Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Location and Stability of Rectus Muscle Pulleys
Muscle Paths as a Function of Gaze
Robert A. Clark* Joel M. Miller,^ and Joseph L. Demer*%
Purpose. The paths of the rectus extraocular muscles (EOMs) are constrained by pulleys,
connective tissue sleeves mechanically coupled to the orbital walls. This study sought to
investigate, using high-resolution magnetic resonance imaging (MRI), the location and stability of EOM pulleys in normal subjects and those with strabismus.
Methods. Multiple contiguous coronal MRI scans spanning the anterior-to-posterior extent of
the orbit during primary gaze, upgaze, downgaze, adduction, and abduction were analyzed
digitally to determine the paths of the rectus EOMs. Pulley locations were inferred from EOM
paths.
Results. Data for 10 orbits of six normal subjects established the normal paths of the rectus
extraocular muscles in primary gaze. Muscle paths in primary position were highly uniform
across normal subjects. In secondary gaze positions, rectus muscle paths at the level of the
pulleys exhibited small but consistent shifts, relative to the orbit, opposite the direction of
gaze, consistent with the expected mechanical effects of the intermuscular connective tissue
suspensions of the pulleys. Twelve orbits of seven subjects with strabismus showed, as a group,
no significant difference from normal in rectus muscle paths in primary gaze and no significant
difference from normal in changes of muscle paths in secondary gaze. Two subjects with
incomitant strabismus were found to have grossly abnormal rectus muscle paths in primary
gaze, suggesting heterotopic pulleys. Computer simulations of these heterotopic pulley locations accounted for the observed patterns of incomitant strabismus in both.
Conclusions. High-resolution MRI can determine the location and sideslip of rectus EOM
pulleys. Pulley position is highly uniform across normal subjects, consistent with the notion
that musculo-orbital tissue connections determine the pulling direction of the rectus EOMs.
In normal subjects and subjects with strabismus, pulleys exhibit small shifts with eccentric
gaze that are consistent with secondary intermuscular, but not musculo-global, mechanical
couplings. Heterotopic pulley position is a potential cause of incomitant strabismus. Invest
Ophthalmol Vis Sci. 1997;38:227-240.
XVecent studies exploiting high-resolution magnetic
resonance imaging (MRI) of rectus extraocular muscles (EOMs) have facilitated a new understanding of
EOM paths and their behavior during changes in gaze.
Historically, the concept of rectus EOM behavior has
evolved from the "shortest path" hypothesis,1 by
which the muscle belly was thought to have complete
From the Departments of * Ophthalmology and %Neurology, University of California,
Los Angeles, and the f Smith-Kettlewell Eye Research Institute, San Francisco,
California,
Supported by National Eye Institute consortium grant EY08313 (JIJ), JMM), core
grant EY00331 to the Department of Ophthalmology at the University of California,
Los Angeles, and core giant EY06883 to Smith-Kettlewell Eye Research Institute.
Submitted for publication May 6, .1996; revised August 1, 1996; accepted September
5, 1996.
Proprietary interest categmy: A'.
Reprint requests: Josejjh L. Demet; Jules Stein Eye Institute, University of California,
100 Stein Plaza, Los Angeles, CA 90095-7002.
Investigative Ophthalmology & Visual Science, January 1997, Vol. 38, No. 1
Copyright © Association for Research in Vision and Ophthalmology
freedom to slip to the path of least tension, to the
"permitted sideslip" hypothesis, by which unspecified
constraints2 or musculo-global elasticities3'4 were proposed to allow only limited muscle path displacement
during gaze shifts.
The most recent evidence demonstrates that paths
of the rectus EOM bellies are tightly constrained in
the orbit during changes in gaze except, of course,
for their most anterior, tendinous insertions.5"7 Rectus
EOMs are now known to pass through connective tissue sleeves—composed of collagen, elastin, and
smooth muscle—that function as pulleys.89 Serial histologic sectioning has demonstrated that these pulleys
are coupled mechanically to the orbital walls, directly
and indirectly, by intermuscular couplings in posterior
Tenon's fascia.9 The pulleys serve as the effective me227
228
TABLE
Investigative Ophthalmology & Visual Science, January 1997, Vol. 38, No. 1
l. Clinical Profiles of Subjects With Strabismus
Subject
Age
(years)
Sex
Primary Deviation
Incomitance
Prior Strabismus Surgery
CB
SB
29
58
F
M
Right hypertropia 3°
Right hypertropia 2°
Greater in left gaze
Greater in downgaze
AC
TL
50
30
M
M
"A" pattern
"A" pattern
RM
36
M
Esotropia 15°
Exotropia 3°,
right hypertropia 5°
Exotropia 7°
None
Right inferior rectus recession
(unknown amount)
None
Bilateral superior oblique tenotomies
JM
60
M
CP
28
F
Left hypertropia 8°,
exotropia 3°
Left hypertropia 5°
Greater in right gaze,
"V" pattern exotropia
Greater in downgaze
"A" pattern
chanical origins of the EOMs, exerting a profound
influence on EOM behavior. This effect is seen most
clearly after muscle transposition surgery, in which
pulleys markedly limit the path displacement of transposed muscles.6'7 Pulley ultrastructure is specialized
for high internal rigidity, capable of resisting displacement during rectus muscle contraction,10 and the pulleys are suspended by connective tissue containing
richly innervated smooth muscle bands.11 Computer
simulation of orbital mechanics shows that binocular
alignment is highly sensitive to pulley location." However, the early MRI studies of muscle paths were performed on small numbers of subjects using scanning
techniques that have now been considerably improved. Quantitative normative data on human pulley
locations are lacking.
These observations suggest that abnormal pulley
sideslip or abnormal pulley position might cause or
contribute to incomitant strabismus. For example, a
V-pattern strabismus could result from a lateral rectus
muscle pulley inferiorly displaced or a medial rectus
muscle pulley superiorly displaced in the orbit. As another example, weakened pulleys could result in excess rectus muscle sideslip during changes in gaze,
leading to incomitant strabismus caused by asymmetrical shifts in muscle positions and elastic tensions.
Histologic evidence indicates that the posterior
orbital paths of the EOMs are determined entirely by
their origins at the annulus of Zinn and by the locations of the pulleys near the equator of the globe.9
No other tissues exist that could influence posterior
muscle paths significandy.9 Thus, despite the inability
of MRI to image the pulleys directly in most cases,9
the paths of the EOMs that are so obvious on MRI
imaging must lead direcdy to the pulleys, whose anteroposterior location is known from the histology to
lie at and just posterior to the equator of the globe
in primary gaze.9 The current study was designed to
examine EOM paths to infer in this manner the location and sideslip of the fibromuscular pulleys during
gaze shifts in normal patients. These findings were
used to evaluate the position and sideslip of die fi-
Bilateral medical rectus recessions
(unknown amount)
None
None
bromuscular pulleys in patients with known incomitant strabismus.
METHODS
Six normal volunteers were recruited by advertisement
and were examined to verify normal ocular motility
and the absence of strabismus. From patients enrolled
in an ongoing clinical study, we selected seven subjects
with incomitant strabismus (Table 1). Four of the
seven subjects with strabismus had incomitant hypertropia, as measured with a Hess screen. One of the
subjects with hypertropia also had a V-pattern strabismus, consisting of an exodeviation (divergence) in
upgaze that shifted gradually to an esodeviation (convergence) in downgaze. An A-pattern strabismus is a
horizontal strabismus with greater divergence or less
convergence in downgaze. One subject had A-pattern
esotropia, and the remaining two subjects had A-pattern exotropias. Qualitative data on subject TL have
been briefly presented elsewhere.12 Three of the seven
subjects with strabismus underwent strabismus surgery
before analysis (Table 1).
After obtaining informed, written consent according to a protocol conforming to the Declaration
of Helsinki and approved by the Human Subject Protection Committee at the University of California, Los
Angeles, all patients underwent high-resolution MRI
using a superconducting 1.5 T General Electric Signa
(Milwaukee, WI) or Picker Vista (Cleveland, OH)
scanner following techniques described in detail elsewhere.5'6 Briefly, subjects' heads were stabilized using
foam cushions and tape. A surface coil was placed over
the scanned orbit, and multiple contiguous coronal
images 3 mm in thickness were obtained with a 256
X 192 or 256 X 256 matrix over a 10 cm square field
of view, giving a pixel resolution of 390 (m\. A fixation
target for primary position was attached to the inside
of the scanner magnet, and other targets were used
to maintain secondary gaze positions. The position of
the globe-optic nerve junction in acquired images
was used to determine the actual amount of globe
Location and Stability of Rectus Muscle Pulleys
229
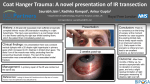
FIGURE l. Coronal magnetic resonance images of a normal right orbit for plane 0 in primary
and secondary gaze positions. The transverse diagram (bottom (eft) demonstrates the movement of the globe-optic nen'e junction from point C in abduction to point D in adduction,
allowing calculation of the total angle of rotation of the globe with change in horizontal
gaze position. Similarly, the sagittal diagram (bottom right) demonstrates the movement of
the globe-optic nerve junction from point A in upgaze to point B in downgaze, allowing
calculation of the total angle of rotation with change in vertical gaze. Muscle and orbital
borders have been outlined digitally in white. Video displays of computer images have
greater contrast and resolution than print images. SR = superior rectus muscle; LR = lateral
rectus muscle; IR = inferior rectus muscle; MR = medial rectus muscle.
rotation for positions of secondary gaze (Fig. 1). Images of primary gaze, upgaze, and downgaze were obtained for all patients, as were abduction and adduction for normal subjects.
Digital magnetic resonance images were transferred to Macintosh computers (Apple Computer, Cupertino, CA) and converted to 8-bit tagged image file
format using locally developed software and were analyzed quantitatively using the program NIH Image (W.
Rasband, National Institutes of Health; available by
ftp from zippy.nimh.nih.gov or on floppy disk from
NTIS, 5285 Port Royal Road, Springfield, VA 22161,
part number PB95-500195GEI). Images of left orbits
were reflected digitally to the orientation of a right
orbit to allow uniform analysis of EOM positions.
To assess the effects of gaze changes on orbital
anatomy, it was important to correct for small concomitant changes in head position. Normalization of image position and orientation facilitated quantitative
comparisons and summaries across subjects. The magnetic field coordinates of the MRI scanner served as
references for rotational corrections.
To normalize position in the coronal plane, all
rectus muscle positions were translated to place the
coordinate origin at the area centroid of the orbit.
We normalized rotation in the coronal plane by rotating the image to align the interhemispheric fissure of
the brain with the scanner-defined vertical meridian
(Fig. 2). This rotational correction ranged from 12°
clockwise to 8.5° counterclockwise. In anterior image
planes without a clear view of the interhemispheric
fissure of the brain, the angle in the coronal plane
Investigative Ophthalmology & Visual Science, January 1997, Vol. 38, No. 1
230
FIGURE 2. Coronal plane magnetic resonance imaging (MRI)
of a normal right orbit demonstrates the two rotational angle
corrections measured in each gaze position. The vertical correction was used to rotate all orbits to bring the interhemispheric
fissure of the brain to the vertical position (as defined by die
magnetic field coordinates of die MRI scanner). The horizontal
angle measured was used to maintain coronal rotational alignment of bony structures during changes of gaze in image planes
that lacked a distinct view of die interhemispheric fissure. Video
displays of computer images have greater contrast and resolution than print images. SR = superior rectus muscle; LR =
lateral rectus muscle; IR = inferior rectus muscle; MR = medial
rectus muscle; SO = superior oblique muscle.
formed by the center of the orbit, a fixed bony point,
and the scanner horizontal meridian was used as a
reference (Fig. 2).
The orbital roof angle is a measure of the sagittal
plane tilt (pitch) of the subject's head. The sagittal
FIGURE 3. Sagittal magnetic resonance imaging reconstruction
of a normal orbit in primary gaze, allowing identification of
the orbital roof angle. Video displays of computer images have
greater contrast and resolution dian print images. SR = superior
rectus muscle; IR = inferior rectus muscle.
plane orbital roof angle was measured by reformatting
the sequence of coronal images in to a single sagittal
image and measuring the angle between the orbital
roof and the scanner horizontal axis (Fig. 3). The
orbital roof angle varied less than 1° on average across
gaze angles.
TABLE 2. Position and Sideslip of Rectus Extraocular Muscles in Plane-1
(mm from orbital center)
Primary Gaze
Normal Subjects
X
Upgaze
Y
Medial rectus
12.1 ± 0.4
0.1 ±
Superior rectus -1.4 + 0.3
12.3 ±
Lateral rectus -11.7 + 0.3 -0.8 ±
Inferior reclus
1.7 + 0.6 -12.3 ±
Primary Gaze
Subjects With
Strabismus
X
X Change
0.7
0.5
0.4
0.5
Y Change
Abduction
Y Change X Change
Y Change
Adduction
X Change
Y Change
0.1 ± 0.3 0.3 ± 0.4 0.1 ± 0.3 -0.3 ± 0.2 0.4 ± 0.7 0.0 + 0.2 -0.3 ± 0.4 0.0 ± 0.2
1.0 ± 0.7 -1.6 ± 0.7 0.4 ± 0.6 1.0 + 0.9 0.2 ± 0.5 0.8 ± 0.4 0.4 ± 0.5 0.1 ± 0.4
0.0 ± 0.1 -0.7 ± 0.4 0.0 ± 0.2 0.8 ± 0.7 0.0 ± 0.4 1.0 ± 0.8 -0.5 ± 0.3 -0.5 ± 0.5
1.1 ± 0.3 -1.0 ± 0.3 -1.3 ± 0.3 1.3 ± 0.3 0.2 ± 0.3 -0.2 ± 0.1 -0.2 ± 0.5 -0.1 + 0.3
Upgaze
Y
Doumgaze
X Change
X Change
Y Change
Downgaze
X Change
Y Change
Medical rectus 12.2 ± 0.5 -0.8 ± 0.9 0.1 + 0.1 0.3 ± 0.4 0.2 ± 0.2 -0.2 ± 0.2
Superior rectus -1.4 ± 0.10 11.9 + 0.8 0.9 ± 1.0 -1.1 ± 0.8 0.6 ± 0.7 2.0 + 0.5
Lateral rectus -12.3 ± 0.4 -0.4 ± 1.6 -0.1 ± 0.2 -0.9 + 0.4 0.0 + 0.2 1.2 ± 0.3
Inferior rectus
1.5 ± 1.2 -12.5 ± 0.5 1.0 ± 0.3 -0.9 ± 0.4 -1.8 ± 0.7 1.8 ± 0.5
Location and Stability of Rectus Muscle Pulleys
231
FIGURE 4. Three contiguous
anterior coronal magnetic
resonance imaging planes of
a normal orbit in primary
position, demonstrating the
procedure for defining the
anteroposterior position of
the globe center with respect
to plane 0. Each image plane
is 3 mm thick. Video displays
of computer images have
greater contrast and resolution than print images.
Finally, to normalize the anteroposterior position,
the plane containing the globe-optic nerve junction
was designated plane 0. The center of the globe in
the sagittal plane was estimated with subpixel resolution by fitting a circle to three points on die globe
images in planes —2, —3, and —4 (Fig. 4). Globe centers, so determined, were within 0.4 mm for all patients and all gaze positions. Rotation of die line joining the center of the globe-optic nerve junction and
the globe center was used to estimate globe rotation in
secondary gaze positions (Fig. 1). Our reconstruction
methods assume minimal globe translation during
changes in gaze. Biomechanical simulation suggests
this to be a reasonable assumption because we calculate anteroposterior displacement to be less than 0.4
mm for up to 30° rotations of gaze in all directions.1314
Pulley locations were inferred, and binocular
alignment was simulated using the Orbit 1.5 Gaze Mechanics Simulation program (Orbit; Eidactics, San
Francisco, CA)13 running on Macintosh computers
(Apple Computer). Orbit simulates binocular alignment using static force balance equilibrium equations
based on orbital parameters, such as innervations,
globe dimensions, EOM insertions, lengths, stiffness,
pulley positions, and contractile forces. The program
Globe Center
then calculates the behavior of the EOMs and globes
based on equations and methods given, in part, in
Robinson,2 Miller and Robinson,3 and Miller and Demer." Pulley positions (based on histologic studies9)
in Orbit's description of a normal eye were taken as a
starting point. Then the lateral-medial and superiorinferior coordinates of Orbit's pulleys were altered to
match Orbit's simulated muscle paths to the paths observed in the MRI scans. To estimate anteroposterior
displacement of the globe during changes in gaze, a
translational compliance of 20 g/mm for small anteroposterior displacementH was used in Orbit simulations,
predicting a maximum anteroposterior shift in globe
position of 0.4 mm for 30° secondary gaze positions
in normal orbits. Translation might differ in subjects
with strabismus, but predicted translation can be computed in Orbit simulations.
RESULTS
We studied 10 orbits in six normal subjects and 12
orbits in seven subjects with strabismus. For all subjects, images were obtained for primary position, upgaze, and downgaze. Abduction and adduction images
were obtained in eight orbits of five normal subjects.
232
Investigative Ophthalmology & Visual Science, January 1997, Vol. 38, No. 1
FIGURE 5. Coronal magnetic
resonance images of the
right orbit of a normal subject in primary position. Image planes are numbered
posteriorly relative to image
plane 0 at the globe-optic
nerve junction. Video displays of computer images
have greater contrast and resolution than print images. SR
= superior rectus muscle;
MR = medial rectus muscle;
IR = inferior rectus muscle;
LR = lateral rectus muscle;
SO = superior oblique muscle; ON = optic nerve; LPS =
levator palpebrae superioris.
For each gaze position, six sequential planes were analyzed, beginning with plane —2 (6 mm anterior to the
globe-optic nerve junction) and extending posteriorly to plane 3 (9 mm posterior to the globe-optic
nerve junction) (Fig. 5). Plane —1 (3 mm anterior to
the globe-optic nerve junction) represents the most
anterior location at which muscle tendons were differentiated clearly from surrounding tissue. The average
position in primary gaze of the area centroids of normal and strabismic EOMs are shown in Figure 6 for
each of these image planes. Coordinates of the
centroids are tabulated in Table 2 for image plane — 1.
In no image plane was there a significant difference in
mean position of any rectus EOM between the normal
group and the group with strabismus (P < 0.05 using
the Bonferroni adjustment for multiple comparisons16). This finding indicates that rectus muscle paths
in the primary position are similar for normal subjects
and subjects with strabismus.
Normal subjects and subjects with strabismus aver-
233
Location and Stability of Rectus Muscle Pulleys
Plane -2
Plane -1
15 SR
5
SR
"
MR
MR
LR
-5
IR
IR
M-O-H
-15
E
1
&
•«5
6
.o
Plane 1
Plane 0
15 -
SR
SR
MR
LR
LR
-5 "
MR
w
o
a.
u—6—i
IR
IR
o
•E
Plane 2
FIGURE 6. Average positions
(relative to right orbital center and viewed as if facing the
subject) of centroids of the
rectus extraocular muscles
for primary gaze in all coronal image planes in normal
subjects and subjects with
strabismus. Error bands =
±2 SD. SR = superior rectus
muscle; LR = lateral rectus
muscle; IR = inferior rectus
muscle; MR = medial rectus
muscle, (open circles) Normal
subjects,
(closed diamonds)
Subjects with strabismus.
Plane 3
SR
15 -
5 -
MR
MR
LR
-5 -
LR
»-5-«H
H-6-H
IR
-15 -
IR
-15
-5
5
15
-15
-5
5
15
Horizontal Position from Orbital Center (mm)
aged 44° of ocular rotation from upgaze to downgaze
(normal subjects, 44.1° ± 6.3° SD; subjects with strabismus, 44.6° ± 6.8° SD). These differences were not
significant. Normal subjects averaged 40.7° (± 5.2°
SD) of ocular rotation from abduction and adduction.
Rectus EOM paths underwent small but consistent
changes with gaze. We term these shifts EOM path
sideslip. The effect of changes in gaze on EOM position in plane —1 are summarized in Figures 7 and 8,
and tabulated in Table 2, for normal subjects and
subjects with strabismus, respectively.
In general, EOMs were displaced more during
gaze changes in their plane of action (as agonists or
antagonists), and were displaced less during gaze
changes out of their plane of action. The displacements were small, averaging less than 2 mm even for
EOMs in their plane of action. Displacements perpendicular to the plane of action of EOMs were always in
a direction opposite the displacement of gaze; e.g.,
the lateral rectus (LR) path was displaced downward
on upgaze. Thus, these shifts do not simply reflect
the necessary movement of the EOM insertions as the
globe rotates.
In normal subjects and subjects with strabis-
234
Investigative Ophthalmology & Visual Science, January 1997, Vol. 38, No. 1
TABLE 4.
Rectus Pully Position
Displacements in Subject TL
3. Rectus Pully Position
Displacements in Subject JM
TABLE
Muscle
Right Orbit
Left Orbit
Muscle
Right Orbit
Left Orbit
Medial rectus
Superior rectus
Lateral rectus
Inferior rectus
0.7 mm
3.9 mm
3.8 mm
0.7 mm
0.6 mm
1.8 mm
4.6 mm
1.1 mm
Medial rectus
Superior rectus
Lateral rectus
Inferior rectus
2.6 mm
2.0 mm
3.7 mm
2.7 mm
4.2 mm
2.6 mm
5.1 mm
5.0 mm
inferior
lateral
inferior
medial
superior
lateral
inferior
medial
mus, the medial rectus (MR) muscle was the most
stable, shifting less than 0.4 mm from its primary
gaze position with horizontal rotations and less
than 0.3 mm with vertical rotations (Figs. 7, 8). The
superior rectus (SR) muscle was the most mobile,
but only in its plane of action. In normal subjects,
the SR shifted 1.6 mm inferiorly on upgaze and 1
mm superiorly on downgaze (for a total vertical
excursion of almost 3 mm), inferiorly on adduction
0.5 mm, and superiorly on abduction 0.8 mm (Figs.
7, 8). Horizontal gaze did not affect the horizontal
position of the SR in either normal subjects or subjects with strabismus. The LR muscle showed significant displacement during gaze changes perpendicular to its plane of action. In normal subjects,
the LR shifted inferiorly 0.7 mm on upgaze and
superiorly 0.8 mm on downgaze (for a total vertical
excursion of 1.5 mm), superiorly on abduction 1
mm, and laterally and inferiorly on adduction 0.5
&
SR
A
O
Primary Position
A
Upgaze
7
Downgaze
<
Abduction
>
Adduction
inferior
medial
superior
lateral
inferior
medial
superior
lateral
mm (Figs. 7, 8). The inferior rectus (IR) muscle
showed significant vertical and horizontal displacement, but only in its plane of action. In normal
subjects, the IR shifted medially 1.1 mm and inferiorly 1.0 mm on upgaze and laterally 1.3 mm and
superiorly 1.3 mm on downgaze (for a total vertical
excursion of 2.3 mm and horizontal excursion of
2.4 mm) while showing almost no shift in position,
either horizontally or vertically, during adduction
or abduction (Figs. 7, 8).
More posterior image planes showed a similar pattern in the direction of displacement of the EOM
paths during changes in gaze, only varying from plane
— 1 by showing a different magnitude of displacement.
The largest displacement inward of the horizontal
EOMs occurred in plane 3 (MR, 0.6 mm; LR, 0.4 mm)
and displacement outward occurred in plane 0 (MR,
0.7 mm; LR, 0.6 mm). The largest displacement inward of the vertical EOMs occurred in plane 0 for the
V
O
Primary Position
oSR
A
Upgaze
V
Downgaze
A
10-
5-
V
MR 0 <
0-
o
A
MR A
LR
•5-
-10-
?
IR
IR
O
A
-15-
-15
-10
-5
0
5
10
15
Horizontal Position from Orbit Center, mm
FIGURE 7. Average positions of centroids of all rectus extraocular muscles (relative to right orbital center and viewed as
if facing the subject) for normal subjects in plane —1 (3
mm anterior to the globe-optic nerve junction) in upgaze,
downgaze, abduction, abduction, and primary position. SR
= superior rectus muscle; LR = lateral rectus muscle; IR =
inferior rectus muscle; MR = medial rectus muscle.
-IS
-10
-5
0
5
10
15
Horizontal Position from Orbit Center, mm
FIGURE 8. Average positions of centroids of all rectus extraocular muscles (relative to right orbital center and viewed as
if facing the subject) for subjects with strabismus in plane
— 1 (3 mm anterior to the globe-optic nerve junction) in
upgaze, downgaze, and primary position. SR = superior rectus muscle; LR = lateral rectus muscle; IR = inferior rectus
muscle; MR = medial rectus muscle.
235
Location and Stability of Rectus Muscle Pulleys
Plane -2
Plane -1
15 _
T
1
5
SR
SR
-
MR <fr
i*6-i LR
LR
-
*
-5 -
IR
IR
-15 -
Plane 1
Plane 0
SR
SR
?
*
O
Ol
.•2
6
D
-
E
«
^
MR
LR
^H
J ^ MR
Q.
-
o
IR
IR
•E
FIGURE 9. Average positions
of centroids of the rectus extraocular muscles for primary
gaze in all coronal planes (relative to right orbital center)
in normal subjects and in subject JM. The left orbit has
been reflected to the configuration of the right orbit. Error bands = ±2 SD. Positions
demarcated with a white dot
in the center are more than 3
SD from the average normal
position, {open circles) Normal
subjects, {closed diamonds)
Subject JM right eye. {closed
boxes) Subject JM left eye.
Plane 2
Plane 3
15
SR
SR
5 _
t
h*n MR
LR
-5 _
t-^D—i
IR
IR
-15 -.
i
-15
-5
MR
5
i
i
15
-15
i
1
i
-5
i
5
i
i
15
Horizontal Position from Orbital Center (mm)
SR (1.9 mm) and plane —1 for the IR (1.3 mm), and
displacement outward for both occurred in plane — 1
(SR, 1 mm; IR, 1 mm).
The EOM sideslip in plane —1 for each EOM is
summarized in Table 2. There were no statistically
significant differences between the normal subjects
and the subjects with strabismus in displacement of
EOMs for various positions of gaze {P > 0.05). This
finding indicates that rectus EOM sideslip is generally
small and consistent in normal subjects and subjects
with strabismus.
Although as a group the subjects with strabismus
did not show abnormal EOM positions or sideslip, two
subjects with strabismus had clearly heterotopic EOM
positions. The first subject, JM, was a 60-year-old man
with a 4-year history of intermittent vertical diplopia
that manifested itself primarily when he was fatigued.
Examination revealed an intermittent left hypertropia
that was greater in downgaze and on right gaze, a
superimposed V-pattern intermittent exotropia, and a
marked inability to depress the left globe in adduction. Double Maddox rod testing revealed 5° of relative excyclotorsion. Left superior oblique palsy was
diagnosed clinically on the basis of the left hyper-
Investigative Ophthalmology & Visual Science, January 1997, Vol. 38, No. 1
236
Left Eye (Right Eye Fixing)
40
.
30
• • • • feW^T%+
10
0
-20
Right Eye (Left Eye Fixing)
t
+<f-^t^±^
+ "'$••
• •
:: '^Ar^r^rrv
G
a
z
e
d
e
g
-30
-40
AB 40 30 20 10
Intended
40
.k
20
-10
UP
V
e
0 - 1 0 -20 -30 -40 AD
—
30
20
• • • Vfr>
lj»
lyr
+
10
0
. . . 1;. . 2: . ji! . .
v^^m-
. . . p . p . IP. .^
.. .ft* -fc.:a^j
i
a
t
T.;b»,.... K . . . . U
-10
-20
-30
-40
AD -40 -30 -20 -10 0
DN
Horizontal Gaze, deg longitude
Simulation
**
Measurement
tropia, left superior oblique underaction, and excyclotropia.17 In primary position, the area centroids of
several of this subject's rectus EOMs were displaced
more than three standard deviations from normal.
Notable were bilateral inferior displacement of the
LRs and bilateral inferior and lateral displacement of
the SRs, both exceeding three standard deviations in
plane —1, plane 0, and plane 1 (Fig. 9). No normal
subject, and only one other subject with strabismus,
had rectus EOM displaced from the mean normal position more than three standard deviations in any scan
plane. The inferred stability of JM's pulleys was normal
during changes in gaze. The maximum midorbital
cross-sectional area of JM's right and left superior
oblique (SO) muscles were similar in primary gaze
(0.207 cm2 versus 0.212 cm2). The contractile changes
in maximum SO cross-section from upgaze to downgaze, 0.055 cm2 for the right SO and 0.068 cm2 for the
left SO, are both within the normal range as previously
described.1819 An Orbit computer simulation, with pulleys positioned to simulate JM's abnormal mean muscle positions (Table 3), exhibited JM's V-pattern exotropia and the increasing left hypertropia in downgaze
and right gaze, but it did not account for his left hypertropia in primary gaze. We reasoned that 4 years of
intermittent hypertropia had stretched the left IR. Increasing its assumed resting length by 4 mm yielded
a good simulation of JM's clinical condition (Fig. 10).
The second subject with strabismus, TL, a 30-yearold man with a history of early childhood exotropia,
had been treated with orthoptics and patching. Exami-,
nation revealed right hypertropia, large A-pattern exotropia, and excessive depression of both eyes during
adduction. Subject TL's pattern of strabismus was surprisingly unaltered by bilateral SO tenotomy, motivating MRI examination. Rectus EOM positions in primary position are summarized for subject TL in Figure
11. All four rectus EOMs in the left orbit, as .well as
••
10 20 30 40 AB
(Torsion X 5)
FIGURE 10. Hess screen for
subject JM showing the observed left hypertropia in primary gaze and V-pattern exotropia. Alignment was simulated by displacing normal
pulley positions in plane —1
by the observed displacement for subject JM (Table
3) and lengthening the left
inferior rectus muscle 4 mm
to account for the subject's
left hypertropia.
the SR and LR of the right orbit, were found to be
displaced more than three standard deviations from
normal in several image planes, so that the array of
right pulley positions appeared rotated clockwise and
the left orbit counterclockwise, as viewed facing the
subject. The inferred stability of TL's EOM pulleys did
not differ.from normal. An Orbit computer simulation,
with pulleys positioned to simulate TL's abnormal
mean muscle positions (Table 4), closely simulated
the A-pattern exotropia and increasing right hypertropia in right gaze but did not account for the right
hypertropia in primary gaze. Once again, a coincidental right IR abnormality (created by lengthening the
right IR muscle 2.5 mm) was used to simulate TL's
right hypertropia in primary gaze, completing the
computer simulation of his clinical condition. The
simulation captures the observed A-pattern and most
of the variation in the incomitant right hypertropia
(Fig. 12).
Additional computer simulations were performed using Orbit to predict the sensitivity of binocular alignment
to several rectus EOM path abnormalities. These computer simulations were performed to determine whether
rectus pulley positions within normal variation, as defined
by the measured standard deviations for normals, were
compatible with normal binocular alignment. Worst cases
were considered in which all pulley locations were altered
to produce synergistic effects on binocular alignment.
First, the array of the centers of all the rectus EOMs was
rotated two standard deviations clockwise from normal
for the right orbit and counterclockwise for the left orbit,
or vice versa, simulating the types of symmetrical malrotation of both orbits. In both cases, the effect on primary
position alignment was negligible, and the maximum deviation from orthotropia in extreme gaze (30° eccentric)
was 10A (5.7°) of horizontal deviation, 3A (1.7°) of vertical
deviation, and 4° of cyclotorsion, all probably within die
range of binocular fusion.17 Simulations using malro-
237
Location and Stability of Rectus Muscle Pulleys
Plane -2
15
Plane -1
-
j
5
-5
SR
-
D
-
o LR
•T*
MR HJH
I-O-HLR
T
MR KJM
l£
•r
-
O
IR
IR
-15
SR
-
<£»
Plane 1
Plane 0
SR
SR
C
T
8
-
6
From
LR
-5 -
c
*£
ff
MR
LR
KCH
O
S
in
o
a.
a
T
X
IR
5
IR
»rti<
T 11. Average positions
of centroids of the rectus extraocular muscles for primary
gaze in all coronal planes (relative to right orbital center)
in normal subjects and in subject TL. The left orbit has
been reflected to the configuration of the right orbit. Error bands = ± 2 SD. Positions
demarcated with a white dot
in the center are more than 3
SD from the average normal
position, {open circles) Normal
FIGURE
subjects, {closed triangles) Subject TL right eye. {closed boxes)
Subject TL left eye.
>
•
15
Plane 3
Plane 2
-
SR
SR
l-OH
5 -
>-Q-I
MR
h-OH MR
LR
•
-5 -
*Y
It
IR
IR
-15 H
i
-15
i
-5
i
5
i
i
15
\
-15
1—
-5
5
15
Horizontal Position from Orbital Center (mm)
tations of three standard deviations also predicted a negligible effect on primary position alignment but deviation
in extreme gaze increased to 14A (8°) horizontally, 5 A
(2.9°) vertically, and 6° of cyclotorsion, amounts challenging or overwhelming motor fusion.17 Finally, moving
EOM pulleys three standard deviations radially inward
(simulating a small orbit) or radially outward (simulating
a large orbit) had an insignificant effect on binocular
alignment in all gaze positions.
DISCUSSION
These high-resolution MRI data suggest that the positions of rectus EOM pulleys are defined precisely. Sev-
eral additional simulations help estimate the range of
pulley positions consistent with normal ocular motor
function. Displacement of the pulleys radially from
the orbital center does not appear to influence binocular alignment significantly. In contrast, displacement
of the pulleys perpendicular to their planes of action
by only a few millimeters may increase the risk of
strabismus by altering EOM pulling directions to a
degree that might exceed the compensatory capabilities of the central nervous system.20 In extreme cases,
such as with subjects JM and TL, grossly abnormal
rectus pulley positions seem likely to be the primary
cause of incomitant strabismus.
Investigative Ophthalmology & Visual Science, January 1997, Vol. 38, No. 1
238
Left Eye (Right Eye Fixing)
30
10
0
30
40
40
4f77^fer! T+
t
T- •"y-77~^y
• " rr^^L^J''^%' ''
^ T r ^ 1 . . ..
•*
z
e
d
e
g
30
{• ' JL^i^xi" ' " '20
G
• • • -f^y*<A_^j • + • • • a
10
20
Right Eye (Left Eye Fixing)
V
e
40
20
UP
• • •V
rr
T ^ T * L ^ ' ' '10
• • % ^ T ^ \ ^ A
•• 0
-10
• • •+'•^<^^^-\^ • •
i
"
T
" * T
i
a
t
-20
-30
-40
AB 40 30 20 10 0 -10 -20 -30 -40 AD AD -40 -30 -20 -10 0
DN
Horizontal Gaze, deg longitude
i>><<
-•- Intended
— Simulation
" Measurement
These findings are consistent with findings in children with craniosynostosis syndromes (i.e., Apert,
Crouzon, and Pfeiffer syndromes), who typically have
marked V-pattern exotropia, small, laterally rotated
orbits, and abnormally located extraocular muscles.21
In subject TL, all of the rectus EOMs were displaced
clockwise in the right orbit and counterclockwise in
the left orbit, giving rise to an A-pattern exotropia in
addition to a right hypertropia.
In subject JM, only the SR and LR were displaced
significandy from normal in both orbits. This subject
had acute onset of diplopia and was diagnosed with
left SO palsy because of left hypertropia that increased
on adduction of the left eye. Dynamic MRI of tfiis
subject, however, did not confirm this diagnosis (using
MRI criteria previously described1819). Alternatively,
we propose that congenitally anomalous rectus pulley
positions may have given rise to incomitant forces
within the range of motor compensation during the
subject's youth. This compensation may have been
disrupted by an event such as inflammation or trauma
to the left IR, which would have unmasked the Vpattern exotropia with incomitant hypertropia and
given the appearance of left SO palsy.
A particularly severe muscle path abnormality has
been documented recendy by MRI in the "heavy eye
syndrome."22 In this syndrome, esotropia and hypotropia develop in eyes with extreme axial myopia. Krzizok and colleagues22 have shown that such patients
exhibit a large inferior displacement of the path of
the LR muscle, with Orbit simulations consistent with
the idea that most of the normal abducting action of
the LR is thus converted to depression. This phenomenon presumably is associated with dehiscence of the
lateral levator aponeurosis, allowing the LR pulley to
shift inferiorly.
No significant differences in mean rectus pulley
sideslip during gaze shifts were found here between
•
10 20 30 40 AB
(Torsion X 5)
FIGURE 12. Hess screen for
subject TL showing right hypertropia in primary gaze and
A-pattern exotropia. Alignment was simulated by displacing normal pulley positions in plane —1 by the observed displacement for
subject TL (Table 4) and
lengthening the right inferior rectus muscle 2.5 mm to
account for the subject's
right hypertropia.
normal subjects and subjects with strabismus. Previous
work3'23 in four subjects showed that the EOM bellies
all tend to bow in toward the center of the orbit during
contraction and bow out from the center of the orbit
during relaxation while remaining relatively fixed during changes of gaze perpendicular to their plane of
action. The largest bowing movements, almost 4 mm,
were measured for the SR and the smallest bowing
movements, 1.5 mm, were measured for the IR.a In
the current, much larger study, all rectus EOMs clearly
showed similar bowing, but the horizontal EOMs
showed much smaller and more posterior bowing
compared with the vertical EOMs. This outward bowing of relaxed EOMs may be attributable to the radial
forces generated by the pulley slings, which extend
from the pulley rings located at the equator of the
globes as far posteriorly as the globe-optic nerve junction.9 The static tension within the pulley slings may
pull the relaxed EOMs outward toward the orbital
wall. Apparent inward bowing of the horizontal rectus
muscles deep in the orbit in image plane +3 may
represent an artifact of the contractile increase in muscle-cross sectional area in a region constrained on the
orbital sides by contact with the bony orbital walls,
forcing the contracting muscles' area centroids centrally.
Histologic studies are consistent with the current
findings in that the MR pulley contains the most fibroelastic and smooth muscle tissue9 and should have
the most rigidity, whereas the SR pulley has the least
fibroelastic tissue and should be least rigid.9 The LR
displaced litde with horizontal gaze changes and approximately 1 mm opposite to the direction of vertical
gaze changes (i.e., up during downgaze and down
during upgaze). These movements increase LR path
length and are opposite to predictions of all versions
of the shortest path hypothesis.1"4 One possible explanation for this increase in path length is that intermus-
Location and Stability of Rectus Muscle Pulleys
cular connective tissue posterior to the center of rotation may stabilize the LR relative to the globe.4'5 Another explanation points to the dense lateral levator
aponeurosis, coupling the LR to the SR (Fig. 5, plane
0). The lateral levator aponeurosis contains dense collagen, elastin, and smooth muscle.9 During upgaze, as
the SR bows downward 1.6 mm from its position in
primary gaze, the lateral levator aponeurosis and posterior Tenon's fascia sag inferiorly toward the LR,
allowing, we propose, the LR to sag down as well.
Conversely, as the SR bows superiorly 1 mm on downgaze, the LR may be pulled superiorly by the lateral
levator aponeurosis. The displacement of the LR superiorly 1 mm during abduction might be related to the
abducting action of the SR, in that under increased
tension, it might pull superiorly on the LR pulley by
the lateral levator aponeurosis.
The IR also exhibited unexpected behavior. It remained relatively immobile during changes in horizontal gaze. During changes in vertical gaze, the IR
bowed superiorly during contraction and inferiorly
during relaxation as expected but also showed significant horizontal displacement as well. The IR shifted
medially 1.1 mm during upgaze and laterally 1.3 mm
during downgaze. A possible explanation could be intermuscular coupling between the IR and the inferior
oblique (IO) muscle, termed Lockwood's ligament.24
We propose that the IO, contracting in upgaze, draws
its belly medially, pulling the relaxed IR medially as
well. During downgaze, relaxation of the IO and contraction of the IR could cause lateral displacement of
the inferior rectus.
In summary, the current study supports previous
work showing that rectus EOM paths undergo small
displacements during changes of gaze.4'5 The current
study reveals some new complexities of the fibroelastic
pulley system. The normal position and sideslip of the
fibroelastic pulleys have been defined. Two subjects
were discovered to have anomalous rectus EOM pulley
positions that could form the structural basis for incomitant strabismus. In subject TL, both orbits appear
rotated in a manner predicted by biomechanical simulation to produce an A-pattern strabismus. In subject
JM, anomalous location of the SR and LR, coupled
with an inferior rectus abnormality, simulated the clinical pattern of SO palsy. Anomalous pulley position
can explain some cases of poor response to strabismus
surgery for clinical oblique muscle dysfunction.
The system of orbital fibromuscular connective
tissues provides mechanical coupling among the
EOMs. The current MRI evidence indicates specific
roles for coupling between LR and SR muscles and
between IR and the IO muscles.
Key Words
binocular alignment, extraocular muscles, magnetic resonance imaging, pulleys, strabismus
239
References
1. Krewson WE. The action of the extraocular muscles:
A method of vector analysis with computations. Trans
Am Ophthalmol Soc. 1950;48:443-486.
2. Robinson DA. A quantitative analysis of extraocular
muscle cooperation and squint. Invest, Ophthalmol.
1975; 14:801-825.
3. Miller JM, Robinson DA. A model of the mechanics
of binocular alignment. Comput Biorned Res. 1984;
17:436-470.
4. Miller JM, Robins D. Extraocular muscle sideslip and
orbital geometry in monkeys. Vision.Res. 1987; 27:38192.
5. Miller JM. Functional anatomy of normal human rectus muscles. Vision Res. 1989;29:223-240.
6. DemerJL, Miller JM, Rosenbaum AL. Effect of transposition surgery on rectus muscle paths by magnetic
resonance imaging. Ophthalmology. 1993; 100:475-487.
7. DemerJL, Miller JM, Poukens V. Surgical implications
of the reed extraocular muscle pulleys. f Pediatr Ophthalmol Strabismus. 1996; 33:208 - 218.
8. Koornneef L. New insights in the human orbital connective tissue: Results of a new anatomical approach.
Arch Ophthalmol. 1977; 95:1269-1273.
9. DemerJL, Miller JM, Poukens V, Vinters HV, Glasgow
BJ. Evidence for fibromuscular pulleys of the reed
extraocular muscles. Invest Ophthalmol Vis Sci. 1995;
36:1125-1136.
10. PorterJD, Poukens V, Baker RS, DemerJL. Structurefuncdon correlations in the human medial rectus extraocular muscle pulleys. Invest Ophthalmol Vis Sci.
1996; 37:468-472.
11. DemerJL, Park CH, Howard TD, Miller JM. The oculomotor plant simplifies binocular yoking during vertical gaze shifts. ARVO Abstracts. Invest Ophthalmol Vis
Sci. 1996;37:S165.
12. DemerJL, MillerJM, Rosenbaum AL. Clinical correlations of models of orbital statics. In: Scott AB, ed.
Mechanics of Strabismus Symposium. San Francisco:
Smidi-Kettlewell Eye Research Institute; 1992; 141 —
161.
13. MillerJM, Shamaeva I. Orbit® 1.5 Gaze Mechanics Simulation. San Francisco: Eidacdcs; 1995.
14. Frueh BR, Musch DC, Grill R, Garber FW, Ham by S.
Orbital compliance in Graves' eye disease. Ophthalmology. 1992; 92:657-665.
15. MillerJM, DemerJL. Biomechanical analysis of strabismus. Binocular Vision Eye Muscle Surg Q. 1992; 7:233248.
16. Matthews DE, Farewell VT. Using and Understanding
Medical Statistics. New York: Karger; 1988:177-178.
17. von Noorden GK. Binocular Vision and, Ocular Motility:
Theory and Management, of Strabismus. 4th ed. St. Louis:
CV Mosby; 1990.
18. DemerJL, MillerJM. Magnedc resonance imaging of
the functional anatomy of the superior oblique. Invest
Ophthalmol Vis Sci. 1995;36:906-913.
19. Mehta AM, Demer JL. Magnetic resonance imaging
of the superior oblique muscle in superior oblique
myokymia. f Pediatr Ophthalmol Strabismus. 1994;
31:378-383.
240
Investigative Ophthalmology & Visual Science, January 1997, Vol. 38, No. 1
20. Ygge J, Zee DS. Control of vertical eye alignment in threedimensional space. Vision Res. 1995; 32:3169-3181.
21. Cheng H, Burdon MA, Shun-Shin GA, Czypionka S.
Dissociated eye movements in craniosynostosis: A hypothesis revived. Br J Ophthalmol. 1993; 77:563-568.
22. Krzizok T, Wagner D, Kaufmann H. Elucidation of the
restrictive motility disorder in high myopia by MRI. ARVO
Abstracts. Invest Ophthalmol Vis Sri. 1996;37:S281.
23. Simonsz HJ, Harting F, de Waal BJ, Verbeeten BWJM.
Sideways displacement and curved path of recti eye
muscles. Arch Ophthalmol. 1985; 103:124-128.
24. Lockwood CB. The anatomy of the muscles, ligaments, and fasciae of the orbits, including an account
of the capsule of Tenon, the check ligaments of the
recti, and of the suspensory ligament of the eye.JAnat
Physiol. 1885-6;20:l-25.