Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
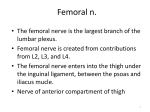
367 Introduction adhistory Uses of the femoral nerve are documented in the lite allows blockade of three ne: oral nerve, the lateral fei and the obturator nerve, Anesthesia and analgesia c Figure 1 Anatomy Femoral vein Femoral artery Skin Fascia lata 00 Table I Surgical procedures amenable to femoral nerve block/3-in-1 block 1. Unilateral saphenous vein stripping 2. Knee arthroscopy* 3. Muscle biopsy of anterior thigh' 4. Split thickness skin graft 'Supplemented with lateral femoral cutaneous nerve block Table II Pain management uses of the femoral nerve block/ 3-in-i block 1. Femur fractures 2. Anterior cruciate ligament reconstruction 3. Split thickness skin grafts of thigh* 4. Osteotomies' 5. Pin or plate insertion or removal* *Supplemented with lateral femoral cutaneous nerve block Fasia ilia &~pwasFemoral nerve Pectineus muscle ~musc ,p vastus medialis, and vastus intermedius. The lateral femoral cutaneous nerve is formed by the posterior division of L2 and L3 and emerges slightly more proximal than the femoral nerve from the lateral border of the psoas muscle. The lateral Figure 3 Landmarks femoral cutaneous nerve is a purely sensory nerve with branches supplying the lateral buttock, thigh, and the knee joint.'"' The obturator nerve is formed by the ventral branches of L2, L3, and L4. It emerges from the medial border of the psoas muscle. Sensory branches to the medial thigh may or may not occur. Other branches innervate the hip joint, external obturator, gracilis, and adductor muscles, and an articular branch innervates the knee joint'"' (Figure 2). igure V-Femoral vein A-Femoral artery FN-Femoral nerve Solid line-Inguinal ligament i SCutaneous innervation Lateral femoral cutaneous nerve Obturator nerve (inner thigh) ".. Femoral nerve ]UH Saphenous nerve Techniques of femoral nerve block and 3-in-i block There are four basic techniques for blocking the femoral nerve at the level of the inguinal ligament. The landmarks are the same for all four of the techniques (Figure 3). With the patient in the supine position, the anterior superior iliac spine and the symphysis pubis are identified. An imaginary line between these structures will identify where the inguinal ligament lies. Next, the femoral artery is palpated below the inguinal ligament. A 22-gauge 2 to 4-cm (1 to 2 in) needle is inserted perpendicular to the skin immediately lateral to the femoral artery. In the first technique, the needle is advanced until maximum pulsation of the needle occurs or a August 1998! VoL 66/No. 4 paresthesia is elicited.' A second, technique elicits no paresthesia or pulsations and utilizes a short beveled needle. Identification of proper placement is based on two "pops." This indicates that the needle has crossed the fascia lata and fascia iliaca." A third technique of identification of the nerve is the use of a peripheral nerve stimulator and identification of quadriceps contraction. A fourth technique is to deposit local anesthetic in a fanwise fashion lateral to the femoral artery.' No studies have compared the four techniques in terms of successful blockade. We have found that the peripheral nerve stimulator is easily administered, positively identifies the femoral nerve, and reduces the chance of nerve damage by "seeking" paresthesias. An inguinal paravascular block or 3-in-i block is carried out in the same manner except that the needle is directed slightly cephalad, and distal pressure is maintained to force the local anesthetic cephalad instead of in a distal direction.' The difference between a femoral nerve block and a 3-in-i block is related to the. volume of local anesthetic. It has been reported that anywhere between 5 and 20 mL"3'35," of local anesthetic can be used for a femoral nerve block, whereas 20 mL or more'l 33 s" of local anesthetic is used for a 3-in-i block. The more volume used, the more the local anesthetic solution will travel to anesthetize additional nerves and provide for a denser block. s itreally a34n-1 block? Controversy has characterized discussions of the 3-in-i block. Is it a 4-in-i block, 3-in-i block, or 369 2-in-i block? 37 The anterior approach to the 3-in-i block by paresthesia and nerve stimulation was effective in blocking the lateral femoral cutaneous nerve and the femoral nerve but consistently missed the obturator nerve. It was proposed that the dose of 0.5 mL/kg of local anesthetic did not travel far enough proximally or laterally to block the obturator nerve.4 ' A second study found that the obturator nerve was blocked only 4% (1 out of 26) of the time.12 The original description by Winnie et al of shortest total time (mean * SD) for short stay at 271 t 43 minutes, the time for the general anesthesia group was 292 ± 62 minutes, for the lidocaine spinal group, 298 * 75 minutes, and for the bupivacaine spinal group, 371 t 85 minutes. Of the patients who received a femoral nerve block, 31% (5 out of 16) complained of pain during the PACU stay compared with 47% (8 out of 17) in the spinal group and 72% (13 out of 18) of those in the general anesthetic group. more of local anesthetic would assure anesthesia of After discharge to home, 31% (5 out of 16) of the patients who received femoral nerve block re- the lateral femoral cutaneous, femoral, and the obturator nerves. 3 Winnie et al did not describe how ported pain compared with 47% (8 out of 17) of those who received a spinal block and 38% (7 out of the 3-in-i block indicated that volumes of 20 mL or the block was tested.3 Interestingly, different results utilizing 20 mL and 40 mL of a 1% concentration of mepivacaine were found in another study concerning blockade of the obturator nerve. The obturator nerve was blocked 62% (24 out of 39) and 78% (33 out of 41), respectively.4 This difference may be due to different evaluation techniques used in the studies. 18) who received general anesthesia. In addition, there was no incidence of backache or nausea and vomiting in the femoral nerve block group. In the spinal anesthetic group, the incidence of backache was 6% (1 out of 18) and nausea and vomiting, 12% (2 out of 17). In the general anesthetic group, the incidence of backache was 16% (3 out of 18) and nausea and vomiting, 28% (4 out of i8).4 In one study, the authors utilized a test of motor Femoral nerve blocks combined with a lateral and sensory blockade, 4 and in the other study, only sensory evaluation was undertaken. 3 The spread of methylene blue after 3-in-i blocks in six cadavers was studied" After dissection, it did not appear that the dye traveled along the femoral nerve, and there was no gross or microscopic evidence of a femoral sheath. The dye spread under the iliacus fascia laterally over the iliopsoas and iliacus muscles. The dye did not spread medially into the pelvis and did not reach the obturator nerve since the iliacus fascia is attached to the pelvic rim." femoral cutaneous nerve block have been used in pediatrics for postoperative pain relief, with a success rate of 96% for orthopedic procedures and skin grafts in the distribution of the femoral nerve and lateral femoral cutaneous nerves.5 The blocks were placed after induction of general anesthesia. No complications were noted. Oral analgesics were commenced when the patient was awake to prevent the onset of severe pain when the block wore off.5 Femoral nerve block supplemented with a lateral femoral cutaneous nerve block has been advocated for skin grafting procedures. The advantages over Based on the anatomical evidence and review local infiltration include a requirement for less total of literature, we conclude that the 3-in-i nerve block would be best described as a 2-in-i nerve block or a combined femoral nerve and lateral femoral cuta- anesthetic agent, less discomfort with administra- neous nerve block. Uss of femoral neve block A comparison of general anesthesia, spinal anesthesia, and femoral nerve block in patients who underwent unilateral saphenous vein stripping was undertaken.4 The technique for general anesthesia was not described; bupivacaine or lidocaine was utilized for spinal block, and 3% chloroprocaine was used for femoral nerve block. The mean 1 SD time in the postanesthesia care unit (PACU) was the shortest for the general anesthesia group at 69 f 21 minutes; the time in PACU after femoral nerve block was 85 33 minutes, and the spinal anesthetic group had a PACU time of 100 = 30 minutes for lidocaine and 128 ± 56 minutes for bupivacaine. The femoral nerve block group had the 370 tion, less distortion, and a lack of moisture from a local anesthetic to interfere with dermatome glue.6 , A case report demonstrated the effectiveness of continuous femoral nerve block for postoperative pain management in a 13-year-old boy who had surgery for patella alta.' The femoral catheter was inserted after general anesthesia was instituted. The upper thigh was prepared aseptically, and a small incision was made lateral to the femoral artery immediately below the inguinal ligament. An 18-gauge 5-cm intravenous catheter was threaded over a 22-gauge spinal needle and advanced through the incision parallel to the artery at a 300 angle to the skin.The position was confirmed with a nerve stimulator and movement of the patella. The catheter was sutured and connected to sterile extension tubing, and a sterile occlusive dressing was applied. On the first postoperative day, an injection of 15 mL of 0.75% bupivacaine was admin- Journalof the American Association of Nuse Anesthetists istered every 6 hours. On the second day, a continuous infusion of 0.5% bupivacaine at 4 mL/h was started. The infusion concluded 24 hours later. Negative cultures were obtained from the local anesthetic reservoir and distal catheter. No complica- pop occurred, the needle and guide wire were removed, and the catheter was advanced. After negative aspiration, a bolus of 0.5 mL/kg of 0.25% bu- The periosteum of the femur is innervated primarily by the femoral nerve. The distal and proximal portions of the femur contain contributing innervation from the obturator nerve and sciatic nerve. Although other analgesic and anesthetic techniques could be utilized for femur fractures, the femoral nerve block is the indication that is most frequently cited in the literature. 8-"2 For children who had a fracture of the middle third of the femoral shaft, utilization of a femoral nerve block with 0.5% bupivacaine at a dose of 2 mg/kg provided rapid analgesia within a mean + SD time of 8 ± 3.5 minutes."3 The femoral nerve block was placed with the subject awake after the skin was anesthetized with 1%lidocaine. All subjects had a pain rating grade of 3 (crying, pain expressed spontaneously, and handling impossible) or 4 (crying, tachycardia greater than 60% of normal rate for age, and handling is impossible) before the femoral nerve block. After the block, the pain grade decreased to 0 (calm, no spontaneous pain or pain during handling) for 85% (11 out of 13) of the subjects and to 1 (calm, no spontaneous pain, pain during handling) for 15% (2 out of 13) of the subjects. The exact duration of femoral nerve block could not be determined since traction had a definitive analgesic effect. Traction placement occurred at a mean ± SD of 124 -* 19 minutes after the femoral nerve block. The block was successful in 93% (14 out of 15) of the subjects."~ Femoral nerve block for fractured femurs was most effective for fractures of the middle third of the femur in a study of 25 adults and children.' 5 Pain relief was obtained at the proximal and distal portions of the femur but was not as complete due to contributions of innervation by the obturator nerve and sciatic nerve.' 4 It has been recommended that femoral nerve blocks should be used for patients who sustained femoral neck fractures. Although the block does not abolish pain, it greatly reduces pain and the need for systemic analgesia."-5 Continuous femoral nerve block in pediatric patients was effective in providing analgesia and decreasing or eliminating the need for parenteral narcotics after femur fracture.' 6 After sterile skin preparation, a 3F, 8-cm single-lumen central venous catheter was inserted using the Seldinger technique. The catheter was placed 2 to 4 cm below the inguinal ligament just lateral to the femoral artery. A double pop technique was used. Once the second patients had a continuous infusion for 4 to 6 days tions were noted.7 August 1998/ VoL 66/No. 4 pivacaine with 1:200,000 epinephrine was administered, followed by a continuous infusion of 0.2% bupivacaine at a rate of 0.15 mL/kg per hour. Three and required no supplemental analgesia. One patient had a continuous infusion for 4 days but required two doses of fentanyl for supplemental analgesia. 6 Four advantages for the use of the femoral nerve block in patients who have sustained fractured femurs have been cited.' First, the block provides superior analgesia compared with narcotics, in part by preventing the protective spasms of the quadriceps muscle. Second, the block allows for assessment of associated injuries without adminis- tering medications that alter the level of consciousness. Third, the patient can be moved for radiological procedures without experiencing severe pain. Fourth, with some sedation when indicated, the fracture can be reduced and splinted without the use of general anesthesia." The use of the femoral nerve block for postoperative analgesia after total knee arthroplasty has not been consistently effective. The knee joint is also innervated by the sciatic and obturator nerves, reducing the effectiveness of analgesia by this technique.8 "9 Femoral nerve block for analgesia after surgery on the knee ligament decreased analgesic requirements in the immediate postoperative period.' At 12 hours postoperatively, there was no difference in use of analgesics between those who received a femoral nerve block and those who did not. Fanwise infiltration of local anesthetic was performed 2.54 cm (1 in) below the inguinal ligament immediately lateral to the femoral artery. The authors used 20 mL of 0.25% bupivacaine.o The concentration of bupivacaine, the volume, or both may have been inadequate. Postoperative analgesic requirements in patients undergoing anterior cruciate ligament repair were compared.2" One group of 50 subjects who received a femoral nerve block with 20 mL of 0.5% bupivacaine by infiltration before surgery was compared with a control group, which received no block. For the group that received the femoral nerve block, intramuscular narcotic requirements were decreased by 80% in the recovery room and by 40% during the first 24 hours after surgery. A second portion of this study compared preoperative and postoperative placement of the femoral nerve block. A 50% decrease in the use of intramuscular narcotics -in the recovery room and during the first 24 postoperative hours was found. Only 10 were used in each group.2 No power anal done to determine whether there is really ence between the two groups or whether t] ing was due toa larger variability in a small nephrinE ported fc ul use of 0.5% bu a dose of2 to 3 ostoperative pain tients un( cruciate room. Eight percent of the subjects required parenteral narcotics after the femoral nerve block, and 21% required ketorolac after the femoral nerve blockYn A dose of 2 to 3 mg/kg of 0.5% bupivacaine in a 70-kg adult would result in volumes of 28 to 42 mL and should be termed a 3-in-i block and not a femoral nerve block. Femoral nerve block combined with lateral femoral cutaneous nerve block in patients undergoing muscle biopsy for testing of malignant hyperthermia susceptibility has been used successfully. The technique provided safe and effective anesthesia for 282 patients. 2 A 3-in-i block could be used for procedures that utilize a femoral nerve block with supplemental lateral femoral cutaneous nerve block and would reduce the need for additional injections. As noted, when the 3-in-i nerve block successfully blocked the femoral nerve, the lateral femoral cutaneous nerve was blocked in 96% (25 out of 26) of the patients.2 a 70 Uses of 3-In-I block The use of the 3-in-i block, with 20 mL of 2% chloroprocaine and 1:200,000 epinephrine, combined with an intra-articular injection of 20 mL of 2% lidocaine provided excellent anesthesia for knee arthroscopy.26 Patient satisfaction was measured by asking the patient to grade satisfaction on a scale of 1 (very satisfied) to 5 (unsatisfied). Patient satisfaction was very high, with a mean * SD score of 1.5 f 0.5. Surgical operating conditions were graded by the surgeon on a four-point scale; 1 indicated excellent and 4, unacceptable. None of the subjects required a general anesthetic. A single-injection 3-in-i block was compared with a 3-in-i block combined with a separate block of the lateral femoral cutaneous nerve and with general anesthesia for knee arthroscopies. The authors used 20 to 25 mL of 1.5% mepivacaine or lidocaine for the 3-in-i block. In the group of patients who received a 3-in-I block, 27% (18 out of 30) had pain during the lateral knee incision. In the group that received a supplemental lateral fem- 1372 [ject+ pen analgesia a fixation wa found that first 12 hours, while all the sub receive a block required analgesi in analgesic usage during the tween the groups was statisti (P<.05). The 3-in-i nerve block has utilized as the sole anesthetic in ing muscle biopsy of the vastus n nant hyperthermia testing,' util Journal of the American Association of Nurse Anesthetists 47,48 used.'~Plasma~ levels were measured and reported in one case report and three studies. In the case report, a 54-kg female patient received an accidental overdose of 180 mg of 0.5% bupivacaine. The peak venous plasma level was noted at 0.92 pg/mL and occurred 45 minutes after injection 41 One study tracked the venous blood samples in six patients for each local anesthetic group. The subjects received 0.6 mL/kg of 1% lidocaine or 0.25% bupivacaine with 1:100,000 epinephrine, up to a maximum of 40 iL. 31 The median peak plasma level in the lidocaine group was 1.85 Table III Contraindications to femoral nerve block/3-in-1 block 1. Burn or infection at site of injection 2. Vascular graft to femoral artery 3. Coagulopathy 4. Neurological disease 5. Patient refusal Table IV Complications of femoral nerve blockl3-in-1 block 1. Hematoma 2. Intravascular injection 3. Femoral nerve dysesthesia or paresis 4. Femoral nerve palsy 5. Toxic effects of the local anesthetic 6. Prolonged motor blockade of quadriceps 7. Methemoglobinemia with the use of prilocaine ; _;;; August 1998 Vol 66/No. 43 ;.-;; ; ; pg/nL (range, 1.22-4.42 pg/mL). The median peak plasma level for the bupivacaine group was 0.67 ug/mL (range, 0.35-0.80 pg/nL). Both groups had a median peak concentration 37.5 minutes after the block was inserted."1 A second study utilized a bolus of 2 mg/kg or 0.5% bupivacaine in 10 children followed by a continuous infusion of 0.25% bupivacaine at 0.35 mg/kg per hour.3 The median venous plasma concentrations of bupivacaine did not exceed 1.2 pg/iL, and the maximal peak concentration was 2.1 pg/mL. No patient exhibited signs of toxicty. 30 Nine children received 2 mg/kg of 0.5% bupivacaine for management of pain for fractures of the middle third of the femur. Plasma bupivacaine levels were studied in subjects weighing a mean * SD of 25.3 f 10.6 kg, and in all but one subject, levels were lower than 1.2 pg/nL. One sub- ject had a level of 1.52 jpg/nL, which was attributed to a partial intravascular injection.3 The established threshold for toxicity for bupivacaine is 373 2 to 4 pg/mL and for lidocaine is 5 to 10 dg/mL. The third study utilized 35 mL of 0.75% prilocaine for postoperative analgesia in patients who had a fractured head of the femur that was corrected with a compression screw or pin and plate.27 For 12 patients in whom plasma prilocaine levels were obtained, the peak levels were lower than the suggested threshold of 6 pug/mL for toXicity. 27 Prolonged femoral nerve blocks with motor blockade of the quadriceps have been noted after the use of bupivacaine.4 9 In the first case report, 0.5% bupivacaine was given in a dose of 180 mg instead of 0.25% bupivacaine. No signs of systemic adverse effects were noted. The motor blockade lasted for 30 hours, and discharge was delayed.49 In a second case, 20 mL of 0.25% bupivacaine was used for pain management after knee arthroscopy. Quadriceps weakness persisted for 8 hours, and discharge was delayed until the next day.5 In a third case, 30 mL of 0.5% bupivacaine was injected, and the patient experienced a motor blockade that lasted 36 hours and a sensory blockade that lasted 60 hours. 5 ' In a fourth case, 15 mL of 0.5% bupivacaine was injected, and the patient experienced some loss of quadriceps function, which returned to normal by 40 hours.52 In none of these cases was there any neurological damage, and quadriceps weakness resolved when the bupivacaine wore off. Bupivacaine is inappropriate in same-day surgical procedures when the patient will need to use the quadriceps. However, if the patient's leg will be immobile and the patient will use crutches, this technique may be appropriate if the patient is informed about the duration of blockade. The use of prilocaine for 3-in-i block may lead to methemoglobinemia.59 Further studies Clearly there is room for further study and research concerning these nerve blocks. Some of the areas that we believe deserve study include: 1. A comparison of the four techniques of blockade and the success rate of each blockade. 2. Optimal dosing of lidocaine or mepivacaine in the outpatient population to avoid residual weakness of the quadriceps. 3. Whether preincision placement of the 3-in-i nerve block reduces postoperative analgesics more than placing the block at the end of surgery. 4. What dose of local anesthetic is required to consistently block the lateral femoral cutaneous nerve during a 3-in-i nerve block. 5. Cost-effectiveness of blocks compared with other modalities of postoperative pain management. 374 Conclusions The literature describes a number of uses for these blocks in anesthesia and analgesia. These blocks are technically easy to administer by appropriately trained anesthesia providers utilizing the correct equipment and technique. Renewing our interest in these blocks may allow us to utilize these blocks as viable alternatives to other methods of anesthesia and analgesia. Selective use of these techniques and further studies are required, but we should certainly not discount these blocks in our practice. REFERENCES (1) Bridenbaugh P0. The lower extremity: Somatic blockade. In: Cousins MJ, Bridenbaugh P0, eds. Neunal Blockade in Chnical Anesthesia and Management of Pain Philadelphia: JB Lippincott Co. 1988:428-429. (2) Adriani J. 1kchniques and Procedures of Anesthesia Springfield, Illinois: Charles C. Thomas Publishers. 1950:301-302. (3) Winnie AP, Ramamurthy S, Durrani Z. The inguinal paravascular technic of lumbar plexus anesthesia: The "3-in-1 block." Anesth Anaig. 1973;52:989-996. (4) vloka J, Hadzic A, Korduba Z, Mulcare R, Kitain E. Anesthesia for long saphenous vein stripping in ambulatory surgery setting: Comparison of femoral nerve block, spinal, and general anesthesia. Rag Anesth. 1995;20(25):24. Abstract. (5) McNicol LR. Lower limb blocks for children. Anaesthesia. 1986;41:27-31. (6) Earle As, Kiehn CL, DesprezJD. Regional block of the thigh: Uses in plastic surgery. Plast Reconstr Surg. 1972;49:134-137. (7) Rosenblatt RM. Continuous femoral anesthesia for lower extremity surgery. AnesthAnaig. 1980;59:631-632. (8) Brennan RJ. A case that illustrates the distinct advantages of femoral nerve block [letter]. JEmergMed 1993;11:623-624. (9) Grossbard GD, Love BR. Femoral nerve block: A simple and safe method of instant analgesia for femoral nerve blocks in children. Aust NZJSurg. 1979;49:592-594. (10) Denton JS. Manning MA. Femoral nerve block for femoral shaft fractures in children: Brief report. JBoneJointSurg~r.1988;77:84. (11) McGlone R, Sadhra K, Hamer DW, Pritty PE. Femoral nerve block in the initial management of femoral shaft fractures. Archives of Emergency Medicine. 1987;4:163-168. (12) Finlayson BJ, Underhill TJ. Femoral nerve block for analgesia in fractures of the femoral neck. Archives of Emergency Medicine. 1988;5:173-176. (13) Ronchi L, Rosenbaum D, Athouel A, et al. Femoral nerve blockade in children using bupivacaine. Anesthesiology. 1989;70:622-624. (14) Tondare A, Nadkarni A. Femoral nerve block for fractured shaft of femur. Can Anaesth Socd. 1982;29:270-271. (15) Hadad FS, Williams RL. Femoral nerve block in extracapsular femoral neck fractures. JBone JointSurgr.1995;77-B:922-923. (16) Tobias J. Continous femoral nerve block to provide analgesia following femur fracture in a paediatric ICU population. Anaesth Intensive Care. 1994;22:616-618. (17) Berry FR. Analgesia in patients with fractured shaft of femur. Anaesthesia 1977;32:576-577. (18) Horde AH, Roberson JR. Thompson WF, Cohen DE, Kelly PM, Hammonds WD. Evaluation of continous femoral nerve analgesia after primary total knee arthroplasty. Anesth Analg. 1990;70:5164. Abstract. (19) Hirst GC, Lang SA, Dust WN, Cassidy JD, Yip EW. Femoral nerve block: Single injection versus continous infusion for total knee arthroplasty. RegAnesth. 1995;21:292-297. (20) Tierney E, Lewis G, Hurtig JB, Johnson D. Femoral nerve block with bupivacaine 0.25 percent for postoperative analgesia after open knee surgery. CanJAnaesth.1987;34:455458. (21) Ringrose NH, Cross MJ. Femoral nerve block in knee joint surgery. AmiSponts Mea 1984;12:398-402. (22) Edkin BS, Spindler KP, Flanagan JF. Femoral nerve block as an alternative to parenteral narcotics for pain control after anterior cruciate ligament reconstruction. Arthroscopy 199511:404409. Journal of the American Association of Nurse Anesthetists (2$) Berkowitz A, Rosenberg H. Femtoral block with mepivacaine for muscle biopsy in malignant 2hyperthermia patients Anethesology. 1985;6265i-652. (24) Maccant RM, Wedel DlJ, Melton A, Gronert GA. Femtoral and lateral femoral cutaneous nerve block for muscle biopsies in children. hediatrAneth. 1995;5223-227. (25) Goranson BD), Lang SA, Dust WN. Combined femoral 3 in 1 nerve block and intra-articular local anesthesia for knee arthroscopy. Rteg Anestk. i995(su ppl) 29. (26) Pate! NJ, Flashburg MH, Paskin S, Grossman L.A regional anesthetic technique compared to general anesthesia for outpatient knee nthroscopy. Ansh As4 i986;65:85-187. (27) Hood G, Edbrooke DL, Gerrish S. Postoperative analgesia after triple nerve block hor fractured neck of femur. Anaesthesia. 199i;46: 138-140. (28) Goad NU. Post-operative analgesia following femoral-neck surA comparison between Sin I nerve block and lateral femoral cutaneous nerve block Bur/ Anaesthesiot 199i;&287-290. (29) Edwards ND, Wright EM. Continous low dose S-in-I nerve blockade for postoperative pain relief after total knee replacement. Anesth gey: A n4g1992;75:205-267. (30) Dahl JR. Christiansen CL, Daugaard JJ, Schultz P, Carlsson P. Continous blockade of the lumbar plexus after knee surgery: Postoperative analgesia and bupivacaine plasma concentrations. Anaesthesia 1988;43:1015-10i8. (Si) Madej TH, Ellis PR, Halsall PJ. Evaluation of "S in 1" lumbar plexus block in patients having muscle biopsy. Br JAnenk. 1989;62: 515-517. (32) Snell US. Clinical Anatomy for Medica! Students. 4th ed. Boston: Little, Brown and Co. 1992. (33) Katz J. Atlas of Sqgional Anesthesia 2nd ed. Norwalk, Connecticut: Appleton &Lange. 1994. (54) Khoo ST Brown TCG. Pemnoral nerve block: The anatomical basis for a single injection technique. Anaesth Intensive Cart.1983;iI:40-42. ($5) Lind J. inguinal paravascular approach to lumbar plexus analgesia (the "S-in-i" block). in: Perranite PM, Vadefloncouer TR, eds. Postoperative Pain Management. New York: Churchill Livingstone, 1993:335-341. (36) Eriksson E, ed. Jllustruted Handbook in Local Anesthesia 2nd ed. Philadelphia: WB Saunders Co. 1980:106-107. (37) Mansour NYt -in-i or 4-.n-l [letter]? RegAnesik. 1992;17:242-243. (38) Spillane WY. S-in-I blocks and continous 3-in-I blocks [letter]. RegA AIL t1992;17:i75-i76. (39) Winnie AP The "S-in-i" block": Is it really 4-in-i or 2-in-i [letter]?Reg Anesth. 1992;17:176-i79. August 1998/ VoL 66/No. 4 (40) Balas GI. In defense of the 3-in-i block [letter]. Reg Anesek. 1992;17:244. (41) Parkinson SK, Mueller JR, Little WL, Bailey SL. Extent of blockade with various approaches to the lumbar plexus. AnethA4n4l i989;68:243-248. (42) Lang SA, Yip RW, Chang PC, Gerard MA. The femoral S-in-i block revisited.JClinAnesth. 1993;292-296. (43) Seeberger MD, Urwyler A. Paravascular lumbar plexus block: Block extension after femora) nerve stimulation and injection of 20 vs. 40nit mepivacaine 10 mg/mt.AcnaAnesthesiolScandi 1995;39:769-773. (44) RitterJW. Femoral nerve "sheath" for inguinal paravascular lumbar plexus block is not found in human cadavers. Clin Aneis.th 1995;7:470-473. (45) Candido K, Winnie A, Covino B, Ran , Vasireddy A, Masters U. Addition of bicarbonate to plain bupivacaine does not significantly alter the onset or duration of plexus anesthesia. Reg Anesth. 985;20: 133-138. (46) Mulroy MI. Peripheral nerve blockade. In: Barash PG, Cullen B, Stoelting UK, eds. Clinic.! Anesthesia. 2nd ed. Philadelphia: JR Lippincott Co. 1992:843-844,867-868. (47) Prerk CM. Palsy after femqral nerve block [letter]. Anaesthesia 1988;43:167-i68. (48) McNicol LU. Palsy after femoral nerve block [letter]. Anaesthesia. 1988;43:509. (49) Madej TH, Ellis FU, Halsall PJ. Prolonged femoral nerve block with 0.5% bupivacaine [letter. Anaesthesia. 1988;43:607-608. (50) Bradshaw E, Mcflale S. Bupivacaine and femoral nerve block [letter].Anaesthesia i989;44:i74. (51) Lynch J. Prolonged motor weakness after femoral nerve block with bupivacaine 0.5% [letter]. Anaesthesia 1990;45:421. (52) Hutchison GL, Bartbram CN. Unilateral spinal anesthesia and prolonged femoral nerve block (letter]. Anaesthesia. 1990;45:987. (53) Bellamy MC, Hopkins PM, Halsall PJ, Ellis FR. A study into the incidence of methaemoglobinaemia after "three-in-i" block with prilocaine. Anaesthesia i992;47:i084i085. AUTHORS Daniel D).Moos, CRNA, MS, is employed by Kearney Anesthesia Associates, PC. and practices at Good Samaritan Hospital in Kearney, Nebraska. James D. Cuddeford, CUNA, MA, is program director of the Bryan Memorial Hospital/Univeristy of Kansas School of Nurse Anesthesia, Kansas City, Kansas. 375