Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
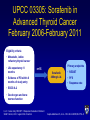
Advances in the management of iodine-refractory thyroid cancers Marcia Brose MD PhD Department of Otorhinolaryngology: Head and Neck Surgery Department of Medicine, Division of Hematology/Oncology Abramson Cancer Center The University of Pennsylvania Otorhinolaryngology: Head and Neck Surgery at PENN Excellence in Patient Care, Education and Research since 1870 MSB 05/30/09 Disclosure Elements – My goal is to present information on several agents currently under investigation for the treatment of advanced thyroid. As none of the agents other than doxorubicin and vandetanib and cabozantinib are FDA approved for the use in thyroid cancer, the rest of the new agents that will be discussed here are in clinical trials (not FDA approved) at this time. – Marcia S. Brose MD PhD DISCLOSURE: In the last three years I have financial interest/arrangement or affiliation with: Name of Organization Relationship Bayer Healthcare research funding, honorarium Onyx research funding, honorarium Novartis research funding, Exelixis research funding honorarium Astrazeneca consulting Bristol-Myers Squibb consulting Genentech/Roche research funding Thyroid Cancer: Clinical Pathology Papillary Follicular cells Differentiated Follicular Hurtle Cell Anaplastic Parafollicular cells Medullary Sporadic Familial American Cancer Society. www.cancer.org/docroot/CRI/content/CRI_2_4_1X_What_is_thyroid_cancer_43.asp. Carling T and Uldesman R. Cancer of the Endocrine System.: Section 2: Thyroid Cancer. Principles of Clinical Oncology. 7th edition. Lippincott Williams and Wilkins. 2005. MSB 05/30/09 Thyroid cancer in the United States 0-1.0cm 1.1-2.0cm 2.1-5.0cm Davies, JAMA 2006 295:2164 >5.0cm Differentiated Thyroid Cancer MSB 09/21/09 Thyroid Cancer: Treatment Strategy • High Risk: (Age >45, male, metastasis, extrathyroidal extension, >4cm) – Total Thyroidectomy – RAI (131I) Ablation – TSH Suppression Therapy with Thyroid Hormone – Follow Serial Thyroglobulin Levels (Tg) – XRT for recurrent local disease/positive margins – Surveillance: NeckUS, Tg, Neck MRI, Chest CT, RAI Whole body scan, FDG-PET MSB 05/30/09 RAI-Refractory Disease • 25-50% of Metastatic Thyroid Cancers loose ability to take up Iodine • This is attributed to down regulation of the Na+/ISymporter (NIS) and other genes of NaI metabolism –In other words, the cancer cells “forget” how to take up iodine and so they are immune to the treatment. MSB 05/30/09 RAI-refractory disease • Standard Chemotherapy has minimal efficacy. 1974 Doxorubicin became the only FDA approved drug for the treatment of advanced thyroid cancer. –No longer used because recent data shows response is 5% –High toxicity in patient with otherwise good QOL Cooper DS, et al. Thyroid. 2009;9:1176-214. Hodak SP, Carty SE. Oncology. 2009;23:775-6. Mehra R, Cohen RB. Hematol Oncol Clin North Am. 2008;22:1279-95,xi. Thyroid Cancer is associated with aberrant cell signaling MAP Kinase Genetic Alteration PTC FTC BRAF V600E 44% 0% BRAF copy gain 3% 35% RET/PTC (1 and 3) 20% 0% 8-10% 17-45% PI3KCA mutations 3% 6% PI3KCA copy gain 12% 28% PTEN 2% 7% Pax8/PPARγ 0% 35% >70% >65% PI3K/AKT RAS Total Nikiforov, Mod Path, 2008, Xing Endocrine Rel Ca(2005), Wang et al, 2007 Cell signalling in differentiated thyroid cancer Tumor Cell RET/PTC Endothelial Cell EGFR VEGFR-2 Ras B-Raf MEK ERK Ras PI3K Raf PI3K MEK AKT ERK mTOR AKT mTOR S6K • Growth • HIF1a • Survival • Inhibition of apoptosis • Proliferation • Migration S6K • Growth • Survival • Proliferation • Migration • Angiogenesis Graphic adapted from Keefe SM, et al. Clin Cancer Res. 2010;16:778-83. Targeting cell signaling in thyroid cancer Tumor Cell RET/PTC Motesanib Sorafenib Sunitinib Vandetanib XL-184 Endothelial Cell EGFR VEGFR-2 Vandetanib Ras B-Raf Sorafenib MEK ERK Ras PI3K AKT mTOR S6K Sorafenib Everolimus Sirolimus • Growth • HIF1a • Survival • Inhibition of apoptosis • Proliferation • Migration Raf PI3K MEK AKT ERK mTOR Axitinib Motesanib Sorafenib Sunitinib Vandetanib Everolimus Sirolimus S6K • Growth • Survival • Proliferation • Migration • Angiogenesis Graphic adapted from Keefe SM, et al. Clin Cancer Res. 2010;16:778-83. UPCC 03305: Sorafenib in Advanced Thyroid Cancer February 2006-February 2011 Eligibility criteria • Metastatic, iodine refractory thyroid cancer • Life expectancy >3 months Primary endpoints n=55 • Evidence of PD within 6 months of study entry Sorafenib 400mg b.i.d. • RECIST • PFS • Response rate • ECOG 0–2 • Good organ and bone marrow function b.i.d. = twice daily; RECIST = Response Evaluation Criteria In Solid Tumors; ULN = upper limit of normal Gupta-Abramson V, et al. J Clin Oncol 2008;26:4714–9 Phase III Study of Sorafenib in Locally Advanced or Metastatic Patients with Radioactive Iodine Refractory Thyroid Cancer (DECISION) trial Eligibility criteria • Locally advanced or metastatic DTC • Progression within 14 months • RAI refractory • No prior targeted therapy, chemotherapy or thalidomide Primary Endpoint: PFS (RECIST) Independent review Met primary endpoint January 2013 Randomisation (1:1) (n=380) • An International, multicentre, randomised, double-blind, phase III study of sorafenib versus placebo in locally advanced/metastatic RAI-refractory DTC Sorafenib 400mg orally b.i.d. n=190 Placebo n=190 Secondary Endpoints: OS, TTP, RR, DCR, PRO, PK Safety Exploratory Biomarkers Progression Investigator’s decision Crossover or continue sorafenib 400mg orally b.i.d. Off study Disease progression www.clinicaltrials.gov. NCT00984282 Targets of Kinase Inhibitors Compound Name VEGFR BRAF PDGFR KIT RET Other Sorafenib + + + + + FLT-3 Sunitinib + + + Axitinib (AG-013736) + + + Motesanib (AMG-706) + + + Pazopanib (GW786034) + + + Vandetanib + + EGFR Cabozantinib (XL184) + + C-MET Lenvatinib (E7080) + + FGFR + + FLT-3 + Summary • DTC is a vascular tumor that has been associated with increased activity of the MAPK pathways • Iodine-refractory patients have an average survival of 3 years • Phase III study of sorafenib in this patient population is positive. Results are expected at ASCO 2013. • Results of phase II trials with lenvatinib have led to the initiation of a phase III trials for patients with RAIrefractory DTC • Additional MKIs are also now in development many of which target VEGFR2, but also mTOR, MEK, and BRAF Advanced Thyroid Cancer’s New Unmet Need: Progression on Sorafenib/VEGFR2 inhibitor • Patients progress but maintain good performance status • Most patients respond then progress in a new lesion or a subset of lesions What to do? • We need additional treatment options Targeting cell signalling in thyroid cancer Tumor Cell RET/PTC Motesanib Sorafenib Sunitinib Vandetanib XL-184 Endothelial Cell EGFR VEGFR-2 Vandetanib Ras B-Raf Sorafenib MEK ERK Ras PI3K AKT mTOR S6K Sorafenib Everolimus Sirolimus • Growth • HIF1a • Survival • Inhibition of apoptosis • Proliferation • Migration Raf PI3K MEK AKT ERK mTOR Axitinib Motesanib Sorafenib Sunitinib Vandetanib Everolimus Sirolimus S6K • Growth • Survival • Proliferation • Migration • Angiogenesis Graphic adapted from Keefe SM, et al. Clin Cancer Res. 2010;16:778-83. UPCC 19309: Everolimus + Sorafenib for DTC patients who progress on Sorafenib alone Eligibility criteria • Metastatic, iodine refractory thyroid cancer • Life expectancy >3 months n=35 • PD on sorafenib Sorafenib + Everolimus Intra-patient Dose escalation Primary endpoints • RECIST • PFS • Response rate • ECOG 0–2 • Good organ and bone marrow function b.i.d. = twice daily; RECIST = Response Evaluation Criteria In Solid Tumors; ULN = upper limit of normal 22 patients accrued so far Primary Endpoint: Best Overall response Rate (BORR) (RECIST 1.1) (Partial and complete RR) in sorafenib naïve pts Independent review BRAF V600E testing Eligibility criteria: • Locally advanced or metastatic DTC • Progression within 14 months • RAI refractory Informed Consent NO25530: An Open-Label, Multi-Center Phase II Study of the BRAF Inhibitor RO5185426 in Patients with Metastatic or Unresectable Papillary Thyroid Cancer (PTC) positive for the BRAF V600 Mutation and Resistant to Radioactive Iodine + First Line Sorafenib Naïve (n=25) RO5185426 + BID Second Line Prior Sorafenib (n=15+) Secondary Endpoints: •PFS, TTP, OS, TTP, in sorafenib naïve pts •BORR, CB, TTP, PFS and OS, in soraefnib exposed patients Status: Accrual Complete Thyroid Cancer Therapeutics Program: Treatment Algorithm for Advanced DTC First Line: Sorafenib For PTC only: Second Line: VEGR2+BRAF+mTOR Third Line: Phase II – Add Everolimus or off label - Sirolimus VEGFR/MET/RET Inhibitors Personalized Pazopanib Cabozantinib BRAF V600E Inhibitor Phase II – vemurafenib ASCO 2012: Selumetinib: MEK inhibition to increase RAI uptake (Ho et al) Going forward as an earlier treatment: 1. Use for patients with high risk disease to increase uptake, 2. Unclear where in the treatment paradigm this will end up. Summary Second Line Agents • Due to tumor heterogeneity, a patient with progression on a multikinase inhibitor may continue to derive benefit from that inhibitor • Combination or Sequential treatments with MKIs (sorafenib + everolimus, or sorafenib + vemurafenib) are likely to aid patients with progression • New agents in development that specifically target mutations (BRAF V600E) may also play a role in the treatment of thyroid cancer in the first or second line settings and carry the most promise Medullary Thyroid Cancer MSB 09/21/09 Signaling pathways in MTC C-MET EGFR RET PKC RAS BRAF VEGF Tumor cell PI3K MEK AKT ERK VEGFR Endothelial cell PLC-g Multikinase inhibitor activities relevant to MTC Drug In vitro IC50 (nm) VEGFR 1 Sorafenib Vandetanib Cabozantinib (XL 184) VEGFR VEGFR3 RET RET/PTC3 RAF 2 Other - 90 20 49 50 6 PDGFR 58 1600 40 110 100 50-100 - EGFR 500 - 0.035 - 4.5 - - C-MET 1.8 Adapted from Sherman, J Clin Endocrinol Metab, 2009, p 1494 ZETA Study: Vandetanib Significantly Prolonged PFSa vs Placebo PFS: 65% Relative Reduction in Risk of Progression1 ▬▬ CAPRELSA 300 mg Events/Patients 59/231 Progression-free Survival 1.0 ▬▬ Placebo 41/100 Median PFS not reached 0.75 (95% CI: 22.6 months, nonestimable) 0.50 16.4 months median PFS 0.25 (95% CI: 8.3-19.7) HR=0.35 (95% CI: 0.24-0.53) P<0.0001 0.0 0 6 12 18 24 30 36 33 6 1 0 0 0 Months Number at Risk CAPRELSA 300 mg Placebo 231 100 173 47 145 30 118 24 CI=confidence interval; HR=hazard ratio. aPFS is defined as time from the date of randomization until the date of objective disease progression based on Response Evaluation Criteria In Solid Tumors (RECIST) assessment or death (by any cause in the absence of progression), provided death was within 3 months from the last evaluable RECIST assessment. 2 Centralized, independent blinded review of the imaging data was used in the assessment of PFS.1 1. CAPRELSA® (vandetanib) Tablets [package insert]. Wilmington, DE: AstraZeneca Pharmaceuticals LP. 2. Wells SA Jr et al. J Clin Oncol. 2012;30(2):134-141. 27 Cabozantinib Ph III in MTC Progression Free Survival by IRC 1.0 Probability 0.9 Cabozantinib Placebo 0.8 Median PFS (months) 11.2 4.0 0.7 1 year PFS 47.3% 7.2% 0.6 HR (95% CI) 0.28 (0.19, 0.40) 0.5 0.4 0.3 pp<0.0001 < 0.0001 0.2 0.1 0.0 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 Months Cabozantinib 219 121 78 55 31 12 2 Placebo 35 11 6 3 2 0 •111 Significant difference in tumor response rate – 28% in cabozantinib vs. 0% placebo; p<0.0001 • Median duration of response: 14.6 months ASCO 2012 oral presentation 1 0 Thyroid Cancer Therapeutics Program: Treatment Algorithm for Advanced MTC First Line: Vandetanib Cabozantinib Second Line: Cabozantinib Vandetanib Third Line/(First): Sorafenib Pazopanib Third Line: Sunitinib/Other? Summary: Agents for MTC • Phase II data shows that several multikinase inhibitors are clinically active in patients with advanced Differentiated and Medullary thyroid cancer. • Vandetanib was approved last year and Cabozantinib just received FDA approval for MTC • Response in these patients result in prolonged disease control • Additional agents are needed as these agents last only 10-12 months, there is a great unmet need to identify additional agents for this disease. Summary: Targeted therapy for Advanced Thyroid Cancer • Where do we go from here? – Completion of large randomized trials: • Phase III of sorafenib is positive. Phase III of lenvatinib is underway. – More data on the activity of the targeted agents used sequentially: • So patients are to benefit from the number of agents available – Novel strategies for treatment bear investigating: • including novel targets and the use of combination therapies to improve outcome.(Sor+Ev, Sor + Vem) – Further subgroup analysis to identify subpopulations: • use of clinical and molecular markers to identify patients that may benefit better with some therapies over others. Pts with Ras mutations, Poorly differentiated TC – Registration trial for sorafenib in MTC!!! Agents currently available in our Thyroid Cancer Therapeutics Program Agent Sub-types Vandetanib MTC, (DTC) Sorafenib DTC, MTC, ATC Everolimus DTC Pazopanib DTC Lenvatinib (E7080) DTC Cabozantinib (XL184) MTC, DTC Vemurafenib (PLX4322 – BRAF V600Ei) PTC Combretastatin ATC PLX3397 ATC MSB 10/16/10 University of Pennsylvania Thyroid Cancer Therapeutics Program • Brose Group – Carolyn Grande RN, CRNP – Steve Keefe MD – Thelma McClosky – Tatyana Kuznetsova, PhD – Waixing Tang MD – Stephen Stopenski • Thyroid Cancer Clinical Trials Unit – Larisa Zifchak RN – Parna Prajapati – Ramkrishna Makani – Jillilan Stanley • • Experimental Therapeutics Program – Andrea Troxel PhD – Peter O’Dwyer MD Pathology/Imaging – Michael Feldman MD PhD – Laurie Loevner MD • Thyroid Cancer Interest Group – Susan Mandel MD – Ara Chalian MD – Kelly Malloy MD – Douglas Fraker MD – Robert Lustig MD – Virginia LiVolsi MD – Zubair Baloch MD • MSB is a Damon Runyon-Siemens Clinical Investigator • Many Community Endocrinologists that have referred their patients, and the patients that have agreed to participate in our trials. Questions? Marcia S. Brose MD PhD Email: [email protected] Telephone: 215-615-6519 Thank you for your courage and attention! MSB 10/16/10