Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
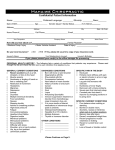
Loma Linda University Special Care Dentistry Health History Questionnaire (Confidential) 1. 2. Have you (has the patient) ever had any health problem in the past five (5) years?…………… Yes Have you (has the patient) seen a doctor (MD or DO) in the past five (5) years?………...… Yes No No 3. If yes, for what reason? Have you (has the patient) been in the hospital in the past (5) five years?……………………. Yes No 4. If yes, for what reason? Have you (has the patient) had a serious illness in the past five (5) years?…………………….. Yes No 5. If yes, what illness? Is there any activity your doctor says you (the patient) cannot do?……………………………. Yes No 6. If yes, what? Have you (has the patient) ever had a bleeding problem?……………………………………… Yes No Please circle the appropriate response for the following questions. He art/Blood Vessels Rheumatic fever……………. Rheumatic heart disease……. Heart valve damage………… Heart murmur………………. Congenital heart defect…….. Artificial heart valve………. High blood pressure………. Heart attack………………. T IA / Stroke………………. Heart surgery………………. Angioplasty………………. Vascular surgery…………. Pacemaker………………. Coronary heart disease……. Congestive heart failure……. Angina pectoris……………. Chest pain………………… Irregular heart beat…………. Rapid heart beat……………. Other heart / vessel disorder. Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Blood Blood clots or thrombosis… Yes Anemia…………………… Yes Sickle cell disease / trait…… Yes Hemophilia………………… Yes Bleeding disorder………… Yes Bruise easily for no apparent reason………… Yes Other blood disorder……… Yes Ne rvous System Epilepsy…………………….. Yes Seizure disorder……………. Yes Multiple sclerosis………….. Yes No No No No No No No No No No No No No No No No No No No No No No No No No No No No No No T rigeminal neuralgia……..… Yes Chronic pain……………….. Yes Anxiety/depression……….. Yes Alzheimer’s disease……….. Yes Dementia…………………… Yes Psychiatric treatment……….. Yes Psychological counseling….. Yes Persistent numbness/tingling. Yes Other nervous system disorder.Yes Head & Neck Glaucoma………. ………….. Yes Chronic sinusitis…………… Yes Injury to head, neck, face, teet h…………….. Yes Headaches………………….. Yes Unexplained visual change… Yes Frequent or severe nosebleeds………….. …….. Yes Persistent sore throat or hoarseness………..…….. Yes Difficulty swallowing…..….. Yes Other head / neck disorder..... Yes Endocrine Diabetes T ype I or II……….. Yes Low thyroid……………….. Yes Other thyroid condition……..Yes Cushing’s syndrome……….. Yes Parathyroid condition..…….. Yes Pituitary condition………….. Yes Other endocrine condition…..Yes No No No No No No No No No No No No No No No No No No No No No No No No No Musculoskeletal Sjogrens syndrome……….. Yes Arthritis…………………….. Yes Artificial joint…………….. Yes Fibromyalgia/rheumatis...….. Yes Chronic back pain………….. Yes Other bone/muscle disorder... Yes No No No No No No Respiratory T uberculosis……………….. Yes Asthma…………………….. Yes Chronic bronchitis………….. Yes Emphysema……..………….. Yes Persistent cough……...…….. Yes Cough up bloody sputum….. Yes Shortness of breath……..….. Yes Other respiratory……..…….. Yes Sleep apnea………………….Yes No No No No No No No No No Urinary Tract Kidney disease………. …….. Yes Renal dialysis………... …….. Yes Venereal disease……..…….. Yes Sexually transmitted disease.... Yes Other urinary disorder.…….. Yes Digestive System Hepatitis…………...……….. Liver disease……………….. Cirrhosis of the liver……….. Ulcers…………... ………….. Jaundice…………………….. Frequent heartburn…...…….. GERD………………... …….. Acid reflux Frequent nausea/vomiting Other digestive disorder Yes Yes Yes Yes Yes Yes Yes No No No No No No No No No No No No Cancer History Leukemia…………….. …….. Yes Benign tumors/growths…….. Yes Cancer……………….. …….. Yes If yes, what type: If yes, treatment: [ ] Surgery [ ] Radiation [ ] Chemotherapy [ ] Hormone therapy Other cancer………..…….. Yes Allergy History Are you allergic to or have you ever had a bad reaction to the following: Dental anesthetics…....…….. Yes Penicillin…………….. …….. Yes Sulfa drugs…………...…….. Yes Other antibiotics……...…….. Yes Aspirin………………. …….. Yes Latex products………..…….. Yes Metals / jewelry……....…….. Yes Other allergy……..…..…….. Yes Family History Has anyone in your family (grandparents, parents, siblings, children) ever had: Diabetes? ……………. …….. Yes No Heart disease? ……….…….. Yes No Depression/anxiety? ……….. Yes No T uberculosis? ………….. ….. Yes No Bleeding disorder? ……….... Yes No Anything else that runs in the family? ……….. Yes No No No No Miscellaneous Lupus erythematosus……..... Yes Organ transplant……………. Yes If yes, which organ? ……….. Yes Suppressed immune system.. Yes Persistent fever………..…….. Yes T aken steroids………..…….. Yes T aken prednisone / cortisone.Yes T aken prescription diet pills.. Yes If yes, which? [ ] Pondimin [ ] Redux [ ] Phen-Fen [ ] Other Use/used tobacco products… Yes Smoke……………….. …….. Yes No No No No No No No No No No No No No No No No No Chew tobacco…………..….. Yes Drink alcoholic beverages….. Yes If yes, how much? …..…….. Yes Used methamphetamines.…..Yes Used amphetamine or speed.. Yes Used cocaine or “crack” ..…..Yes Used other recreational drug..Yes Are you a recovering alcoholic or addict? ...…….. Yes O ther Down syndrome……………. Yes Developmental delay………. Yes Mental retardation…………. Yes Cerebral palsy……………… Yes Autism……………………… Yes ADHD……………………… Yes Combative / aggressive…..... Yes Self-abusive………………… Yes Surgical: VP shunt or revisions……. Yes Vagal nerve stimulator…… Yes Blood transfusion………… Yes No No Women O nly Are you pregnant? ……...….. Yes Is there a chance you could be pregnant? ……….. Yes Are you nursing (breast-feeding)? .…..…….. Yes How long? Circle the following drugs that you are (the patient is) taking or have taken Heart pills Oral contraceptive Antibiotics Nitroglycerin Steroids/Cortisone Antihistamines Digitals Hormones Cyclosporine A Aspirin Insulin T ranquilizers Blood thinners Diabetic drugs Sleeping pills Blood pressure T hyroid Antidepressants List all medications and doses that you are (the patient is) now taking: If you are not the patient, are you able to give legal consent for the patient? Relationship to patient Yes No If “No,” who does? Name of person able to give consent Signature of parent / guardian / person filling our form No No No No No No No No No No No No When? _________________________ How many packs per day? Name of person filling out form No No No No No No No Date No No No