Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
ASNR 2012
ASNR 2012
Imaging Genomics: Correlation of Invasive
Genomic Composition and Patient Survival
Using Qualitative and Quantitative MR Imaging
Parameters
RR Colen1, B Mahajan1, A Flanders2, E Huang3, R Jain4, D Gutman5, S Hwang5, J Kirby6,
J Freyman6, TCGA Glioma Phenotype Research Group, , F Jolesz1, PO Zinn2
1
Brigham and Women's Hospital, Boston, MA, USA.
2 Thomas Jefferson University Hospital, Philadelphia, PA, USA.
3 National Cancer Institute, Bethesda, MD, USA.
4 Henry Ford, Detroit, MI, USA.
5 Emory University, Atlanta, GA, USA.
6 SAIC-Frederick, Bethesda, MD, USA.
7 M.D. Anderson Cancer Center, Houston, TX, USA.
© NlH National Center for Image Guided Therapy, 2012
ASNR 2012
Disclosure
No Disclosures.
R25 CA089017(RRC)
P41 RR019703 (FAJ)
© NlH National Center for Image Guided Therapy, 2012
ASNR 2012
Introduction
Microarray technology is a novel method that allows for the simultaneous
analysis of whole genome gene- and microRNA expression events.
However, despite the discovery of many new molecular targets and pathways
that has resulted from these discoveries, the search for an effective therapy
continues.
In order for personalized medicine to transpire, a cost-effective biomarker that
accurately reflects underlying molecular cancer compositions is urgently
needed.
© NlH National Center for Image Guided Therapy, 2012
ASNR 2012
Introduction
•
Large scale gene- and microRNA based cancer characterization is commonly
not performed due to high cost, time and manpower required for data
analysis and interpretation.
•
Imaging, specifically MRI, is a promising biomarker that can reflect underlying
tumor pathology and biological function.
•
It can evaluate the entire tumor, including its peritumoral regions which
harbor microscopic invasion of cancer cells, the major cause for tumor
recurrence.
•
It follows that if imaging phenotypes can serve as non-invasive surrogates for
cancer genomic events, MRI can provide important information as to the
diagnosis, prognosis, and optimal treatment based on personalized genomic
based medicine.
© NlH National Center for Image Guided Therapy, 2012
ASNR 2012
Imaging genomics
• Imaging genomics has emerged as a new field which links the specific
imaging traits (radiophenotypes) with gene-expression profiles.
• Advantages of Imaging genomics:
• It is non-invasive.
• Specific imaging traits(radiophenotypes) can be correlated with geneexpression profiles
• MRI biomarkers can be developed from the conventional and advanced
imaging sequences/techniques.
• MRI biomarker signatures can be created based on tumor biology
- Invasion (Flair + Peritumoral perfusion)
- Tumor growth (CE + necrosis)
- Tumor aggressiveness (Invasion + growth)
© NlH National Center for Image Guided Therapy, 2012
ASNR 2012
Purpose
•
In this presentation, we wish to describe and identify the invasive MRI
characteristics in GBM and the implicated genes and microRNAs
associated with these invasive features.
•
To document the pre-operative qualitative imaging data reflective of
invasive tumor growth patterns.
© NlH National Center for Image Guided Therapy, 2012
ASNR 2012
Methods and Materials
• Retrospective study of 78 treatment naïve GBM patients, whom had
both gene- and microRNA expression profiles and pretreatment MRneuroimaging.
•
Image data were obtained from The Cancer Imaging Archive(TCGA)
{http://cancerimagingarchive.net/} sponsored by the Cancer Imaging
Program, DCTD/NCI/NIH.
© NlH National Center for Image Guided Therapy, 2012
ASNR 2012
Methods and Materials
Discovery and Validation sets
•To increase the robustness and validity of the analysis, the 78 patients
were randomly separated into a discovery and validation set each
consisting of 39 patients.
•By using the FLAIR signal volume as criteria for further subgrouping the
patients, each set was sub-stratified into high, medium, and low FLAIR
volumes (each consisting of 13 patients) corresponding to volumes of
high, medium, and low peritumoral edema/invasion, respectively.
© NlH National Center for Image Guided Therapy, 2012
ASNR 2012
Methods and Materials
Discovery (N = 26) and validation (N = 26) sets.
© NlH National Center for Image Guided Therapy, 2012
ASNR 2012
Methods and Materials
•
Image Analysis - Qualitative assessment
VASARI feature set criteria was used for visual assessment of key
features of invasion:
- presence of either T1 contrast enhancement of increase
T2/FLAIR hyperintensity involving the basal ganglia, corpus
callosum (unilateral, bilateral, or contralateral) or brainstem
- presence of subependymal enhancement
- presence of pial enhancement
- presence of peritumoral nonenhancing FLAIR hyperintensity.
© NlH National Center for Image Guided Therapy, 2012
ASNR 2012
Methods and Materials
•
Image Analysis - Quantitative assessment
- Slicer 3.6 (slicer.org) - Segmentation module
The 3D Slicer software 3.6 (http://www.slicer.org) was used for all
purposes of image analysis, manipulation and segmentation.
3D Slicer is an open-source software platform developed at our institution
(BWH/Harvard Medical School) for medical image processing and 3D
visualization of image data.
- Slicer platform provides functionality for segmentation, registration and 3D
visualization of imaging data and advanced MRI analysis algorithms.
© NlH National Center for Image Guided Therapy, 2012
ASNR 2012
Methods and Materials
•
Image Analysis - Quantitative assessment
-
T2/FLAIR was registered to the post- contrast
T1WI.
-
Volumetric segmentation was performed in a simple
hierarchical model of anatomy, proceeding from
peripheral to central.
- 3 distinct structures were segmented:
•
edema/invasion
• enhancing tumor
• necrosis
© NlH National Center for Image Guided Therapy, 2012
ASNR 2012
Methods and Materials
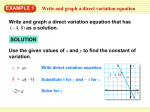
A 55 year old male patient with a right
temporal GBM.
(a) Axial FLAIR image demonstrates
segmentation (in blue) of the region of
FLAIR hyperintensity corresponding to
the area of edema/tumor infiltration.
(b) The segmented edema/tumor
infiltration (blue), enhancement (yellow)
and necrosis (orange) are seen overlaid
on a base post- contrast T1WI.
(c) Axial post-contrast enhanced T1WI
demonstrates the segmentation of the
enhancement (yellow) and necrosis
(orange).
© NlH National Center for Image Guided Therapy, 2012
ASNR 2012
Methods and Materials
Models of edema, tumor and necrosis were generated from the previously
performed segmentations, and the volumes of the same were
automatically calculated.
Volumes of each radiophenotype ( edema/tumor infiltration, enhancing
tumor, and necrosis) were then correlated with the genomic findings.
© NlH National Center for Image Guided Therapy, 2012
ASNR 2012
Methods and Materials
• Biostatistical Image-Genomic Analysis: A total of 12,764 genes and 555
microRNAs were analyzed (Affymetrix/Agilent chip technology) in each
patient.
•
Comparative Marker Selection (Broad Institute) identified preferentially
up-regulated genomic events in one vs. another predefined patient
group (high_low).
•
Ingenuity pathway analysis (IPA) Analysis provided insight into
molecular-cellular-disease
© NlH National Center for Image Guided Therapy, 2012
ASNR 2012
Results
High FLAIR Radiophenotype
© NlH National Center for Image Guided Therapy, 2012
ASNR 2012
Results
Low FLAIR Radiophenotype
© NlH National Center for Image Guided Therapy, 2012
ASNR 2012
Results
• Our MRI screen on an invasive MRI radiophenotype identified genes and microRNAs associated
with tumor invasion.
• Bioinformatically predicted gene-microRNA regulatory networks in high FLAIR signal GBMs were
seen.
© NlH National Center for Image Guided Therapy, 2012
ASNR 2012
Results
•
Kaplan Meier Analysis demonstrated the top upregulated gene, POSTN
(known to be associated with invasion and mesenchymal change), to
stratify patients into good (low POSTN) and poor (high POSTN) survival
groups.
Kaplan Meier curves for Periostin.
(a) Days to death
(b) Progression free survival.
© NlH National Center for Image Guided Therapy, 2012
ASNR 2012
Results
d)
e)
(c) Periostin expression levels across the two main GBM subtypes, Mesenchymal and Proneural
showed an increase in POSTN expression in the mesenchymal group and (d) shows the concordant
inverse expression levels of miR-219 across the Mesenchymal and Proneural subtypes. (e) Note the
inverse correlation (Rsq=0.204) with Periostin.
© NlH National Center for Image Guided Therapy, 2012
ASNR 2012
Results
Qualitative analysis using the Vasari featureset
Two qualitative invasive features were statistically significant in this patient population: 1)
Ependymal enhancement and 2) enhancement across the midline.
Ependymal Enhancement. Those patients with ependymal enhancement had a worse
prognosis than those without ( p= 0.0044). This was further a better predictor of survival than
age (p=0.4606), a currently used clinical demographic to stratify GBM patient prognosis.
Kaplan Meier Survival Curve
© NlH National Center for Image Guided Therapy, 2012
ASNR 2012
Results
Qualitative analysis using the Vasari featureset
Two qualitative invasive features were statistically significant in this patient population: 1)
Ependymal enhancement and 2) enhancement across the midline.
Enhancement across the midline. Those patients with enhancement across the midline had a
worse prognosis than those without ( p= 0.0087). This was further a better predictor of survival
than age(p=0.2298), a currently used clinical demographic to stratify GBM patient prognosis.
Kaplan Meier Survival Curve
© NlH National Center for Image Guided Therapy, 2012
ASNR 2012
Conclusion
•
Invasive features of Glioblastoma can be determined by both qualitative and
quantitative assessment of MR imaging parameters.
•
Imaging genomics reflect tumor compositions which have genes involved in:
- tumor invasion
- differences in patient survival
•
Invasive MR imaging features and phenotypes can serve as biomarkers to help
predict tumor genomic composition and patient survival
© NlH National Center for Image Guided Therapy, 2012
ASNR 2012
Conclusion
Thank you for your interest!
Acknowledgements: This work was supported by NIH grant R25
CA089017-06A2 (RRC).
Any questions please email: [email protected].
© NlH National Center for Image Guided Therapy, 2012