Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Lipomatous hypertrophy of the interatrial septum
Author(s)
Henrique Rodrigues; Paulo Donato; Nuno Neves; Cristina Marques
Patient
female, 52 year(s)
Clinical Summary
Authors describe a case of Lipomatous hypertrophy of the interatrial septum diagnosed by
MR. A mass in right atrium with 18cm2 was detected by echocardiography, and later MR
showed a homogeneous mass, with high intensity in T1 images and a decrease of signal
with fat-suppression.
Clinical History and Imaging Procedures
Our patient was a 52 years old female with a long history of cardiac congestive
insufficiency, diabetes type II, hypertension, hyperlipidemia, Pickwick syndrome, and a
very elevated body mass index (52 kg/m2). She went to hospital urgency with acute
exacerbation of cardiac insufficiency, on admission physical examination showed:
diaphoresis; dyspnea and taquipnea; bibasilar pulmonary crackles; hypotension (90/ 60
mmHg); arrhythmic pulse (frequency- 110); irregularity of S1 and S2; and extreme obesity.
ECG depicted atrial fibrillation with rapid ventricular response but with no ST
abnormalities. Laboratory data showed: anemia (Hg- 9,2mg/dl), hyperlipidemia
(246mg/dl); hypercholesterolemia (320mg/dl); hypoxemia (PO2 – 81mmHg) with
hypercapnia (PCO2 – 52mmHg) and oxygen saturation of 80%. Echocardiography made
immediately after arrival described a heterogeneous mass, measuring 18cm2, dependent of
right atrium wall, which could correspond to a thrombus, vegetation or tumour. Chest CT
with intravenous contrast (Fig 1), showed a filling defect in right atrium of low density,
without enhancement, that could correspond to adipose tissue. Cardiac MR was performed
thereafter: T1-Weighted TSE images showed a homogeneous high intensity mass with 7cm
dependent of septum and posterior wall of right atrium (Figs 2, 3, 4). T1- Weighted TSE
images with fat-suppression showed a decrease of signal in the mass (Fig 5). Cine MR
performed in different phases of cardiac cycle in sagittal view showed a mass in posterior
wall, with mobility. There were no hiposinal voids or turbulent flux in the right atrium near
vena cava confluence.
Discussion
Lipomatous hypertrophy of the interatrial septum was first described by Prior in 1964, it’s a
benign abnormality characterized by large fatty tissue deposits in the septum [1].
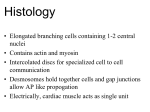
Microscopically, is characterized by a non encapsulated diffuse mass composed mostly of
mature lipocytes with interspersed hypertrophic cardiac muscle fibers [2]. The thickening
of the interatrial septum can be associated with obesity and increase in fat deposition with
advancing age [3]. Clinical manifestations range from cardiac irritability to obstructive
symptoms, and are related to the dimension of the lesion. A septal thickness of more than
3cm was combined with an incidence of supraventricular arrhythmias of more than 60%,
but only few cases of clinical relevant obstruction of the SVC can be found in the literature
[4]. Echocardiography, computed tomography and magnetic resonance imaging allow a
simple non-invasive diagnostic. TC can depict a mass with negative densities in the septum
and usually right atrium, which does not enhance after intravenous contrast. The MR
appearance is characteristic, showing on T1-Weighted SE images, high signal intensity
mass within the interatrial septum with the same signal intensity as subcutaneous fat. It has
the same signal as fat in other sequences such as T2-weighted SE and cine. If doubt
persists, fat-suppression techniques may help in demonstrating reduction of signal in the
mass as in subcutaneous fat [5]. Several other lesions can present as septal tumour mass:
myxomas, true cardiac lipomas, liposarcoma, parietal thrombi and metastatic tumours [6].
Surgical treatment is only required in cases of refratary arrhythmia and severe obstruction
of right atrium inflow tract.
Final Diagnosis
Lipomatous hypertrophy of the interatrial septum
MeSH
1. Heart Atria [A07.541.358]
The chambers of the heart, to which the BLOOD returns from the circulation.
2. Neoplasms, Adipose Tissue [C04.557.450.550]
Neoplasms composed of fatty tissue or connective tissue made up of fat cells in a
meshwork of areolar tissue. The concept does not refer to neoplasms located in
adipose tissue.
3. Heart Neoplasms [C14.280.459]
References
1. [1]
Prior JT. Lipomatous hypertrophy of cardiac interatrial septum. Arch Pathol 1964;
78:11-15
2. [2]
Fletcher CDM. Diagnostic histopathology of tumours, Vol I. New York: Churchill
Livingstone, 1995; 22-25
3. [3]
Shirani J, Roberts WC. Clinical, electrocardiographic and morphologic features of
massive fatty deposits (Lipomatous hypertrophy) in the atrial septum. J Am Coll
Cardiol 1993; 22:226-238
4. [4]
Reyes CV, Jablokow VR. Lipomatous hypertrophy of the cardiac interatrial septum.
A report of 38 cases review of the literature. Am J Clin Pathol 1979; 72:785-788
5. [5]
Didier D, Ratib O. Dynamic cardiovascular MRI- Principles and practical examples.
Stuttgart-New York: Thieme, 2003; 99-111
6. [6]
Burke AP, Litovsky S, Virmani R. Lipomatous hypertrophy of the atrial septum
presenting as a right atrial mass. Am J Surg Pathol 1996;20:678-685
Citation
Henrique Rodrigues; Paulo Donato; Nuno Neves; Cristina Marques (2005, Nov 22).
Lipomatous hypertrophy of the interatrial septum, {Online}.
URL: http://www.eurorad.org/case.php?id=4309
DOI: 10.1594/EURORAD/CASE.4309
To top
Published 22.11.2005
DOI 10.1594/EURORAD/CASE.4309
Section Cardiac Imaging
Case-Type Clinical Case
Views 32
Language(s)
Figure 1
CT
Fig 1- Chest TC with intravenous contrast shows a hypodense mass in right atrium without
contrast enhancement
Figure 2
MR
Fig 2 - T1-Weighted TSE image, in cardiac horizontal long axis, shows a mass with 7cm,
hyperintense, located in the right atrium and atrial septum.
Figure 3
MR
Fig 3 - T1-Weighted TSE image, in coronal view, depicts the hyperintense mass in right
atrium.
Figure 4
MR
Fig 4 - T1-Weighted TSE image, in sagittal view, showing the confluence of superior and
inferior vena cava in the right atrium. The mass does not cause any significant obstruction
at this level.
Figure 5
MR
Fig 5 - T1-Weighted TSE image, with fat-suppression, in coronal view, shows decrease in
signal intensity of the mass, like subcutaneous fat.
Figure 1
CT
Fig 1- Chest TC with intravenous contrast shows a hypodense mass in right atrium without
contrast enhancement
Figure 2
MR
Fig 2 - T1-Weighted TSE image, in cardiac horizontal long axis, shows a mass with 7cm,
hyperintense, located in the right atrium and atrial septum.
Figure 3
MR
Fig 3 - T1-Weighted TSE image, in coronal view, depicts the hyperintense mass in right
atrium.
Figure 4
MR
Fig 4 - T1-Weighted TSE image, in sagittal view, showing the confluence of superior and
inferior vena cava in the right atrium. The mass does not cause any significant obstruction
at this level.
Figure 5
MR
Fig 5 - T1-Weighted TSE image, with fat-suppression, in coronal view, shows decrease in
signal intensity of the mass, like subcutaneous fat.
To top
Home Search History FAQ Contact Disclaimer Imprint