Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
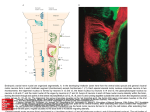
Anatomy Outline Test #1 Lec. 1: Intro CNS PNS Brain and SC, meninges (neurons and ganglia) Spinal nerves: 8 cervical, 12 thoracic, 5 lumbar, 5 saccral, 1 coccygeal ((31 pairs) SC: sensory neurons in dorsal root ganglion Axons, dendrites, ganglia Contains ANS- autonomic Nervous System o Parasympathetic: always on Vegetative fxns: respiration, peristalsis, HR, glandular secretion (homeostastis) Smooth muscles and organs only!! NONE in body wall or extremities!! Cranio-sacral outflow o Sympathetic Always off…unless fight or flight response HR, respiration, BP peristalsis, reproductive fxn, digestion Thoraco-lumbar outflor Somatic: 1 neuron o Efferent: controls striated/skeletal muscle (effects things) o Afferent: information from body wall and outside world into CNS (affects you) Visceral: 2 neurons (1 in CNS, 1 in ganglia in body) o No control over o Efferent: controls smooth muscle, glandular secretion o Afferent: info from organs and tissues into CNS Neuron Epineurium: surrounds bundle of fasicles Perineurium: covers fascicle (bundle of nerve fibers) Endoneurium: covers individual nerve fiber The Skull 3 parts of skull bones: o Outer table: very dense, hard bone o Diploe: spongy bone, soft, vascular (absorbs impact, distributes force) o Inner table: very dense, hard bone bone receives most blood from dural arteries (doesn’t heal well) Neurocranium: bony shell surrounding brain and meninges Viscerocranium: fascial skeleton, from pharyngeal arches Important Features o Pterion: “H” shaped, where parietal bone, frontal bone, sphenoid bone, and temporal bone come together Most vulnerable, middle meningeal a. underneath epidural hematoma o Mastoid Process: not on neonatal skull Calvarium, “skullcap” o 3 bones: Frontal bone Paired parietal bones Occipital bone o Coronal suture= “crown”, between frontal and parietal bones o Sagittal suture: between 2 parietal bones o Lambdoid suture= between occipital bone and parietal bones o Bregma: where parietal bones meet frontal bone *reference pt for surgery o Lambda: where parietal bones meet occipital bone Skull Issues o Fractures: depressed fracture (doesn’t require treatment), comminuted fracture, linear fracture, basilar fracture o “Coup-Countrecoup”- back of skull is broken, soft tissue bounces around The scalp o Layers= “SCALP” Skin, hair follicles Connective tissue (dense) Aponeurosis/ Epicranial aponeurosis (broad flat tendon between frontal and occipital belly of occipitofrontalis) Loose CT: fatty Pericranium: continueous w/ dura mater o Innervation Trigeminal nerve (CN V) Spinal Nerves Greater occipital (C2), Third occipital (C3), lesser occipital (C2,C3), greater auricular (C2, C3) o Arterial Supply Multiple anastomoses and tight CT heavy bleeding!! Overlap of carotids Coronal cuts worse (muscle pulls wound open) gaping Sagittal cuts don’t gape o Venous Return All drain to jugular vein Emissary Veins: connect skull veins and some penetrate scalp dural sinuses inside cranial cavity **important for infection inside brain from scalp wound= meningitis** o Lymphatics Many channels, FEW nodes Nodes in collar Lec. 2: Neural Development Part 1 Neurulation: 22-23 days Notochord induces neuroectoderm neural plate neural groove and neural folds neural crest and neural tube formation o Neural crest All sensory cells of PNS unipolar neurons of spinal ganglia (DRG) sympathetic trunks, sympathetic organ plexuses, pre-aortic ganglia schwann cells Neural canal (lumen of neural tube)- ventricular system, central canal of SC **rostral neuropore closes first (day 25) failure to closemeroencephaly/anencephaly **caudal neuropore closes second (day 27) failure to close spina bifida Microglia come from mesenchymal cells (in bone marrow) comapred to other neuronal cells Sulcas limitans: seperates alar from basal plate Alar Plate Cell bodies = dorsal gray horns afferent nuclei “alar=affarent”/sensory neurons Basal Plate Cell bodies= ventral gray horn and lateral gray horn Congenital Anomalies of SC: o Spinal dermal sinus (dimple) o Spina bifida occulta (tuft of hair) o Spina bifida cystica w/ meningocele w/ meningomyelocele (occurs w/ meroencephaly and craniolacunia (deficient development of calvaria) o Myeloschisis: most severe type of SB, SC left open (neural folds didn’t fuse) Brain Development o Head Fold Midbrain flexure, cervical flexure (demarks hindbrain from SC) Pontine flexture (thinning of roof of hindbrain myelencephalon and metencephalon) o Forebrain (prosencephalon) Telencephalon cerebral hemispheres (lat. Ventricles) Diencephalon thalamus, epithalamus, hypothalamus (3rd ventricle) o Midbrain (mesenchephalon) Mesencephalon Midbrain (Aqueduct) o Hindbrain (Rhombencephalon) Metencephalon Pons, cerbellum (4th ventricle) Myelencephalon Medulla Oblongata (4th ventricle) Choroid Plexus, CSF o Tela choroidea of 4th ventricle: pia mater + ependymal roof choroid plexus o Median and Lateral Apertures: absorption of CSF into venous system via arachnoid villi Midbrain o Neural canalcerebral aqueduct o Alar plate Neuroblast tectum colliculi o Basal plate neuroblast tegmentum of midbrain, substantia nigra? Forebrain o Closure of rostral neuropore, optic vesicles appear (primordial of retina and optic nerves) Diecephalon o From lat wall of 3rd ventricle o Thalamus, hypothalamus, epithalamus o Pituitary gland (hypophysis): ectoderm derivative *2 sources: hypophyseal diverticulum and neurohypophyseal diverticulum hypophyseal diverticulum contacts infundibulum(the neurohypophyseal diverticulum) pars anterior, pars tuberalis of pituitary gland results in adenohypophysis (glandular) or anterior lobe (oral ectoderm) and neurohypophysis (nervous part) or posterior lobe (neuroectoderm) as hypohyseal diverticulum stalk regresses, can get cysts (accessory anterior lobe tissue) Lamina terminalis: most important cerebral commissure (from one hemisphere to other) Corpus callosum connects neocortical areas Brain Anomalies o Cranium Bifidum: cranial meningocele, meningoencephalocele (meninges and brain), meningohydroencephalocele (brain w/ ventricular system) o Exencephaly: most of brain extrudes from calvarium o Anencephaly: common lethal, females ALWAYS associated w/ acrania, possible association w/ rachischisis, most common anomaly in stillborns Polyhydramnios o Microcephaly: calvaria and brain small, normal face size, genetic, environmental factors (premature synostosis- union of all cranial sutures) o Agenesis of corpus callosum o Hydrocephalus (depending on what canal is blockedwhat ventricles are enlarged) o Holoprosencephaly Severe, common, small forebrain (lateral ventricles fuse1 large ventricle)- eyes abnormally close together o Hydranencephaly Rare, hemispheres absent or membranous sacs, brainstem intact, head grows excessively after birth o Arnold-Chiari Malformation Most common involving cerebellum hydrocephalus tonguelike projection of medulla displacement of vermis of cerebellum though foramen magnum Lec. 3: Gross Brain, Meninges, Circulation, and SC Meninges functions: o supportive framework for vasculature and CSF o protection for brain and SC- suspended in CSF (bouyancy), and tethered by meninges Layers o Dura mater- Pachymenix (thick membrane) o Arachnoid and Pia mater- Leptomenix (slender membrane) Continous w/ one another Pia- directly adherent to brain, makes brain look shiny Dura Mater- outermost layer, tough, thick, collagenous membrane, only layer sensitive to pain o Cranial Dura Mater: adherent to inside of calvaria (suture lines, base) 2 layers tightly fused together (not separated by pathologies) Periosteal Layer (periosteum of skull) Meningeal Layer Pathologies can separate periosteum from bone (epidural/extradural space) Specialized Formations Venous sinuses o Endothelial lined spaces between periosteal and meningeal layers (normal seperation) o Collect blood from the brain Infoldings/Partitions/Septa: inward projections of meningeal layer at major brain fissures o Falx cerebri- divides cerebral hemispheres o Tentorium cerebelli- seperates cerebellum from cerebral hemispheres o Falx Cerebelli- divides cerebellar hemispheres o Diaphragma sellae- covers pituitary gland o Purpose: division of the cavity into compartments, restrict rotary displacement of brain Innervation CN V (trigeminal nerve) C2, C3: floor of posterior cranial fossa o Spinal Dura Mater Only 1 meningeal layer (not fused)- otherwise movable vertebra could tear SC) But technically, periosteal layer exists (separated by epidural space) Leptomeninges o Continuous, develop from single layer of mesenchyme o Pia mater: visceral part (covers organ) o Arachnoid mater: parietal part (adheres to dura mater) o Joined together by arachnoid trabeculae (tethers) o Continuous at roots of cranial/spinal nerves o Arachnoid Mater Inner lining of dura (via pressure) Cranial/spinal arachonid similar Not vascularized o Subarachnoid cisterns Radiological landmarks, CSF sampling sites (Cisterna Magna) o Pia mater Follows arteries into the cerebral cortex Highly vascularized Spinal Pia Thick Denticulate ligaments: anchors length of SC to dura mater (bilateral) Filum terminale: tethers cord to coccyx Meningeal Spaces Subarachnoid space- true space Subdural space and extradural/epidural space- not true spaces (only exists b/c of hemorrhage) Extracerebral Hemorrhages o Between the skull and brain o Subarachnoid hemorrhage: b/c of ruptured aneurysm (sudden BP causes rupture) Headache, stiff neck o Epidural/extradural hemorrhage: b/c of skull fractures, laceration of middle meningeal a. Initial LOC lucid interval (1-5 hrs) decline of consciousness o Subdural hemorrhage (between dura and arachnoid) b/c of head trauma, ruptures cerebral vein CSF Partial filtrate of blood, composition similar to plasma Functions: buoyancy, cushion, chemical stability Formed in ventricles (arise from embryonic neural tube) Choroid Plexus o Specialized ependymal cell protrusions into each ventricle (produce CSF) o Invagination of the tela choroidea (pia mater + capillaries + ependymal cells) into the ventricles CSF circulation o Lateral ventricles interventricular foramina 3rd ventricle cerebral aqueduct 4th ventricle median and lateral apertures subarachnoid space (continous w/ SC and cerebellum) o CSF returns to blood via arachnoid villi arachnoid granulations (large cluster) in dural sinuses Herniation of arachnoid mater thorough the meningeal layer of dura mater Only 1 layer of endothelium o Flow maintained by pressure of CSF, ependymal cell cilia, rhythmic pulsations of brain blood flow o Hydrocephalus Lec 4: CNS Vasculature Blood supply essential to brain function (brain ischemiaLOC loss of electrical activity irreversible damage) Blood Supply to Brain: o Internal Carotid A. (80% of blood to brain)- ant. And middle fossa Cervical part (arise in neck) via common carotid a. Petrous part of temporal bone (enters carotid canal) Cavernous part- crosses though cavernous sinus (in carotid groove)- emerges though dural roof Cerebral part o Vertebral A. (20%) – post. Fossa Enter skull though foramen magnum, merge together basilar a. Supply blood to post. Brain, branches brainstem Arteries of the Brain o Cerebral a. (3) Anteror cerebral a. –supply most of medial, superior surface of brain, frontal poles Middle cerebral a. – supplies lateral surface of cerebral hemispheres, temporal poles (via lateral sulcus) Posterior cerebral a. – supply inferior surface of brain and occipital poles o Cerebellar a. (3) Posterior Inferior cerebllar a. (PICA): largest branch off vertebral a. Anterior Inferior cerebellar a. (AICA): first major branch of basilar a. *Labyrinthine a. supplies inner ear Superior Cerebellar a.: last major branch of basilar a. o communicating a. (2)- Anterior and Posterior o Anterior choroidal a. Last branch given off by ICA Supplies Optic tract, choroid plexus of lat. Ventricle, and deep brain structures (CVAs) o Perforating A. – supply deep cerebral structures (key brain regions) Circle of Willis/Cerebral Arterial Circle o *Important anastomosis between A/P blood supplies to the brain. (although limited blood flow b/c of pressure) Watershed Zones o Areas of brain located btwn terminal distributions of adjacent a. (if BP, watershed zones lose blood flow) Blood-Brain Barrier o Function: seperates blood from brain b/c of it’s potential for harmful agents, and variable composition o o True BBB: microenvironment of neuronal fxn, protects Brain extra-cellular environment Formed by regular blood capillaries throughout brain (astrocyte foot providing tight jxns sealing endothelial cells, and a thick BM) Lipid-soluble substances (fats, gases, alcohol) can pass Ion regulation Blood-CSF barrier: protects CSF from blood All along arachnoid mater (via tight jxns) At choroid plexuses b/c true BBB absent (permeable capillaries) specialized choroid ependymal cells provide tight jxns Circumventricular organs b/c true BBB absent (around 3rd and 4th ventricles)specialized ependymal cells provide tight jxns Circumventricular organs sample blood b/c of leaky capillaries Venous drainage o cerebral veins dural venous sinuses basilar plexus of veins or internal jugular veins o 2 types of Valveless veins dural venous sinuses 1. Cerebral veins superficial deep: Vein of Galen (Great cerebral vein.) 2. Emissary Veins: connect from scalp to brain Lec. 5: Intro to Autonomic Nervous System **In CNS A collection of nerve cell bodies= nucleus bundle of nerve fibers that connect nuclei = tract **In PNS nerve cell bodies (1 or many)= ganglion bundle of nerve fibers+ supporting CT+blood supply = nerve CNS & PNS somatic and visceral divisions o 1 neuron between CNS and sensory eding/effector organ o afferent nerves: pain, pressure, movement of limbs, contraction of GIenter SC via dorsal roots (via sensory nerves) to brain via SC o efferent nerves: brain sends signals to initiate responses secretomotor to glands or muscle motor response actions generate sensory responses reflexes: shortcut from SC muscle motor response (bypass brain) SC cervical nerves # for vertebra below nerve all other nerves # for vertebra above nerve somatic or visceral fibers (carried by cranial/spinal nerves) o Somatic fibers General sensory afferent fibers (sensory): Extroceptive sensations (from skin, pain, and proproception from muscles, tendons, joints) General visceral efferent fibers (motor) Transmit impulses to skeletal muscles o Visceral fibers General visceral afferent fibers (sensory) Transmit pain or subconscious visceral reflex sensations from visceral organs to CNS General visceral efferent fibers (motor) Transmit impulses to smooth muscle and glandular tissues Pre-synaptic and post-synaptic fibers o Sensory fibers: pseudounipolar neurons (cell bodies outside CNS ganglia) o Motor fibers: multipolar neurons Cell bodies of somatic motor and presynaptic visceral motor neurons: gray matter of SC Cell bodies of post-synaptic motor neurons: outside CNS in autonomic ganglia fibers leave via vertebral foramen ventral/dorsal rootletsventral nerve root, dorsal nerve root (dorsal root ganglion) mixed spinal nerve ventral/dorsal primary ramus (mixed)motor/sensory nerve segmental innervation/distribution (myotomes/dermatomes) or peripheral nerve innervation/distribution (plexuses.) o dorsal roots- sensory afferent fibers from cell bodies in dorsal root ganglion (DRG)peripheral sensory endings and post. Horn of SC (gray matter) o Ventral roots- motor efferent fibers from cell bodies in anterior horn of SC gray mattereffector organs Dorsal/ventral roots- only nerves that can be cut (rhizotomy) for pain relieve/spastic paralysis o Dorsal Primary rami: Small portion of area on back o Ventral Primary rami: Everything else, trunk, arms, limbs Majority merge w/ adjacent anterior rami somatic nerve plexuses (multisegmental peripheral nerves) Autonomic nervous system (ANS) Motor fibers that stimulate smooth muscle, cardiac muscle, glandular cells 2-neuron system 1st presynaptic neuron in gray matter on SC o synapses w/ 2nd neuron in autonomic ganglia (fibers end in effector organ) sympathetic and parasympathetic always separate (originate in CNS but leave in different areas) Sympathetic o Fxns: Primary fxn: regulate blood vessels (vasoconstrict mostly) Pupil: keep wide (adapt to light) Speeds up heart rhythm Turns off peristalsis of stomach Turns of reproductive organ normal fxn o Fight or flight, catabolic system o Thoracolumbar o Release NE at post-synaptic neurons o Extend to innervate all body’s blood vessels reach all parts of body (except nails, cartilage) o Short pre-synaptic fibers (b/c ganglia are so close to SC) o Long post-synaptic fibers o Thoracolumbar outflow (white rami is only on T1-L2/L3) o Pre-synaptic neuron: 1 location: interomedial cell column (lateral horn) of T1-L2/L3 leaves SC though anterior root (motor)anterior ramiwhite ramus communicanssympathetic ganglion/paravertebral ganglion If innervating head, neck, body wall, limbs, thoracic cavity- 3 options 1. Ascend up sympathetic trunk, synapse w/ post synaptic neuron at higher paravertebral ganglia (via gray ramus communicans) 2. Descend in sympathetic trunk, synapse w/ post synaptic neuron at lower paravertebral ganglia 3. Immediately synapse w/ post synaptic neuron at that level If innervating viscera: Pass though trunk and paravertebral ganglia without synapsingabdominopelvic splanchnic nervepre-vertebral ganglionviscera or adrenal medulla…etc. o Post-synaptic neuron: 2 locations: Paravertebral ganglia (in sympathetic trunks/chains) Prevertebral ganglia/pre-aortic ganglia stimulates contraction of blood vessels, arrector muscles (goosebumps), sweating if innervating head, travels on cephalic a. branchcell bodies in superior cervical ganglion (close to vagus and carotid!!) if innervating viscera of thoracic cavity, travels on cardiopulmonary splanchnic n. pass though abd. Splanchnic n. pre-vertebral ganglia cardiopulmonary, esophageal plexuses Parasympathetic o Fxns: homeostasis/anabolic system Keeps pupil contracted Maintains normal heart rhythm Maintains normal peristalsis of stomach Maintains normal fxn of repro organs o Craniosacral o Release Ach at post-synaptic neurons o Long Pre-synaptic neurons Starts in brainstem Has to travel to ganglia in head or viscera o Short Post-synaptic neurons (b/c ganglia is in wall of viscera) Post synaptic neurons ALWAYS found in ganglia in PNS (head/visceral organs) o ONLY affect visceral structures (NONE in body wall or limbs)!! o Outflow (leave in 2 places) Cranial parasympathetic outflow Gray matter of brainstem, fibers exit CNS in CN III, VII, IX, X (3, 7,9, 10) CN III, VII, XI innervates head (4 ganglia) CN X innervates thoracic and abdominal viscera (most of GI) Sacral parasympathetic outflow Gray matter of SC, exit via anterior roots of S2-S4 and pelvic splanchnic n. Innervates pelvic viscera Blue Boxes o If cell bodies are intact when axons damagedpossible regeneration o Paresthesia: pressure on a nerve (pins/needles) o Crushing nerve injury: kills the axons, cell bodies intact, CT coverings intact regenertion o Cutting nerve injurysurgery o Anterograde degeneration: degeneration of axons detached from cell bodies (axon and myelin sheath) o Compression of vas nervorumischemia of nerveserious, usually permanent paresthesia Lec. 6: Gross Brain-Internal Lateral sulcus/Fissure of Sylvius : seperates temporal lobe from frontal and parietal Central sulcus: seperates frontal and parietal lobes Parietal, temporal, frontal opercula-forms opercular cortex, covers insula Lateral sulcus/Fissure of Sylvius : seperates temporal lobe from frontal and parietal Frontal Lobe Precentral sulcus Broca’s ephasia: punctuated speech, not coherent (motor) (Ventral) Orbital gyri: lateral to olfactory sulcus (contains Olfactory bulb, olfactory tract) Fxns:Voluntary movements, Executive fxns: personality, insign, forsight (gets inhibited when you drink/Thenias Gage) Parietal Lobe Language comprehension-Wernicke’s area- can say things but they are gibberish Other Fxns: spatial orientation, directing attention Temporal Lobe Fxns: emotional, olfactory processing complex aspects of learning/memory Wernike’s Area (language comprehension) Occipital Lobe o Visual Cortex Limbic Lobe Cingulate gyrus (emotional processing, depression) Fxn: emotional responses, drive-related behavior, memory White Matter Corpus Callosum White matter, communication between hemispheres Centrum Semiovale White matter, in dorsal core of frontal/parietal lobes, conveys neural impulses throughout cerebrum Internal Capsule (anterior and posterior limb, Genu) Brainstem All 3 areas contain tegmentum, “hood”: contains the brainstem nuclei (posterior in midbrain) Anterior to tegmentum: large ascending and descending tracts Tegmentum covered dorsally by tectum only in mesencephalon PAG Raphe Nuclei PAG: periaqueductal gray: important in descending pain control system Electrical stimulation of PAGameliorate pain Opium and derivatives (morphine) control pain by activating this network Endogenous ligands for opiate receptors (enkephalin and dynorphin) Friedreich’s Ataxia (problem w/ spinocerbellar tract) Inherited degenerative disease Lack of coordination in arms (intention tremor) and wide based, reeling gait (ataxia) Red Nucleus : coordinates muscle tone, body position, gait (lestion produces resting tremor, abnormal muscle tone, involuntary writhing) Pontocerebellar angle/Cerbellopontine Angle o Syndrome: most common neoplasms in the posterior fossa- most are benign (majority vestibular schwannomas (acoustic neuomas)). o SS secondary to compression of nearby CN V, VII, VIII o CN V involved loss of ipsilateral corneal reflex Reticular Formation Autonomic Reflex circuitry (inspiration, expiration, breathing rhythm, HR, BP) Hypothalamus- sympathetic control via IML column of SC Interuption: Horners Syndrome (Miosis, ptosis, enopthalmos) Projections from ARAS (ascending reticular activating system)- maintains consciousness/sleep wake cycle o If damaged bilaterally coma Type of Neuons Noradenergic Neurons o Locus Cerulus of rostral pons cerebral cortex Dopaminergic Neurons o in substantia nigra and VTA o 3 fiber streams Nigrostriatal/Mesotriatal (substantia nigracaudate and putamen) Mesolimbic: from VTA limbic structures Mesocortical: from VTAcerebral cortex o fxn: initiation of movement, motivation, cognition, pleasure, addiction o Parkinson’s disease o Antipsychotics used for Schizophrenia: blocks dopamine receptors Serotonergic Neurons o In raphe nuclei widespread innervation o Sleep/wakefulness, overall arousal o Descending pain control system o Antidepressants: enhance effectiveness of transmission of serotonin Cholinergic Neurons o Reticular formation, basal forebrain Substantia innominata: basal nucleus of Meyhert (forbrain cholinergic) o Forebrain activity lvl, sleep/wake, learning/memory Ach receptors Blood Supply to Brainstem Vertebral-basilar system Stroke syndromes: medial or lateral areas commonly affected Lec. 7: Spinal Cord and Nerve Roots (combined Paulman and Sarkos tract stuff) Tracts: axons that have same function (collected into bundles) Tracts terminating in brain=ascending, affarent, sensory tracts Tracts from brain to SC= descending, efferent, motor tracts Spinal Cord Basics Gray Matter o Anterior Horn: motor neurons o Lateral Horn: autonomic neurons (sympathetic or parasympathetic neurons o Posterior Horn: sensory neurons White Matter o Anterior Funiculus o Lateral Fasciculus o Anterior Funiculus Intrinsic Fascicles of SC: interneurons (intrinsic reflex pathways) Spinal Levels o Cervical enlargement, Lumbosacral enlargements- bigger ventral horns (b/c of motor neurons for the head/limbs) Spinal Nerves o Branches: Dorsal Primary Ramus posterior cutaneous n. medial and lateral branch Ventral Primary Ramus Lateral cutaneous n. and anterior cutaneous n. Spinal Vasculature o 2 arterial sources Vertebral a. 1 anterior and 2 posterior spinal arteries Get reinforcing contribution by segmental medullary arteries Great Anterior Segmental A. (of Adamkiewicz)- largest (reinforces 2/3 blood supply to SC) Radicular a. from regional arteries, supply nerve roots, peripheral parts of horns (do not contibute to spinal a. ) None of the a. supplying SC is sufficient to supply ENTIRE cord! (ischemia loss of portion of SC) Venous Drainage o Longitudinal veins ant. And Post. To cord connect to parallel veinsInternal vertebral plexus Spinal Sensory Pathways o Sensation Modalities Proprioception Mechanoreceptors Myelinated A and fibers Touch Mechanoreceptors Pacinian corpuscles Myelinated A- fibers Temp Thermoreceptors Myelinated A- and unmyelinated C fibers (slow, general temp sense) Pain Nocipceptors Myelinated A- fibers (fast) and unmyelinated C fibers (slow) Itch o Histamine Unmyelinated C fibers Mechanical Senses Proprioception, Touch (receptors in peripheral tissue)= DORSAL COLUMN TRACT/PCML TRACT Primary neuron in DRGenter cord via dorsal horn ascend up sC by dorsal column nucleus First synapse in brain stem – dorsal column nucleus @ medulla o Gracili nucleus o Cuneate nucleus 2nd neurons decussate to opposite side of CNS travel up brainstem via medial lemniscus VPN of thalamussomatosensory cortex **MS: damage to fasciculus cuneatus of C-spine: loss of proprioception/Asterogenesis (can’t describe objects w/ touch) “Protective Senses” Temp, Pain, Itch= ANTEROLATERAL PATHWAY** A for Anterolateral also stands for ASAP- decussates ASAP** Receptors in peripheral tissue (bare nerve endings) Primary neuron in DRG First synapse in dorsal horn of SC decussate via ventral commissure in SC Ascend in anterolateral columns Spinothalamic Tract o Originates and decussates in SC (transmits pain, temp, itch to thalamus) o spinal lemniscusVPN of thalamus o **Syringomyelia** (if central canal becomes enlarged, compresses fibers) o Causes selective loss of pain and temp in upper limbsfrequent burns (b/c no pain) Somatotopic Organization o Anterior Horn Medial columnsinnervate muscles of midline Lateral columnsinnervate muscles of trunk Contains motor nuclei o Posterior Horn (slender)- contains cell bodies of secondary sensory neurons (receive processes from spinal/dorsal root ganglion cells in specific/laminar layers) Brown-Sequard Syndrome o A spinal hemi-section o Axons in the dorsal column are ipsilateral o Anterolateral system: decussates as it ascends causes loss of pain, temp, itch (1-2 segments caudal to lesion) o Loss of mechanical sensations (proprioception, touch) @ level of lesion Spinal Motor Pathways Lateral Columns **typically contralateral, decussate in brainstem o Corticospinal tracts (LCS- CL)- lateral corticospinal= contralateral o **mnemonic: Cleopatra’s contralateral pyramids**- and her RED RUBYS Frontal cortex Decussates @ pyramids Primary motor pathway for major muscle movements Contralateral in the cord!! o Rubrospinal Tract **RED RUBIES* Cleopathra also has RED Rubies on her necklace (C-spine only!!) Red nucleus ventral horn of ONLY cervical spine Ventral Columns** typically ipsilateral, decussate in SC o Remember “IV” – ipsilateral ventral columns o Corticospinal Tracts o o o Motor cortex ventral horn of cervical and thoracic Ipsilateral in cord until terminal level Some decussate = bilateral Reticulospinal Tracts From medulla/Pons ventral horn Descent ipsilaterally down cord bilateral motor control Branches or has interneurons (spinal reflexes)- autonomic fxns Tectospinal Tracts Superior colliculusventral horn of c-spine (fxns in upper limb/neck) Tectum: visual movements/gaze Vestibulospinal Tracts Medial nuclei: head/neck position Lateral nuclei: ipsilateral (interneurons decussate) Corticobulbar tract* (mostly in head & neck) Primary motor cortexmotor nuclei in pons and medulla CN motor fxn Lec. 8/9: CN Nuclei for most CN (except CN I and II) are in brainstem or upper spinal cord CN IV comes off ventral side (not dorsal side) Motor and sensory usually NOT carried by same nerve CN I- Olfactory nerve (only have 1 nose)= SVA Olfactory Organ: contains cell bodies olfactory receptor neurons, possess fine olfactory cilia, surrounded by fluid by olfactory glands olfactory nerves though cribiform plate of ethmoid boneolfactory bulb synapse w/ Mitral cells axons of 2nd neurons form olfactory tract lateral and medial olfactory striae (distinct fiber bands) ONLY CN to enter cerebrum directly!! o Lateral striae temporal piriform complex o Medial striae though anterior commisure to other side o Temporal Lobe Epilyptic seizures (start smelling funny things before seizure) b/c of direct connection o Reflex vomiting- doesn’t get routed to cortex for interpretation (start throwing up b/c of smell) CN II- Optic nerve (2 eyes)= SSA Optic nerve and eye- direct extensions of developing brain Retinal receptor cells axons as optic nerves medial half of each retina deccusate in optic chiasm optic tracts terminate in lateral geniculate nuclei of thalamus visual cortex in occipital lobe Partial crossing of optic nerve fibers in chiasm- requirement for binocular vision, depth of field perception CN III- Oculomotor nerve: chief motor nerve to ocular and extraocular muscles GSE: somatic motor to 4 extraocular muscles, and levator palpebrae superioris (superior eyelid) o superior, medial, inferior recti, and inferior oblique o proprioceptive to these muscles GVE: parasympathetic motor to the sphincter pupillae and ciliary m. o Sphincter pupillae: constricts pupil (control light input) o Ciliary m: changes shape of lens (distance vision) o Primary neurons in Edinger-Westphal nucleus in midbrain Synapse in ciliary ganglion short ciliary n. eye muscles CN IV- Trochlear Nerve One fxn, one muscle GSE to superior oblique muscle Only CN to emerge from posterior/dorsal side of midbrain CN V- Trigeminal nerve/Sensory N. of Face Both deep and surface **CN VII and IX often hitch a ride with CN V (some branches of V carry different modalities) 3 divisions (all GSA fibers, each exit cranial volt though different foramen) V1: Ophthalmic n. above eye, forehead, temporal region, scalp, bridge of nose V2: Maxillary n. innervation to upper teach, nasal cavity o Trigeminal neuralgia (unbearable pain in face, b/c of pulsating a. running next to it) V3: Mandibular n.: lower teeth, also carries SVE muscles of mastication o ONLY CN V branch that has intrinsic motor fibers!! CN VI- Abducens nerve (Ab- 6 pack) One fxn, one muscle GSE to lateral rectus muscle (pulls eye outward) If damaged, will go cross-eyed CN VII- Facial Nerve Multiple modalities!! o SVE: facial expression muscles o GVE: parasympathetic to pterygopalatine and submandibular ganglia o GSA: small region posterior to ear o SVA: taste to anterior 2/3 tongue Exits CN vault w/ CN VIII 3 main branches: facial nerve proper, greater superficial petrosal n., chorda tympani nerve sensory geniculate ganglion in temporal bone (NO SYNAPSES b/c it’s a sensory ganglion!!) from facial nerve proper (SVE) (Two zebras bit my crotch) o Temporal o Zygomatic o Buccal o Marginal Mandibular o Cervical CN VIII- Vestibulocochlear nerve (8 looks like ear) Vestibular nerve: SSA fibers= equlibrium, motion (input from semicircular canals, utricle, saccule) o Ganglia in medulla medial to ICP Cochlear nerve: SSA fibers = sensory: hearing, sense sound vibrations (input from cochlea) o Ganglia in medulla lateral to ICP Innervates inner ear (neuroectoderm) CN IX- Glossopharyngeal nerve Multiple Modalities w/ numerous branches!! o SVA: taste to post 1/3 of tongue o SVE: 1 muscle- stylopharyngeus (gag reflex when touching tympanic membrane/Qtip) o GVE: to parotid gland (otic ganglion) o GSA: middle ear space, pharynx, post tongue and soft palate (trigeminal nucleus; gag reflex) Exits cranial vault with CN X and XI (and jugular bulb) Forms part of the pharyngeal plexus of nerves Carotid body: chemoreceptor (02, CO2) Carotid sinus: baroreceptor (measures BP) If damaged, problems adapting to BP CN X- Vagus Nerve Multiple Modalities!! (5) o GSA: lower pharynx, larynx, root of tongue o GVA: thoracid and abdominal organs o SVA: epiglottic taste buds o SVE: motor to soft palate, pharyngeal mm, laryngeal mm o GVE: parasympathetic to thoracic and abd vicsera in carotid sheath between jugular and carotid (super strong) in the neck: pharyngeal branch: SVE to pharyngeal mm superior laryngeal: SVE to 1 muscle, GSA to upper larynx, SVA (taste) to epiglottic region recurrent laryngeal: GSA to inferior larynx, SVE to rest of laryngeal mm. most below the neck (thoracid/abd viscera)- GVE parasympathetic CN XI- Accessory Nerve/Spinal accessory nerve One fxn, 2 muscles GSE to sternocladomastoid and trapezius muscles Nucleus in upper 5-6 segments of C spine arises from nerve roots Joined by branch of CN X while exiting skull CN XII- Hypoglossal Nerve GSE to 3 pairs of extrinsic tongue muscles and ALL intrinsic tongue muscles Hitches a ride with spinal nerves of C1, C2 Blue Boxes CN injuries: usually b/c of fracture at base of skull, movement of brain can tear/bruise CN CN 3, 4, 5, 6 prone to compression/injury related to pathologies of cavernous sinus Olfactory Nerve o Anosmia: loss of smell (URI, sinus disease, head trauma, aging) o Olfactory Hallucinations- lesion irritating the lateral olfactory area may cause temporal lobe epilepsy or uncinate fits Optic Nerve o Could be affected my demyelinating diseases (MS) o Optic Neuritis: lesions of optic n. diminution of viscual acuity o Visual Field Defects An optic nerve lesion blindness in temporal and nasal visual fields of ipsilateral eye Optic chiasm lesion bitemporal hemianopsia (loss of vision of one half of visual field in both eyes) Right optic tract at midline lesion left temporal and right nasal visual fields (contralateral homonymous hemianopsia) Most common type of vision loss, strokes Oculomotor Nerve o Ipsilateral oculomotor palsy (injury) o Compression: Extradural hematoma ipsilateral slowness of the papillary response to light (compresses superficial fibers first) Aneurysm of Posterior cerebral/Suerior cerebellar A. **stopped halfway though on blue boxes…sorry!*