Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
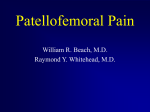
Four-dimensional CT analysis of Recurrent Patellar Dislocation –a 3D-3D Registration Technique Authors: Yuki Hoshi1, Satoshi Oki1, Ryuto Yoshida1, Yutaro Morishige1, Kengo Harato1, Masahiro Jinzaki2, Masaya Nakamura1, Morio Matsumoto1, Takeo Nagura3 1 Department of Orthopedic Surgery, Keio University School of Medicine, 2Department of Diagnostic Radiology, Keio University School of Medicine, 3 Department of Biomechanics, Keio University School of Medicine, Tokyo, Japan, Disclosures: Yuki Hoshi (N), Satoshi Oki (N), Ryuto Yoshida (N), Yutaro Morishige (N), Kengo Harato (N), Morio Matsumoto (N), Masaya Nakamura (N), Masahiro Jinzaki (N), Takeo Nagura (N) Introduction: Lateral patellar instability caused by medial patellofemoral ligament (MPFL) injuries has been considered to be pathology of recurrent patellar dislocation. However, little has been reported on its kinematic changes of the knee joint. The purpose of this study was to describe detailed kinematic changes of the tibia and patella in patients with recurrent patellar dislocation using four-dimensional computed tomography (4DCT) imaging. Methods: Five knees of 5 patients with recurrent patellar dislocation (mean age, 35.6 yrs; 5 females) were enrolled. As a control group, three healthy volunteers (mean age, 28.7 yrs; 2 males and 1 female) were enrolled. In the static position, CT scan of the both legs including whole length of the femur, patella, and tibia was performed. Dynamic 4DCT was performed using Toshiba Aquilion ONE (Toshiba America Medical Systems Corporation). In the CT gantry, the subject was positioned in supine position with the knee joint flexed in 60 degrees on a triangle pillow. The subject was asked to extend the knee to full extension in 10 seconds. Ten frames of CT volumetric data were obtained for one second. The effective radiation dose for 64-slice scanner would be approximately 1.7 mSv (170 mrem), compared with 0.5 mSv (50 mrem) for a single CT acquisition. This radiation dose has been justified by previous studies. This study was approved by our Institutional Review Board. The CT data of all frames and static whole leg CT were extracted as DICOM format. From the static CT DICOM data, surface data of the whole femur, tibia and patella were reconstructed. From 4DCT DICOM data, surfaces of the partial femur, tibia, and patella of all frames were also reconstructed. The partial femur surface of the knee joint surface in 4DCT was matched into the whole femur data in static CT by surface matching technique using iterative closest point (ICP) program in the software (VTK 5.10.0). Then the surfaces of the whole tibia and patella were matched into the matched partial tibia and patella surfaces of that frame. The motion of whole legs during the 4DCT exam was reproduced(Figure 1). In each frame, tibial rotation angles, patellar tilt, and patellar translation were calculated. Tibial rotation angles were calculated from the coordinate systems of the femur and tibia used in previous studies1. The distal half of the femoral shaft was fit into a cylinder, and the axis of the cylinder was defined as the femoral axis. The line between the medial and lateral epicondyle pointing the lateral side was defined as ML line. The femoral axis was defined as Y axis, the line perpendicular to the ML line and Y axis was defined as X axis. The Z axis was defined as the line perpendicular to X and Y axes. In tibia coordinate system, the tibial shaft was fit into a cylinder, and the axis of the cylinder was defined as tibial long axis (Y axis). The line between the posterior margin of the medial and lateral articular surfaces was defined as the ML line. As in the femur, the line perpendicular to the tibial long axis and ML line was defined as X axis. Z axis was defined as the line perpendicular to the X and Y axes. Tibial rotation angles were calculated from the Cardan (in z-x-y order) angle of the tibia coordinate system according to the femur coordinate system. The rotations around X, Y, Z were defined as varus/valgus, external/internal rotation, and flexion/extension, respectively (Figure2A). Patellar tilting angles were calculated from the norm of a plane fit into the patellar. (Figure 2B,C). Patellar translation was calculated by tracking the center of mass of the patella in the femur coordinate system (Figure 2D). In data analysis, each parameter at every 10° of knee flexion from 40° to 10° of flexion was calculated. Mann Whitney U-test was used to compare the dislocation and control groups. Results: In dislocation group, the patellar lateral tilt increased as the knee extended(Figure 3). In addition to lateral translation, patellar superior translation increased compared with the control group(14±3.4mm and 4.3±3.7mm at 10° of knee flexion:P=0.04). In control group, the tibia showed normal screw home movement. Namely, the tibia internally rotated during early phase of extension and externally rotated at the end phase of extension. On the other hand, in dislocation group, the tibia rotated externally in earlier phase of extension(internal rotation:-2.2±5.4° at 10°,7.9±0.3° in the control group: P=0.02). Discussion: The dislocation group showed superior patellar instability and tibial external rotation in addition to patellar lateral tilt. Given this result, not only does the medial support mechanism such as MPFL stabilize the patella in the patellar grove, but also changes the force vector of the quadriceps like pulley systems. Once the patellar medial support mechanisms were disrupted, the force vector changes laterally. This change externally rotates the tibia. Furthermore, the quadriceps need to pull the patella more proximally to achieve the full extension, like in the tendon bowing of the finger. Significance: In addition to lateral tilt, superior translation and superior tilt of the patella increased in patellar dislocation. Tibial external rotation increased and started in the early phase of knee extension, that is another pathology of patellar dislocation. References: 1) Grood ES, Suntay WJ. A joint coordinate system for the clinical description of three-dimensional motions: application to the knee. J Biomech Eng. 1983; 105(2):136-44. ORS 2017 Annual Meeting Poster No.2239