setting. The studies examined a variety of variables, including T he management of acute perioperative pain remains a controversial issue, in part due to traditional pain management strategies that have relied heavily on the use of opioids. Recent study of the development of pain has prompted investigation into different treatment options focusing on nonopioid drugs. Nonsteroidal anti-inflammatory agents (NSAIDs) (Table 1) have long been the mainstay of nonopioid pain relief. Their inhibition of the enzyme cyclooxygenase (COX) and the resulting attenuation of inflammation make them effective analgesics. However, the use of NSAIDs in the perioperative setting is limited due to concerns regarding their effects on platelet aggregation and renal function. At least 2 isoforms of COX have been identified. The specificity of COX is an essential factor in determining the pharmacologic action of the NSAIDs. The recent development of COX-2 selective agents (Table 2) has provided additional options for the management of acute pain. Their unique pharmacologic profile makes them a promising alternative to nonselective COX-inhibitors. The COX-2 selective agents were first approved for the treatment of chronic pain, and indications exist for the treatment of osteoarthritis, rheumatoid ar- www.aana.com/members/journal/ efficacy, perioperative opioid reduction, and effects on platelet aggregation and renal function. The data reveal an overall reduction in postoperative opioid use and significant patient satisfaction with perioperative COX-2 use, no effect on platelet aggregation, and a minor negative effect on renal function. The literature suggests that perioperative use of selective COX-2 inhibitors can be well tolerated and efficacious in carefully selected patient groups. Further data are needed to fully examine the role of these drugs in the perioperative setting. Intensive research into cardiovascular issues surrounding all NSAIDs is warranted. Key words: COX-2, cyclooxygenase-2, perioperative pain, platelet aggregation, renal function. Table 1. Commonly used nonselective NSAIDs* Generic name Trade name(s) Ibuprofen Motrin, Advil, Nuprin, Medipren Indomethacin Indocin Sulindac Clinoril Diclofenac Voltaren Naproxen Naprosyn, Anaprox, Aleve Piroxicam Feldene Oxaprozin Daypro Ketorolac Toradol * NSAID indicates nonsteroidal anti-inflammatory drug. thritis, dysmenorrhea, and a variety of musculoskeletal disorders. In October 2001, celecoxib became the first COX-2 inhibitor approved for the management of acute pain in adults. In recent months, however, new and sometimes conflicting data have emerged regarding all NSAIDs, including those selective for COX-2. The data highlight the potential for increased risk of adverse cardiovascular events (including myocardial infarction, stroke, and death) associated with all NSAIDs and as increased risk AANA Journal/February 2006/Vol. 74, No. 1 49 of potential serious skin reactions and gastrointestinal bleeding associated with specific agents. As of June 2005, the National Institutes of Health and the US Food and Drug Administration (FDA) suspended all clinical trials involving NSAIDs, and focus of pharmaceutical company and FDA researchers is directed toward specific cardiovascular issues. In a series of events that began in September 2004 (Table 3),1,2 the prescription COX-2 specific agents valdecoxib (Bextra) and rofecoxib (Vioxx) were removed from the market. The prescription COX-2 specific agent celecoxib (Celebrex) and all nonprescription NSAIDs remain on the market at this time with FDAsanctioned revised labeling. In June 2005, the FDA asked all manufacturers of NSAIDs to make labeling changes to include a boxed warning highlighting the potential for increased risk of potentially life-threatening cardiovascular events and gastrointestinal bleeding associated with their use. The physiologic basis of surgical pain Surgical pain can be defined as pain that is caused by noxious stimulation due to injury. Postoperative pain is most often mediated by inflammatory mechanisms and is usually self-limiting. Inflammatory pain assoTable 2. Cyclooxygenase-2 selective inhibitors Generic name Trade name Celecoxib Celebrex Rofecoxib Vioxx Valdecoxib Bextra Parecoxib Dynastat (parenteral pro-drug of valdecoxib) ciated with surgery is characterized by a decrease in the threshold of pain sensitivity followed by central nervous system sensitization. This is accompanied by an exaggerated response to painful stimuli (primary hyperalgesia) and a spread of the hyperalgesic area to nearby uninjured tissues (secondary hyperalgesia). Primary hyperalgesia occurs mainly as a consequence of excess inflammatory and excitatory pain mediators.3 Pain is mediated peripherally at nociceptors, at the level of the spinal cord, and at the level of the brain. There are 4 physiologic processes involved in the experience of pain: transduction, transmission, modulation, and perception (Figure 1). Transduction takes place in the periphery by nociceptors. Transmission then takes place along pain pathways. These pathways conduct pain signals from the site of injury to the spinal cord and brain. Modulation is the chemical process that involves many neurotransmitters, amino acids, and inflammatory mediators to suppress or excite pain transmission. Perception is the emotional, psychological, and physiologic response to pain and is largely a subjective experience. The most important of the excitatory neurotransmitters involved in pain modulation are substance P and glutamate, which facilitate the transmission of pain signals through the central nervous system. Substance P is released peripherally at the site of tissue injury. It sensitizes nociceptors, releases histamine from mast cells, and is a potent vasodilator. Glutamate is a central mediator of pain transmission. It causes changes in membrane excitability and facilitates the activation of pain receptor systems in the central nervous system. It also has an important role in the concept of “wind-up,” which occurs when nociceptors increase the frequency Table 3. Timeline of recent events surrounding the cardiovascular issues associated with NSAIDs*1,2 September 2004 • Merck and Company, Inc, announced voluntary withdrawal of Vioxx (rofecoxib) from US and worldwide markets due to increased risk of cardiovascular events. December 2004 • NIH halts research involving naproxen and Celebrex (celecoxib) and Alzheimer disease prevention. • NIH halts research involving Celebrex and colorectal cancer prevention. • FDA issues public health advisory for all NSAIDs citing results of a long-term clinical trial that suggested increased cardiovascular risk with long-term use of NSAIDs compared with placebo. March 2005 • FDA alert is issued regarding increased risk of cardiovascular events (myocardial infarction, stroke, death) in patients receiving Celebrex based on preliminary reports from an NIH study. April 2005 • FDA asks Pfizer to voluntarily remove Bextra (valdecoxib) from the market. June 2005 • FDA asks all manufacturers of NSAIDs to make labeling changes including “a boxed warning highlighting the potential for increased risk of cardiovascular events and the well described, serious, potential life threatening gastrointestinal bleeding associated with their use.” * NSAID indicates nonsteroidal anti-inflammatory drug; NIH, National Institutes of Health; and FDA, Food and Drug Administration. 50 AANA Journal/February 2006/Vol. 74, No. 1 www.aana.com/members/journal/ Figure 1. The path of pain from surgical injury to the brain www.aana.com/members/journal/ AANA Journal/February 2006/Vol. 74, No. 1 51 and intensity of their signals as a result of repeated stimulation. The repeated stimulation of these neurons also causes them to widen their sensory range, causing previously unaffected adjacent neurons to begin firing. Wind-up occurs after prolonged exposure to painful stimuli and in the face of undertreated pain.3 Modulation of pain also includes the actions of inhibitory neurotransmitters. These include substances such as β-endorphins, serotonin, γ-aminobutyric acid, and enkephalins. These modulators function to reduce the activity of mechanisms involved in pain transmission.4 Opioid pain control takes advantage of the inhibitory neurotransmitters and receptors to produce analgesia. The binding of the opioids to various inhibitory receptors in the brain and spinal cord activates them and interrupts the transmission of pain. This takes place through the inhibition of presynaptic release or postsynaptic response to excitatory substances. Prostaglandins are the main inflammatory modulators released by injured tissues. They are formed as a result of arachidonic acid metabolism. They produce inflammation and discomfort by vasodilation, increased vascular permeability (edema), and sensitization of the tissues to pain. As inflammation progresses, more nociceptors (even those in surrounding uninjured tissues) are recruited and sensitized to pain mediators. In this way, inflammation also contributes to wind-up. When tissue is injured, phospholipases release free arachidonic acid that then is metabolized into prostaglandins by the COX. There are 2 isoforms of COX: COX-1 and COX-2. COX-1 is a constitutive enzyme and has a homeostatic role in gastrointestinal mucosa protection, platelet aggregation, and maintenance of renal function. COX-2 is expressed at sites of tissue injury to mediate pain and inflammation. COX-2 also is expressed in the brain and kidney and contributes to homeostatic mechanisms there (Figure 2). The pharmacology of NSAIDs The first recorded uses of the salicylic acid derivatives that have become modern NSAIDs date back many centuries. They were used as analgesics and antipyretics. Salicylic acid was synthesized in 1860 in Germany and was indicated for use as an analgesic, anti-inflammatory, and antipyretic. In the years that followed, other compounds were synthesized that mimicked the action of salicylic acid. These drugs were collectively referred to as NSAIDs.5 Until 1971, there was little understanding of the mechanism of action of NSAIDs. It was the work of British pharmacologist Harry Collier in the 1960s that 52 AANA Journal/February 2006/Vol. 74, No. 1 prompted modern inquiry into the biochemical basis of NSAID action. Collier hypothesized that the drugs acted by “inhibiting some underlying cellular mechanism that takes part, to different extents in different responses, and mediated by different endogenous substances.”6 The work of prostaglandin researchers Vane7 showed that the NSAIDs were capable of blocking prostaglandin synthesis in animal studies performed on dogs and rabbits. Cyclooxygenase was isolated in 1976. In the early 1990s, the existence of a second form of COX, one that was inducible in the presence of inflammatory stimuli, was suspected.8,9 The inducible form of cyclooxygenase, COX-2, was isolated in 1991.10,11 Nonselective NSAIDs are inhibitors of COX-1 and COX-2. The side-effect profile of nonselective NSAIDs is well known and is related to the inhibition of prostaglandins. These side effects include gastrointestinal irritation and bleeding, platelet inhibition, and renal dysfunction.12 Current research supports the fact that much of the unfavorable side-effect profile of nonselective NSAIDs is attributable to the inhibition of COX-1, while the analgesic and anti-inflammatory profiles are the result of the inhibition of COX-2. The recent identification of COX-2 selective agents provides a novel strategy for the relief of surgical pain. It is now possible to specifically target the prostaglandins that mediate inflammatory pain without inhibiting the gastric cytoprotective and platelet aggregating properties. Study of the perioperative use of COX-2 selective agents It is well known that NSAIDs are very effective agents for treating the pain associated with inflammation. It is also well known that much of the pain that results from surgery is caused by inflammation resulting from direct tissue injury. Nonselective NSAIDs have been used for the treatment of surgical pain for decades. However, clinical use has not gained popularity for surgical patients because of unattractive side effects, specifically inhibition of platelet aggregation. The unpleasant and sometimes dangerous side effects of opioids—nausea, vomiting, constipation, respiratory depression, and sedation—leave great room for improvement in acute pain management. This fact, coupled with the benefits of reduced inflammation achieved by NSAIDs, has prompted in-depth study of novel, nonopioid treatment options. The World Health Organization developed a 3-step strategy for the treatment of cancer pain (Figure 3). All 3 steps include the use of nonopioid drugs for the relief of pain. The first step consists of nonopioid an- www.aana.com/members/journal/ Figure 2. Cascade of inflammation through the arachidonic acid pathway in response to surgical injury Surgical tissue injury Phospholipases cleave free arachidonic acid in response to tissue injury Arachidonic acid Cyclooxygenase 1 (COX-1) Cyclooxygenase 2 (COX-2) Prostaglandins involved in: Prostaglandins involved in: Gastrointestinal mucosa protection Platelet aggregation/hemostasis Renal function homeostasis Vasodilation ↑Sensitivity to pain (hyperalgesia) ↑Capillary permeability (edema) Renal function homeostasis algesia with or without the use of an adjuvant such as an antidepressant or anxiolytic. The second step adds a mild opioid to the first. Finally, the third step adds a potent opioid. This regimen has provided satisfactory pain relief in 80% to 90% of patients studied.13 Concern regarding nephrotoxic effects surrounds the use of NSAIDs. Both isoforms of COX are known to have an important role in renal blood flow homeostasis. Preservation of renal function is a concern in surgical patients. The renal effects of perioperative selective COX-2 inhibitors, particularly in populations at high risk for NSAID-induced nephropathy, merit exploration. The discovery of COX-2 selective agents stimulated extensive and ongoing study into their efficacy and safety in a variety of settings, the first of which was the www.aana.com/members/journal/ management of chronic pain. Inquiry into the use and benefits of the COX-2 selective inhibitors in the surgical arena also has become a promising focus. Recently, a tremendous increase in the body of knowledge regarding COX-2 selective inhibitors has occurred. A systematic review of the literature was initiated to scrutinize the current data on perioperative use of selective COX-2 inhibitors. The purposes of this review were as follows: 1. Examine the current data available on the efficacy of COX-2 inhibitors in the management of acute postoperative pain across multiple surgical pain models. 2. Examine the current data available on the effects of COX-2 inhibition on platelet function. 3. Examine the current data available on the effects of COX-2 inhibition on renal function. AANA Journal/February 2006/Vol. 74, No. 1 53 Figure 3. World Health Organization analgesic ladder13 Freedom from cancer Opioid for mild to moderate Pain ± Nonopioid ± Adjuvant 3 Pain persisting or increasing Opioid for mild to moderate pain ± Nonopioid ± Adjuvant 2 Pain persisting or increasing 1 ± Nonopioid ± Adjuvant Review of the literature • Literature search. Three separate PUBMED searches were conducted for prospective, randomized, controlled studies dealing with COX-2 inhibitors in the surgical setting. The first search addressed efficacy for pain relief and was conducted for studies that included the terms COX-2, cyclooxygenase-2, acute pain, surgical pain, perioperative pain, or postoperative pain. A second search was conducted for studies dealing with platelet aggregation and bleeding time as they relate to COX-2 specific inhibitors. A third search was done for studies that addressed the effects of COX-2 specific inhibitors on renal function. • Inclusion criteria. It was determined a priori that only randomized, controlled studies that specifically addressed the topic of COX-2 selective agents and their relevance in the perioperative setting would be reviewed. Criteria for relevance in the perioperative setting included effects on platelet aggregation and bleeding time, effects on renal function, use for preemptive analgesia, and use for postoperative analgesia. Studies were assessed for sensitivity of pain scoring tools and statistical analysis. Bibliographies of articles on these subjects also were searched by hand for additional articles meeting the inclusion criteria. Discussion The 22 studies of the efficacy of pain relief were divided into groups according to established pain models. 54 AANA Journal/February 2006/Vol. 74, No. 1 The specific groups included oral surgery, abdominal surgery, orthopedic surgery, and otolaryngologic surgery. Three randomized, controlled studies that addressed the effects of COX-2 inhibitors on platelet function were identified. One study was identified that specifically examined the effects of COX-2 inhibition on surgical blood loss. Four studies were identified that examined the effects of COX-2 inhibition on renal function. Efficacy in management of postoperative pain • Orthopedic pain model (Table 4). Nine trials studying the efficacy of selective COX-2 inhibitors in the orthopedic pain model were identified.14-22 Various procedures were studied and included total knee arthroplasty, total hip arthroplasty, bunionectomy, and spinal surgery. All studies examined a selective COX-2 inhibitor and compared efficacy with another selective COX-2 agent, opioids, or placebo. Of the 9 studies, 6 examined the opioid-sparing effects of concurrent perioperative treatment with selective COX-2 inhibitors.14,16,18-20,22 All 6 studies found a significant reduction in postoperative opioid requirements (P < .05). In addition to the opioid-sparing effects, 5 of the 6 trials also found improved patient satisfaction among patients who received COX-2 inhibitors as part of their pain management regimen (P < .05).16,18-20,22 Buvanendran and Kroin22 found that in patients undergoing total knee replacement, perioperative use of oral rofecoxib reduced opioid consumption, pain, vomiting, and sleep disturbances. Improved knee range of motion and reduction in physical therapy time also was noted. Compared with placebo alone, COX-2 inhibitors were associated with less consumption of rescue medication, lower pain scores, and greater patient satisfaction.15,17,18,20 • Abdominal surgery pain model (Table 5). Four trials examining the efficacy of COX-2 inhibitors on postoperative pain after abdominal surgery were identified.23-26 Of the 4 studies, 3 reported significantly lower postoperative pain scores in the patient groups that received COX-2 inhibitors as part of the pain management regimen (P < .05).24-26 Of the 4 studies, 3 also found significant reduction in total postoperative opioid doses in groups receiving concurrent COX-2 inhibitors.22,24,25 Sinatra et al25 examined rofecoxib oral suspension as an analgesic adjunct after lower abdominal surgery. The effects of a single preoperative dose of rofecoxib (25 or 50 mg) oral suspension on postoperative morphine requirements, effort-dependent pain, and pulmonary function were measured. Postoperative morphine requirements were reduced by 44% in the 25-mg www.aana.com/members/journal/ www.aana.com/members/journal/ AANA Journal/February 2006/Vol. 74, No. 1 55 Valdecoxib, 20 or 40 1 preoperative mg PO + MSO4 by PCA; placebo + MSO4 by PCA Hip arthroplasty Hip arthroplasty Camu et al18 (n = 203) Malan et al19 (n = 181) Parecoxib, 20 or 40 mg IV; MSO4, 4 mg IV; placebo Rofecoxib, 50 mg Preoperative and PO 24 and 2 h postoperative preoperatively + 50 mg daily for 5 d + 25 mg daily for 8 d compared with matching placebo at same times Rasmussen et Orthopedic knee al21 (n = 208) surgery Buvanendran Total knee and Kroin22 replacement (n = 70) Median time to first rescue Total epidural analgesic consumption and in-hospital opioid consumption significantly less in rofecoxib group NA NA NA NA NA NS Significant Significant all groups Significant for both agents Ouset similar with all 3 agents; levels and duration of analgesia were significantly superior with parecoxib than with MSO4 Patients receiving either dose of parecoxib consumed significantly less morphine postoperatively, and duration of analgesia was significantly superior with parecoxib than with MSO4 Parecoxib, 20 and 40 mg, reduced total MSO4 in 36 h by 22.1% and 40.5%, respectively Patients receiving either valdecoxib dose required 40% less morphine than placebo Visual analog scale score significantly greater in placebo group at PACU admission MSO4 consumption in 48 h by both valdecoxib groups significantly reduced 20 mg, significant to 18 h; 40-80 mg, significant to 24 h Celecoxib, significant to 8 h; rofecoxib, significant to 16 h Quality of pain relief Other NA NS NA Significant Significant Significant Significant Significant NA NA In rofecoxib group, median pain scores lower, knee flexion greater, patient satisfaction higher, sleep disturbances significantly reduced Greater patient satisfaction noted in parecoxib groups Patient satisfaction significantly higher in parecoxib groups; MSO4 PCA discontinued earlier in both parecoxib groups Pain intensity levels and patient satisfaction significantly improved in both valdecoxib groups Patient satisfaction on global evaluation significantly greater in valdecoxib 80-mg group All groups reported significant improvement in patient satisfaction in a dosedependent manner Significant for Rofecoxib demonstrated both agents greater duration than celecoxib Opioid total dose reduction * PO indicates by mouth; PCA, patient-controlled analgesia; MSO4, morphine sulfate; bid, twice a day; IV, intravenous; PACU, postanesthesia care unit; NA, not applicable; and NS, not significant. Significant values were P ≤ .05 in favor of the cyclooxygenase-2 inhibitor. 1 after discontinuation of IV PCA on postoperative day 1 Parecoxib, 20 or 40 mg Postoperative bid IV; placebo Postoperative on request followed by doses at 12 and 24 h Hubbard et Total knee al20 (n = 195) replacement Parecoxib, 20 or 40 mg + MSO4 by PCA; placebo + MSO4 by PCA Rofecoxib, 50 mg PO; placebo Bekker et al17 Lumbar (n = 61) diskectomy 1 preoperative Valdecoxib, 40 or 80 Postoperative mg PO daily + MSO4 by PCA; placebo + MSO4 by PCA Reynolds and Total knee Hoo16 arthroplasty (n = 104) 1 preoperative Celecoxib, 200 mg PO; 1 preoperative rofecoxib, 50 mg PO; MSO4 by PCA Valdecoxib, 20, 40, or 80 mg PO; placebo Spinal fusion Analgesic agents and doses Dose timing Desjardins et Bunionectomy al15 (n = 223) Reuben and Connelly 14 (n = 60) Reference Type of surgery Table 4. Orthopedic pain model* AANA Journal/February 2006/Vol. 74, No. 1 * MSO4 indicates morphine sulfate; PCA, patient-controlled analgesia; PO, by mouth; IV, intravenous; NA, not applicable; FEV1, forced expiratory volume in 1 second; and FVC, forced vital capacity. Significant values were P ≤ .05 in favor of the cyclooxygenase-2 inhibitor. Parecoxib-valdecoxib group reported improved patient global evaluation Significant NA Parecoxib, 40 mg IV preoperatively + valdecoxib, 40 mg postoperatively and daily for 4 d Joshi et al26 Laparoscopic (n = 263) cholecystectomy Preoperative and Patients receiving parecoxib used postoperative 21% less fentanyl immediately postoperatively; pain intensity scores significantly less in parecoxib group; fewer patients receiving valdecoxib required supplemental analgesics after discharge Pulmonary function tests (FEV1 and FVC) improved in both rofecoxib groups Significant NA Pain scores at 12 h significantly lower in both rofecoxib groups at rest and after vigorous cough Preoperative Rofecoxib, 25 or 50 mg; placebo MSO4 by PCA Sinatra et Open abdominal al25 (n = 48) surgery Parecoxib and ketorolac groups had greater global evaluation scores than MSO4 group NA Significant Pain intensity significantly less with parecoxib (either dose) and ketorolac than with MSO4 Gynecologic laparotomy Parecoxib, 20 or 40 mg IV; 1 postoperative ketorolac, 30 mg IV; MSO4, 4 mg IV; placebo Barton et al24 (n = 200) Median time to Opioid total first rescue dose reduction Other NA Significant No significant difference noted in patient global evaluation Quality of pain relief Postoperative pain scales similar in all 3 groups Type of Analgesic agents Reference surgery and doses Dose timing Tang et al23 Major gynecologic MSO4 by PCA + parecoxib Postoperative (n = 60) surgery 20, or 40 mg PO on request and 12 and 24 h after initial dose Table 5. Abdominal surgery pain model* 56 group and 59% in the 50-mg group (P < .05). At 12 hours after drug administration, resting pain scores and pain scores after spirometry were lower in both rofecoxib groups compared with placebo (P < .05). Pulmonary function, measured by forced vital capacity, was best preserved in the rofecoxib 50-mg group. • Oral surgery pain model (Table 6). Six studies were identified for the oral surgery pain model.15,27-31 All studies compared a COX-2 specific inhibitor to placebo, an oral codeine derivative, or another NSAID. Of the 6 studies, 3 compared a selective COX-2 inhibitor with a nonselective NSAID.29-31 All 3 studies found analgesic efficacy of the selective COX-2 inhibitor comparable to that of the nonselective NSAID. All 3 studies also found duration of the selective COX-2 inhibitor to be longer. There were no adverse effects of selective COX-2 inhibitors noted in any of the studies. Daniels et al31 found that valdecoxib, 20 and 40 mg, demonstrated longer duration than a combination of oxycodone, 10 mg, and acetaminophen, 1,000 mg, after third molar extraction (P < .05). In a study by Chang and Frick,28 rofecoxib, 50 mg orally, was compared with a combination of codeine, 60 mg, and acetaminophen, 600 mg, after third molar extraction. Peak pain scores were lower in the rofecoxib group, and significantly more patients in the codeine-acetaminophen group experienced nausea and vomiting (P < .05).28 • Otolaryngologic surgery model (Table 7). Three studies were identified for the otolaryngologic surgery model.32-34 All compared a selective COX-2 inhibitor with acetaminophen or placebo. All 3 studies found that the selective COX-2 inhibitor or the combination of a COX-2 with acetaminophen demonstrated significantly lower pain scores compared with acetaminophen or placebo (P < .05). Joshi et al,33 in a study of pediatric patients undergoing tonsillectomy, found that postoperative pain scores were significantly lower in the rofecoxib www.aana.com/members/journal/ group at 2 and 24 hours. Nausea and vomiting also were decreased in the rofecoxib group compared with the placebo group.33 Effects on platelet function Three studies were identified that specifically addressed the effects of selective COX-2 inhibitors on platelet function.35-37 All studies compared the effects of a supratherapeutic dose of a selective COX-2 agent with standard doses of nonselective NSAIDs and placebo in adult volunteers. All 3 studies examined platelet aggregation responses, bleeding time, and serum thromboxane B2 concentrations. All studies found that the specific COX-2 inhibitors had no effects on platelet function, whereas the nonselective NSAIDs significantly increased bleeding time and reduced platelet function and thromboxane B2 levels. It was determined that the selective COX-2 inhibitors spared COX-1 function and, therefore, did not interfere with normal mechanisms of platelet aggregation and hemostasis. Hegi et al38 specifically compared rofecoxib and diclofenac and their effects on platelet aggregation and surgical blood loss in patients undergoing vaginal hysterectomy or breast surgery. Rofecoxib showed less platelet disturbance, intraoperative blood loss, and hemoglobin decrease than did diclofenac. The study did not determine the effects of rofecoxib compared with placebo. Five studies identified for the efficacy portion of this review mentioned surgical blood loss as a secondary outcome measured.14,16,19,22,25 All 5 studies found no difference in surgical blood loss when a COX-2 inhibitor was compared with opioid or placebo. Effects on renal function Four studies were identified that examined the effects of selective COX-2 inhibition on renal function.39-42 Rossat et al39 examined the renal effects of celecoxib and naproxen in salt-depleted normotensive subjects. The results indicated that although celecoxib had no effects on systemic blood pressure, transient decreases in renal blood flow and glomerular filtration rate (GFR) were noted. Decreased urine output and sodium and potassium retention also were noted with repeated administration.39 Swan et al40 examined the effects of rofecoxib on renal function in elderly patients on a low sodium diet. The renal perfusion effects of rofecoxib and indomethacin were compared with placebo. The GFR was similarly decreased by rofecoxib and indomethacin after a single dose and after multiple doses. It was determined that the effects of COX-2 inhibition on renal function are similar to the effects of nonselective NSAIDs and www.aana.com/members/journal/ that COX-2 might have an important homeostatic role in the maintenance of renal perfusion.40 Schwartz and Vandormael41 studied renal effects of rofecoxib, celecoxib, and naproxen in elderly patients on a normal-salt diet. Renal function was measured by urinary sodium excretion, systolic and diastolic blood pressure, creatinine clearance, and body weight. It was found that influence on renal function did not differ between selective COX-2 inhibitors and nonselective NSAIDs.41 Whelton et al42 examined the renal effects of celecoxib and naproxen in elderly subjects. After an initial dose, naproxen produced a greater reduction in GFR. On day 6 of the 10-day study, the treatment difference became statistically significant. It was noted on day 6 that the reduction in GFR was –7.53 mL/min/1.73m2 for naproxen and –1.11 mL/min/1.73m2 for celecoxib. Although both agents reduced GFR, the reduction was significantly greater for naproxen.42 Summary New insight into the physiology and management of acute postoperative pain calls for the incorporation of multimodal analgesia. It has been demonstrated in the literature across multiple pain models that COX2 inhibitors are safe and effective agents in the treatment of postsurgical pain in a carefully selected patient population. Current literature suggests that selective COX-2 inhibitors reduce postoperative opioid use, reduce the complications associated with opioids, and increase patient satisfaction. Furthermore, selective COX-2 inhibition seems to have no effect on platelet function in healthy subjects. Although not all of the efficacy studies examined perioperative blood loss, several examined bleeding as an outcome. None of those studies demonstrated any increase in surgical bleeding with the use of selective COX-2 inhibitors. Further investigation into the perioperative platelet effects of COX-2 inhibition and the specific effects on surgical bleeding is warranted. Cyclooxygenase-2 has an important homeostatic role in renal function. Renal function seems to be decreased to some degree, most notably GFR, by selective COX-2 inhibitors; the effect on renal function is similar to that caused by nonselective NSAIDs. The data indicate that COX-2 inhibitors should be used cautiously in patients with preexisting renal and cardiac disease. More studies are needed examining the renal effects of selective COX-2 agents in the perioperative setting to further investigate their effect on surgical patients. In light of recent controversy surrounding the use of AANA Journal/February 2006/Vol. 74, No. 1 57 58 AANA Journal/February 2006/Vol. 74, No. 1 www.aana.com/members/journal/ Parcoxib, 20 or 40 mg 1 preoperative IV or IM; ketorolac, 60 mg IM; placebo Parecoxib comparable to ketorolac in onset but had longer duration Analgesic efficacy of parecoxib, 20 mg to 100 mg similar to ketorolac, 30 mg; parecoxib, 50 and 100 mg had significantly longer duration than ketorolac Effects, onset, and peak analgesic effect not significantly different from ibuprofen Peak pain score significantly lower in rofecoxib group NA All groups significant to 24 h Quality of pain control NS Significant NA NA NA Significant, all groups NA NA NA NA Significant NA Other Parecoxib had longer duration than ketorolac Parexocib doses <20 mg had suboptimal analgesic activity compared with placebo and ketorolac Rofecoxib demonstrated longer duration than ibuprofen Significantly more patients in codeine-acetaminophen group reported nausea/ vomiting Valdecoxib, 40 mg showed greater analgesic duration than 20 mg; both doses of valdecoxib showed significantly longer duration than oxycodoneacetaminophen All groups receiving valdecoxib reported significant increase in patient satisfaction in a dose-dependent manner Median time Rescue medication: to first rescue Total dose reduction * PO indicates by mouth; IV, intravenous; NA, not applicable; and NS, not significant. Significant values were P ≤ .05 in favor of the cyclooxygenase-2 inhibitor. Extraction, third molar Daniels et al31 (n = 304) 1 postoperative dose Parecoxib, 1, 2, 5, 10, 1 postoperative 20, 50, or 100 mg IV; ketorolac 30 mg IV; placebo Rofecoxib, 50 mg PO; codeine, 60 mg – acetaminophen, 600 mg PO Mehlisch et al30 Extraction, (n = 453) third molar Extraction, third molar Chang and Frick28 (n = 393) Valdecoxib, 20 1 postoperative or 40 mg PO; oxycodone, 10 mg – acetaminophen, 1,000 mg PO; acetaminophen, 1,000 mg PO; placebo 1 preoperative Rofecoxib, 50 mg PO; 1 postoperative ibuprofen, 400 mg PO; placebo Extraction, third molar Daniels et al27 (n = 406) Valdecoxib, 10, 20, 40, or 80 mg PO; placebo Analgesic agents and doses Dose timing Morrison et al29 Dental (n = 151) surgery Extraction, impacted third molar Type of surgery Desjardins et al15 (n = 284) Reference Table 6. Oral surgery pain model* NA Significant REFERENCES * PO indicates by mouth; NA, not applicable; and NS, not significant. Significant values were P ≤ .05 in favor of the cyclooxygenase-2 inhibitor. Significant Visual analog scale scores and intraoperative and postoperative opioid requirements significantly smaller in rofecoxib group Rofecoxib, 50 mg PO; placebo Otolaryngologic surgery Turan et al34 (n = 60) 1 preoperative Decreased nausea/ vomiting with rofecoxib NA Rofecoxib, 1 mg/kg PO; placebo Joshi et al33 Pediatric (n = 66) tonsillectomy 1 preoperative Significant difference in pain scale ratings at 2 and 24 h postoperatively NA Patient satisfaction greater in celecoxib + acetaminophen group vs placebo NS NS Maximum pain scores lower in celecoxib + acetaminophen group Celecoxib, 200 mg 1 preoperative PO; acetaminophen, 2,000 mg PO; celecoxib, 200 mg + acetaminophen, 2,000 mg PO; placebo Outpatient Issioui et al32 (n = 112) Other Rescue medication: Total dose reduction Median time to first rescue Quality of pain relief Analgesic agents and doses Dose timing Type of surgery Reference Table 7. Otolaryngologic surgery model* www.aana.com/members/journal/ all NSAIDs, intensive research into the use of NSAIDs in specific patient populations is warranted. The cardiovascular issues surrounding the NSAIDs as a class warrant specific randomized, controlled, prospective studies in healthy patients to determine in which patient populations NSAIDs can be used safely. This review suggests that selective COX-2 inhibitors can be used successfully as part of a multimodal treatment strategy for perioperative pain in carefully selected patients. 1. Food and Drug Administration Website. COX-2 selective and nonselective non-steroidal anti-inflammatory drugs (NSAIDS). Available at: www.fda.gov/cder/drug/infopage/COX2/default.htm. Accessed June 9, 2005. 2. NIH News. National Institutes of Health Website. Available at: www.nih.gov/news/pr/dec2004/od-17Q&A.htm. Accessed June 9, 2005. 3. Sinatra R. Role of COX-2 inhibitors in the evolution of acute pain management. J Pain Symptom Manage. 2002;24(suppl):S18-S27. 4. Morgan GE, Mikhail MS, Murray MJ, eds. Clinical Anesthesiology. New York, NY: Lange Medical Books/McGraw-Hill; 2002:309-358. 5. Flower RJ. Drugs which inhibit prostaglandin biosynthesis. Pharmacol Rev. 1974;26:33-67. 6. Vane JR, Botting RM. Mechanism of action of nonsteroidal antiinflammatory drugs. Am J Med. 1998;104:2S-8S. 7. Vane JR. Inhibition of prostaglandin synthesis as a mechanism of action for aspirin-like drugs. Nature. 1971;231:232-235. 8. Fu J-Y, Masferrer JL, Seibert K, Raz A, Needleman P. The induction and suppression of prostaglandin H2 synthase (cyclooxygenase) in human monocytes. J Biol Chem. 1990;265:16737-16740. 9. Masferrer JL, Zweifel BS, Seibert K, Needleman P. Selective regulation of cellular cyclooxygenase by dexamethasone and endotoxin in mice. J Clin Invest. 1990;86:1375-1379. 10. Xie W, Chipman JG, Robertson DL, Erikson RL, Simmons DL. Expression of a mitogen-responsive gene encoding prostaglandin synthase is regulated by mRNA splicing. Proc Natl Acad Sci U S A. 1991;88:2692-2696. 11. O’Banion MK, Sadowski HB, Winn V, Young DA. A serum- and glucocorticoid-regulated 4-kilobase mRNA encodes a cyclooxygenase-related protein. J Biol Chem. 1991;266:23261-23267. 12. Fitzgerald GA, Patrono C. The coxibs, selective inhibitors of cyclooxygenase-2. N Engl J Med. 2001;345:433-442. 13. World Health Organization. WHO Guidelines: Cancer Pain Relief. 2nd ed. Geneva, Switzerland: World Health Organization; 1996. 14. Reuben SS, Connelly NR. Postoperative analgesic effects of celecoxib or rofecoxib after spinal fusion surgery. Anesth Analg. 2000;91:1221-1225. 15. Desjardins PJ, Shu VS, Recker DP, Verburg KM, Woolf CJ. A single preoperative oral dose of valdecoxib, a new cyclooxygenase-2 specific inhibitor, relieves post-oral surgery or bunionectomy pain. Anesthesiology. 2002;97:565-573. 16. Reynolds LW, Hoo RK. The COX-2 specific inhibitor, valdecoxib, is an effective, opioid-sparing analgesic in patients undergoing total knee arthroplasty. J Pain Symptom Manage. 2003;25:133-141. 17. Bekker A, Cooper PR, Frempong-Boadu A, Babu R, Errico T, Lebovits A. Evaluation of preoperative administration of the cyclooxygenase-2 inhibitor rofecoxib for the treatment of postoperative pain after lumbar disc surgery. Neurosurgery. 2002;50:1053-1057. 18. Camu F, Beecher T, Recker DP, Verburg KM. Valdecoxib, a COX2-specific inhibitor, is an efficacious opioid-sparing analgesic in patients undergoing hip arthroplasty. Am J Ther. 2002;9:43-51. AANA Journal/February 2006/Vol. 74, No. 1 59 19. Malan TP Jr, Marsh G, Hakki SI, Grossman E, Traylor L, Hubbard RC. Parecoxib sodium, a parenteral cyclooxygenase 2 selective inhibitor, improves morphine analgesia and is opioid-sparing following total hip arthroplasty. Anesthesiology. 2003;98:950-956. 20. Hubbard RC, Naumann RM, Traylor L, Dhadda S. Parecoxib sodium has opioid-sparing effects in patients undergoing total knee arthroplasty under spinal anesthesia. Br J Anaesth. 2003;90:166-172. 21. Rasmussen GL, Steckner K, Hogue C, Torri S, Hubbard RC. Intravenous parecoxib sodium for acute pain after orthopedic knee surgery. Am J Orthop. 2002;31:336-343. 22. Buvanendran A, Kroin JS. Effects of perioperative administration of a selective cyclooxygenase 2 inhibitor on pain management and recovery of function after knee replacement: a randomized controlled trial. JAMA. 2003;290:2411-2418. 23. Tang J, Li S, White PF, et al. Effect of parecoxib, a novel intravenous cyclooxygenase type-2 inhibitor, on the postoperative opioid requirement and quality of pain control. Anesthesiology. 2002;96:1305-1309. 24. Barton SF, Langeland FF, Snabes MC, et al. Efficacy and safety of intravenous parecoxib sodium in relieving acute postoperative pain following gynecologic laparotomy surgery. Anesthesiology. 2002;97:306-314. 25. Sinatra RS, Shen QJ, Halaszynski T, Luther MA, Shaheen Y. Preoperative rofecoxib oral suspension as an analgesic adjunct after lower abdominal surgery: the effects on effort-dependent pain and pulmonary function. Anesth Analg. 2004;98:135-140. 31. Daniels SE, Grossman EH, Kuss ME, Talwalker S, Hubbard RC. A double-blind, randomized comparison of intramuscularly and intravenously administered parecoxib sodium versus ketorolac and placebo in a post–oral surgery model. Clin Ther. 2001;23:10181031. 32. Issioui T, Klein KW, White PF, et al. The efficacy of premedication with celecoxib and acetaminophen in preventing pain after otolaryngologic surgery. Anesth Analg. 2002;94:1188-1193. 33. Joshi W, Connelly NR, Reuben SS, Wolckenhaar M, Thakkar N. An evaluation of the efficacy and safety of administering rofecoxib for postoperative pain management. Anesth Analg. 2003;97:35-38. 34. Turan A, Emet S, Karamanlioglu B, Memis D, Turan N, Pamucku Z. Analgesic effects of rofecoxib in ear-nose-throat surgery. Anesth Analg. 2002;95:1308-1311. 35. Leese PT, Talwalker S, Kent JD, Recker DP. Valdecoxib does not impair platelet function. Am J Emerg Med. 2002;20:275-281. 36. Leese PT, Recker DP, Kent JD. The COX-2 selective inhibitor, valdecoxib, does not impair platelet function in the elderly: results of a randomized controlled trial. J Clin Pharmacol. 2003;43:504-513. 37. Leese PT, Hubbard RC, Karim A, Isakson PC, Yu SS, Geis GS. Effects of celecoxib, a novel cyclooxygenase-2 inhibitor, on platelet function in healthy adults: a randomized, controlled trial. J Clin Pharmacol. 2000;40:124-132. 38. Hegi TR, Bombeli T, Seifert B, et al. Effect of rofecoxib on platelet aggregation and blood loss in gynaecological and breast surgery compared with diclofenac. Br J Anaesth. 2004;92:523-531. 26. Joshi GP, Viscusi ER, Gan TJ, et al. Effective treatment of laparoscopic cholecystectomy pain with intravenous followed by oral COX-2 specific inhibitor. Anesth Analg. 2004;98:336-342. 39. Rossat J, Maillard M, Nussberger J, Brunner HR, Burnier M. Renal effects of selective cyclooxygenase-2 inhibition in normotensive salt-depleted subjects. Clin Pharmacol Ther. 1999;66:76-84. 27. Daniels SE, Desjardins PJ, Talwalker S, Recker DP, Verburg KM. The analgesic efficacy of valdecoxib vs. oxycodone/acetaminophen after oral surgery. J Am Dent Assoc. 2002;133:611-621. 40. Swan SK, Rudy DW, Lasseter KC, et al. Effect of cyclooxygenase-2 inhibition on renal function in elderly persons receiving a low-salt diet. Ann Intern Med. 2000;133:1-9. 28. Chang DJ, Frick GR. Rofecoxib versus codeine/acetaminophen in postoperative dental pain: a double-blind, randomized, placebo- and active comparator–controlled clinical trial. Clin Ther. 2001;23:1446-1455. 41. Schwartz JI, Vandormael K. Comparison of rofecoxib, celecoxib, and naproxen on renal function in elderly subjects receiving a normal-salt diet. Clin Pharmacol Ther. 2002;72:50-61. 29. Morrisson BW, Christensen S, Yuan W, Brown J, Amlani S, Seidenberg B. Analgesic efficacy of the cyclooxygenase-2-specific inhibitor rofecoxib in post-dental surgery pain: a randomized, controlled trial. Clin Ther. 1999;21:943-953. 30. Mehlisch DR, Desjardins PJ, Daniels S, Hubbard RC. Single doses of parecoxib sodium intravenously are as effective as ketorolac in reducing pain after oral surgery. J Oral Maxillofac Surgery. 2003;61:1030-1037. 60 AANA Journal/February 2006/Vol. 74, No. 1 42. Whelton A, Schulman G, Wallemark C, et al. Effects of celecoxib and naproxen on renal function in the elderly. Arch Intern Med. 2000;160:1465-1470. AUTHOR Melissa Holmes Zemmel, CRNA, MSNA, is a nurse anesthetist at Baptist Hospital of Miami, Miami, Fla. She was a student at Virginia Commonwealth University, Richmond, Va, at the time this article was written. Email: [email protected] www.aana.com/members/journal/