Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
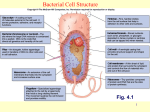
Microbiology 10.03.08 Antimicrobial Chemotherapy I Transcriber: Sheila Karst Morris 37:51 (Length of lecture) Slide 2 First of all we’re going to talk about major classes of antibiotics and how they work. How bacterial drug resistance develops, and I’m going to mention to you some aspects of antimicrobial resistance that is important in selected bacteria. Then we’ll finish with how resistant organisms are detected in the clinical laboratory. Slide 3 It’s important to know how to use the terminology properly. An antibiotic is an agent that can be naturally occurring partially or completely synthetic that selectively inhibits the growth of microorganisms at low concentrations. When the first antibiotics were discovered, these were compounds that were produced by a microorganism that inhibited the growth of other microorganisms. After the first discovery, it became obvious that you could modify the properties of naturally occurring antibiotics in the organic chemistry lab by synthesizing different molecules and side chains to attach to the basic structure to change their activity. Penicillin was discovered by Fleming in 1928, at that time the true penicillin only worked on gram + bacteria. It was found if you could put an amino group on the beta lactam ring you could enhance the activity against gram – bacteria. Amino penicillin, or ampicillin came into being to have gram – activity. We’re always looking for new targets in bacteria for antibiotics, because the bacteria are developing resistance. It’s important to distinguish an antibiotic from an antiseptic. An antibiotic is taken internally, an antiseptic is used externally, like iodine or alcohol or chlorhexidine on the skin to clean a wound or disinfect the skin. A disinfectant is something that you would use to destroy microbes on inanimate objects, like the table top. You would not put it on your skin, you would put it on your dental operatory or something like that, instruments, counters, etc. Slide 4 Going back 80 years now to the pre-antibiotic era, this was a big deal when Fleming first discovered penicillin, it opened the door to modern antibiotics. Slide 5 If we’re thinking about antibacterial drugs, there are lots of different antibiotics and families. The generic names, the trade names, you’ll become familiar with them in the clinic, or seeing patients on them, or ordering them. You can classify the antibiotics into a relatively few different mechanisms, by where they interfere with the metabolism of bacteria. In general terms you can see the different places that antibiotics work on bacteria will target things that are different for the bacteria than they are for humans. Prokaryotic cells are different from eukaryotic cells, for an effective drug to work on a bacterium you have to find something that it inhibits only in the prokaryotic cells, that’s not in the eukaryotic cell; otherwise you would kill your own cells. The first place it was discovered for antibiotics to work is on the cell wall. That’s how all of the betalactams work, on cell wall synthesis. If you can remember the bacteria have rigid cell wall that protects Microbiology: Antimicrobial Chemotherapy I Sheila Karst Morris pg. 2 them from osmotic lysis, it’s very important, gives them structural integrity. Without it, there’s not much left of them. The first groups of antibiotics developed interfered with the synthesis of cell walls, there are a variety of different ways they can do that. The names you need to be familiar with that act on the cell wall are listed in that part of the diagram: beta-lactam group (penicillin, cephalosporin, monobactam, carbopenams), phosphomycins, bacitracins, vancomycins, glycopeptides, and cycloserin. The ones that inhibit cell wall synthesis are the most widely used and important medically. Then you have agents that work on DNA replication. Bacterial DNA is transcribed into messenger RNA, mRNA translated into proteins. There’s a couple ways to interfere with this. Fluroquinolones and niadixic (?) acid actually interfere with DNA replication in the bacteria. They actually interfere with the enzymes that produce the supercoiling or that will cause the separation of new DNA once it’s replicated before it goes into the progeny. You can interfere with DNA replication earlier by drugs such as rifampin that inhibit DNA dependent RNA polymerase, the enzyme that transcribes DNA into RNA. You might say, why don’t those interfere with human cells? The DNA dependent RNA pol enzyme in bacteria is very different from that in humans. There’s no cross reactivity. A large group of drugs, including the macrolides, arythromycin, chloramphinocol, clindamycin, and tetracyclins, aminoglycosides that all act at the bacterial ribosome that inhibit protein synthesis. Then you have the group of drugs that actually interferes with cell membrane function, polymyxin and daptomycin. Finally we have the drugs that interfere with biochemical synthetic reactions for folic acid, metabolic inhibitors such as trimethoprim and sulfonamide. The cell wall, DNA, proteins and biochemical metabolism and the cell membrane, those are the 5 sites in the bacterial cell that you can interfere by using antibiotics. That’s pretty much what’s available now, any drug you have is going to work in one of those different places. Slide 6 How do we interfere with cell wall function? You have to understand what the bacterial cell wall is made of. Dr. Yother showed diagrams, the peptidoglycan which is an important part of gram + and gram – cell walls. It’s larger and thicker in gram +. If you look at the cell wall structure, you have carbohydrate chains, polysaccharides, which are the N-acetyl-Glucosamine and N-acetyl-Muramic acid that are in parallel chains. Then they’re cross linked by amino acids. We call this a penta-glycine bridge, with alanines hanging down off of carbohydrates, glycines attach them to the next chain. Only if you have this matrix/lattice work type arrangement here of the cell wall, that it will be rigid and form the cytoskeleton that the bacteria needs. If you don’t have cross linking you just have strands of carbohydrate that are not bound together in any way. This is where you have to look for the targets of the antibiotics. Slide 7 Beta lactams work because their structure, the “house” and the “garage”, the beta lactam ring typical of penicillin. The ring is common to all beta lactam drugs which include different agents shown here. You can of course change the spectrum of activity of the beta lactams by modifying the R group/side chain. Microbiology: Antimicrobial Chemotherapy I Sheila Karst Morris pg. 3 This is where the chemistry lab can attach other structures on there that will actually broaden the activity of the drug. The basic business part of it is right here, the beta lactam ring that resembles the amino acids. The alanine residues that cross link the cell wall. What happens is that you have what we refer to as penicillin binding proteins, the enzymes, carboxypeptidases, that actually string the amino acids together to cross link the carbohydrate chains in the cell wall. Remember, every time you’re putting molecules together you need an enzyme to catalyze the reaction. Normally the process takes place; the enzymes will recognize the alanine molecules and will attach to them and link them together to link carbohydrate chains. Penicillin, where bacterial cells are replicating, then enzymes mistake penicillin for their substrates, the alanines. They bind irreversibly to the penicillin, with enough penicillin the bacteria has no way to cross link its carbohydrates so the cell walls fall apart. It’s only good if the bacteria are replicating, penicillin won’t’ do anything to cells in the plateau phase; they must be dividing and growing. The cephalosporins, carbapenams, monobactams are different because they have something different attached at the R group. One of the ways that bacteria escape from beta lactams is that they make an enzyme, beta lactamase, which opens the ring by cleaving bonds. If you open the ring, you don’t have penicillin, you have peniciloic acid, a carboxylic acid, which no longer resembles the alanine; they don’t mistake it for substrate. Some of the newer drugs, beta lactamase inhibitor combination, one commonly used in an outpatient setting is augmentin. It’s amoxicillin plus clavulatic (?) acid, which inhibits the activity of the beta lactamase, so it protects the beta lactam drug from being broken down. Skip slides 8, 9 Slide 10 There are other drugs besides beta lactams that work on cell wall synthesis. It’s pertinent that you know a few and understand their mechanisms. Cycloserine is a drug that is sometimes used to treat TB. It’s not the first line, but since you have to use several drugs to treat because of high mutation rate and long length of time to treat, it’s pertinent to have cycloserine as a backup. Cycloserine inhibits the synthesis of the alanine molecules. To work and properly fit into the chains to connect the carbohydrates, you need the D isomers, the D-alanyl-D alanine. Cycloserine messes this up. Must have the D, not L isomer. It acts differently than the beta lactam. Another important drug is called vancomycin. It’s in the class referred to as glycopeptides, the biochemical type of drug it is. This is a very important drug for treating gram + bacterial infections. What this does is acts at the alanine molecules, where as penicillin bind the enzymes that would normally link the alanines together and cross link the cell wall, vancomycin bind to the substrate. It bind the alanine molecule itself so that the enzymes that want to cross link the side chains can’t get in there to it. Rather than binding enzyme, it binds to the cell wall substrates and blocks the transpeptidation reaction. It’s the drug to treat methicillin resistant S. aureus and other drug resistant infections. It doesn’t work on gram – bacteria, the molecule is too large to get inside the gram – cell wall. It works well for most gram + and kills them quickly. Microbiology: Antimicrobial Chemotherapy I Sheila Karst Morris pg. 4 Bacitracin we saw in the lab, it’s used to help identify group A streptococcus. Bacitracin also acts on the bacterial cell wall, it complexes with the lipid carrier that bring the cell wall precursors to the membrane. The wall is built outside of the cell membrane, the building blocks are the carbohydrates and amino acids, the things you have to put together are made in the cytoplasm. You need carrier molecules, lipids, which carry these things to the cell membrane so they can be put into the cell wall. Bacitracin actually binds up the lipid carrier molecules that would transfer the cell wall precursors; they can’t get to the outside to make to the cell wall. It’s another way to prevent cell wall synthesis. Isoniazid, INH, it’s the mainstay drug to treat TB. Because we treat TB for so long, the bacteria have a likelihood of mutating and becoming resistant, you must use several drugs. Then you can kill the resistant mutants so they don’t take hold and grow. INH actually inhibits components that are fatty acids and lipids, part of mycolic acid. It’s a big part of the cell wall in mycobacteria, they have a lot of lipid in the cell wall. Without mycolic acid, you don’t have a proper cell wall, INH inhibits its synthesis. Slide 11 There are a lot of drugs that act on the bacterial ribosome. You remember from biochemistry what happens, DNA is transcribed into mRNA, which is the genetic code/template for protein synthesis. You have to have proteins to synthesize structural proteins, enzymes to catalyze reactions. Bacterial ribosomes are different from eukaryotic ribosomes, that why these antibiotics do not do much of anything to eukaryotes. In the cell, the mRNA template determines the sequence of the amino acids (aas) with codons, each aa has it’s own particular code, the anticodon that matches up with the order of the base pairs in the mRNA. The aa’s know which order they’re put into, for proteins to work you must have the proper sequence of aas. The transfer RNA molecules actually bring the aas down there, to the mRNA. The two parts of the bacterial ribosome, the 30s and the 50s portions that come together with the mRNA in the middle, those two components are there, when tRNA brings an aa down there it recognizes the genetic code and sits there. The next one comes in, they’re spliced together, you have the enzyme peptidyl transferase that links the aas together at the ribosome. There are a lot of things you can do to inhibit these processes. Tetracyclins are drugs that are very important in the treatment of many infections, many gram +, pneumonia, rickettsial disease, mycoplasma, Chlamydia, many stds. We’re always concerned about tetracyclins, dentists know we don’t give it to children younger than 8 years old because it binds calcium and prevents development of enamel and causes the teeth to be permanently discolored dark yellow. It also interferes with bone development, you can’t give it to pregnant women or young children. The tetracyclins prevent the tRNA that brings the aa from attaching at the 30s ribosome. If you can’t bring new aas in to make a peptide, you can’t make a peptide. Aminoglycosides also act at the 30s ribosome. They include gentamycin, amacacin. They’re important drugs, they’re not given orally, must be given intravenously or intramuscularly. They’re important in treatment of gram – bacterial infections. They have no activity on anaerobic bacteria, but very good on enteric gram – infection. Topical gentamycin is an important component in ophthalmic solutions used Microbiology: Antimicrobial Chemotherapy I Sheila Karst Morris pg. 5 to treat conjunctivitis. They’re no longer very popular because we have other alternatives, they’re very good drugs but they do have toxicities. Some associated toxicities with gentamyacin, they can cause 8th cranial nerve damage: hearing loss, vestibular problems like dizziness. In addition to this they can be toxic on the kidneys. You must monitor renal function. If using them systemically, you must measure blood levels because they have a “narrow therapeutic index”, there’ s not that much difference in the amount to kill bacteria and the amount to get side effects. Aminoglycosides bind to the 30s ribosome and cause the inactivation of the initiation complex, the 30s and 50s ribosome together. They cause the mRNA to misread the genetic code, it can cause the wrong aa to be incorporated into the protein. In addition to this it causes the peptide being formed to fall off the ribosome, you have truncated/shortened peptides, with the wrong aas in them, they don’t do what they’re suppose to do. Oxizolidinones bind the 50s ribosome and prevent formation of the 50s/30s complex. Unless you have them together with the mRNA, none of this stuff takes place. We have one that’s used in the US, linasolin (?), a drug that’s used for gram + infections. It’s an alternative to vancomyacin for gram +. Streptogramins are not quite as widely used as other classes, but I put them here because of their mechanism of action. They bind the 50s and prevent peptide elongation and cause premature release. They do essentially what the aminoglycosides do, but they attack the 50s rather than 30s. Chloramphenicol and clendamyacin bind the 50s and inhibit peptidyl transferase. They actually prevent the peptide bond from ever being formed between the aas at the two tRNA. Chloramphenicol is rarely used, it was developed around 1950, it’s very good drug against anaerobic and a lot of gram + bacteria, but it had a lot of toxicity. It causes depression of the bone marrow, if you take it very long you can develop aplastic anemia, you quit making blood cells. Because of the side effect, and there’s so many other drugs, it’s hardly used. Clendamyacin is a very good treatment for anaerobic infections. It might be used to treat an infection in the oral cavity due to anaerobes, it’s used fairly often in many clinical settings. The macrolides include erythromyacin, azithromyacin (z pak), they’re very common drugs used orally for outpatient infections, especially respiratory (mycoplasma, Chlamydia). They bind at the 50s ribosome and actually prevent the tRNA that’s released it’s aa from turning loose the aa. If it can’t release it’s aa, it can’t go back and get another one, because tRNA is recycled. You tie up all the tRNA so you can’t bring in aa, you can’t make peptides. Slide 12/13 The two agents that are important that interfere with cell membranes are polymyxins and daptomycin. Polymyxins are active on gram -, they have kidney toxicity, not very pleasant drugs to use, but they’re good if the bacteria is resistant to other things. One of the ways they are used, in patients with pneumonia, olistin (?) is given through an inhalational system. The antibiotic is made into a nebulizer, the patient breathes it down into their lungs, that’s how it acts. It’s a fairly unique way to administer antibiotics. Microbiology: Antimicrobial Chemotherapy I Sheila Karst Morris pg. 6 Daptomycin is an important drug in gram + infections. Staphylococcus resistant to many drugs, daptomycin is an alternative. It interferes in a calcium dependent process, it opens channels in the membrane causing depolarization, it causes your K to leak out. It changes the K equilibrium between the inside and outside of the bacterial cell through depolarization of the cell membrane. The influx of K disrupts the cell membrane integrity and the bacterial cells die. It’s membrane depolarization and affects the movement of K in/out of the cell. Slide 14 The agents that interfere with DNA replication, rifampin is an important second line drug for treating TB, it’s often given along with INH. That’s the main place you would see it, because it prevents transcription of mRNA. Metronidazole is an old antibiotic, it’s used exclusively to treat anaerobic bacterial infections. It’s not known precisely how it works, it’s believed to damage DNA through metabolites that it produces through it’s metabolism. They somehow damage/denature DNA and cause bacterial cells to die, but only under anaerobic conditions. Slide 15 The quinolones are important drugs in the outpatient and hospital setting. Quinolones, there are several drugs in this class, ciphrofloxacin, levofloxicin, moxyfloxicin are the main three in the US. Ciprofloxacin is good against gram – and +, the other two are better against gram +. They have been around for about 20 years, there are new ones being developed. One of the main advantages of these is that they have a broad spectrum. Ciprofloxacinin is active against P. aeruginosa, important infections often resistant to many antibiotics. Many are getting resistant to them now. Quinolones act on the DNA, when DNA is replicated, it’s replicated from the parent strands, you have the supercoiling of the DNA, then you have to cut off the new DNA from the old DNA when the bacteria is dividing. They inhibit one or both of those reactions. Some inhibit supercoiling of DNA by DNA gyrase, some bind topoisomerase, the enzyme that cuts off new DNA. Slide 16 Then we have the antimetabolites, some of the first compounds developed. Sulfonamides and later trimethoprim. Folic acid is important in bacteria for production of DNA. Methyl groups are produced by folic acid, it’s an essential component for DNA replication. We get folic acid from our diet, so we don’t have to have folic acid produced. It’s necessary for blood cell and DNA development. Bacteria have to synthesize their folic acid. They cannot use it from the environment. They have to synthesize it from several different substrates, such as para amino benzoic acid (PABA). It happens that with sulfonamide, it’s similar to PABA, if you put sulfonamide into the system, it looks a lot like PABA. It binds to the teridine (?) and so you have this reaction down here, but you can’t get to folic acid because even though it looks like it, it doesn’t really work. You block the pathway and can’t get to folic acid. Another drug, trimethoprim inhibits a later reaction. It inhibits dihydrofolate reductase, part of the reaction to get the folic acid, one intermediate is dihydrofolate, you must reduce it to tetrahydrofolate, Microbiology: Antimicrobial Chemotherapy I Sheila Karst Morris pg. 7 that’s inhibited by trimethoprim. If you put them together into one pill, you inhibit folic acid at two different places, it works synergistically, better. That’s why we have a combination of trimethoprim and sulfonaminde. Bactrim or septra are common drugs to treat UTI and other infections due to many different bacteria. They have a broad spectrum and are very important drugs. Together they inhibit two different steps in folic acid metabolism. That is the completion of the brief overview of antibiotics and how they work.