Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Review
Advances in targeted therapeutic
agents
Nicholas C Nicolaides†, Philip M Sass & Luigi Grasso
Morphotek, Inc., Exton, PA, USA
1.
Overview of the targeted
therapeutic landscape
2.
Classes of TTAs
3.
Nucleic acid TTAs
4.
Target identification and
Expert Opin. Drug Discov. Downloaded from informahealthcare.com by Eisai Inc on 02/18/11
For personal use only.
selection
5.
TTAs in development
6.
Expert opinion
Importance of the field: The number of disease-associated protein targets
has significantly increased over the past decade due to advances in molecular
and cellular biology technologies, human genetic mapping efforts and information gathered from the human genome project. The identification of gene
products that appear to be involved in supporting the underlying cause of disease has offered the biopharmaceutical industry an opportunity to develop
compounds that can specifically target these molecules to improve therapeutic responses and lower the risk of unwanted side effects that are commonly
seen in traditional small chemical-based medicines.
Areas covered in this review: An overview of targeted drug therapies is presented in this review. We include a review of the various classes of targeted
therapeutic agents, the types of disease-associated molecules being targeted
by these agents and the challenges currently being encountered for the
successful development of these various platforms for the treatment of disease.
What the reader will gain: An understanding of the current targeted therapy
landscape, the discovery and selection of disease-specific gene products that
are being targeted, and an overview of targeted therapies in preclinical and
clinical studies. A description of the various targeted therapeutic platforms,
target selection criteria and examples of each are discussed in order to provide the reader with the current status of the field and emerging areas of
targeted therapy discovery and development.
Take home message: Novel medications are in demand for the treatment of
serious medical conditions including cancer, autoimmune, infectious and
metabolic diseases. Targeted therapies offer a way to develop very specific
treatments for serious medical conditions while concomitantly resulting in
little to no off-target toxicity. Targeted therapies provide an opportunity to
develop personalized medicines with superior treatment modalities for the
patient and a better quality of life.
Keywords: antibodies, antibody fragments, antisense oligodeoxynucleotides,
cell surface receptors, fusion proteins, genetic pathways, genetics, genomics, immunotoxins,
protein design, protein--drug conjugates, proteomics, RNAi, targeted therapies
Expert Opin. Drug Discov. (2010) 5(11):1123-1140
1.
Overview of the targeted therapeutic landscape
Targeted therapy is generally considered as the use of a compound that can specifically bind a disease-associated gene product and results in the suppression or activation of its biological activity thereby altering the disease state. In this broad
definition, targeted therapeutic agents (TTAs) may include small chemical entities
(SCEs), peptides, recombinant proteins, antibodies, antibody fragments and nucleic
acid-based agents. Targeted SCEs are mostly comprised of compounds that can
block enzymes, ion channels, cell surface proteins and transmembrane receptors.
Peptides and recombinant proteins include molecules that can target soluble
proteins, cell surface proteins/receptors and non-protein antigens. Antibodies and
10.1517/17460441.2010.521496 © 2010 Informa UK, Ltd. ISSN 1746-0441
All rights reserved: reproduction in whole or in part not permitted
1123
Advances in targeted therapeutic agents
Article highlights.
.
.
.
.
Expert Opin. Drug Discov. Downloaded from informahealthcare.com by Eisai Inc on 02/18/11
For personal use only.
.
.
.
Targeted therapies offer opportunity to generate
person-specific medicine; an overview of this area of
drug development is presented.
Targeted therapeutic agents include mAbs, antibody
fragments, bifunctional antibodies and recombinant
protein receptors; an overview of these various agents
is provided.
Protein immunotoxins have improved the therapeutic
activity of recombinant protein therapies.
Protein--chemotoxin conjugates provide another
alternative to improve the therapeutic benefit of
target-specific proteins.
Pathogenic targeting proteins offer a means of
discovering disease-specific targets and serve as possible
targeting agents; examples of this class are provided.
Nucleic acid targeting molecules represent one of the
most promising target-specific agents for therapy.
Disease-specific targets are the key for maximizing the
potential of targeted therapeutic agents; methods for
identifying and validating targets are discussed.
This box summarizes key points contained in the article.
antibody fragments are molecules that can specifically bind to
distinct regions (epitopes) on a protein or non-protein-based
molecule (antigen) and perturb its activity. Antibody-based
therapeutics contain immunoglobulin-type structures with a
protein backbone comprising of a variable antigen-binding
domain that provides target specificity and, in the case of
full length antibodies, a constant region (Fc) that can engage
with immune cells and/or immunomodulatory factors to
elicit immune-effector activity as a means to kill target cells.
Nucleic acid-based TTAs encompass short DNA or RNA
strands consisting of complementary nucleic acids that can
form double-stranded complexes with specific sequences
encoded by an mRNA within the cell that in turn results in
degradation of steady-state message and suppression of the
encoded protein. Nucleic acid agents include antisense
deoxyribonucleic acids and inhibitory RNA (RNAi), miRNA
and siRNA.
Experimental and clinical studies have demonstrated the
ability of several SCEs to be capable of targeting a biological
molecule based on its chemical structure; however, off-target
effects of the parent compound or metabolites have typically
resulted in side effects due to binding of homologous family
member proteins or non-related proteins, respectively, whose
function is critical for normal organ function and not
involved in the disease. Examples of these include the broad
spectrum tyrosine kinase inhibitors sorafinib and sunitinib
as well as the bcr-abl kinase inhibitor imatinib, which have
all demonstrated clinical activity and suppression of a focused
target kinase but have subsequently been shown to suppress
the biological activity of a larger class of kinase proteins [1,2].
Because of the inability of SCEs and/or their metabolites to
strictly bind one target, here we focus on TTAs that elicit their
1124
pharmacological activity via the ability to provide a more
stringent binding to a single target molecule while completely
avoiding metabolite-mediated side effects because of their
degradation into ubiquitous biological subunits (i.e., amino
acids or nucleic acids). This class of targeting agent includes
mAbs, antibody fragments, recombinant fusion proteins,
peptides and nucleic acid fragments.
Despite the complexity of manufacturing, antibody and
non-antibody protein-based therapeutics remain as some of
the most successful drugs in the marketplace. A representative sampling of therapeutic proteins, soluble receptor and
recombinant fusion proteins is shown in Tables 1 and 2,
respectively, which covers the diverse array of disease indications for which this class of therapeutic proteins are
approved. The development and application of proteinbased TTAs have significantly advanced since insulin, the
first recombinant protein, was successfully manufactured [3].
Therapeutic proteins continue to represent a high potential
for treating disease as numerous novel platform technologies
have been developed that are able to improve their expression titers, purification, stability and overall manufacturing
in addition to their pharmacokinetic and pharmacodynamic
profiles. Furthermore, the use of protein-based TTAs to
deliver small chemical compounds via targeting of cell
surface proteins that are exclusively expressed by diseaseassociated cells have expanded their pharmaceutical potential
by combining traditional SCE drug development expertise
with a target-specific delivery system [4]. The development
of conjugate-based targeting agents has especially created a
great deal of interest in oncology by the use of antibodies,
antibody fragments and fusion proteins to deliver toxic
payloads to malignant tissues. This approach offers the
opportunity of delivering cytotoxic compounds to tumors
while avoiding toxic side effects due to suppression of
targets involved in pathways important for normal tissue
function [5].
The development of compounds that can specifically
inhibit the translation of mRNA encoding for a diseaseassociated protein provides one of the most powerful applications of targeted therapy. Because these sequence-specific
compounds are capable of blocking the synthesis of specific
proteins whose function is needed to promote and/or maintain the disease state, mRNA targeting compounds offer the
potential for better efficacy and less toxicity in treating disease [6]. In light of these benefits, many years of research
have focused on refining the development and clinical application of antisense oligodeoxynucleotide (AS)-based therapies
and the more recent RNAi platforms, siRNA and miRNA.
Despite the many advances achieved in enhancing the utility
of this platform, several major hurdles still remain for these
agents to be able to specifically deliver intact nucleic-acid
compounds to disease tissues and elicit robust, long-term suppression of a disease-specific gene message for clinical benefit.
A review of these platforms and efforts to improve their
therapeutic use are provided in the sections below.
Expert Opin. Drug Discov. (2010) 5(11)
Nicolaides, Sass & Grasso
Expert Opin. Drug Discov. Downloaded from informahealthcare.com by Eisai Inc on 02/18/11
For personal use only.
Table 1. Approved recombinant proteins.
Protein class
Molecule (indication)
Trade name (company)
Recombinant erythropoeitin
Erythropoietin (anemia)
Recombinant insulin
Insulin (diabetes)
Recombinant HGH
HGH (growth disorders)
Recombinant ILs
IL-2*
IL-11z
GM-CSF (neutrophilsz)
G-CSF (neutrophilsz)
Epogen (Amgen)
Procrit/eprex (J&J)
Aranesp (Amgen)
Epogin (Roche)
Espo (Kirin)
Dynepo (Shire)
Novolog (Novo Nordisk)
Humalog (Eli Lilly)
Apidra (Sanofi-Aventis)
Humulin (Eli Lilly)
Lantus (Sanofi-Aventis)
Levemir (Novo Nordisk)
Genotropin (Pfizer)
Nutropin (Roche)
Norditropin (Novo Nordisk)
Humatrope (Eli Lilly)
Saizen (MerckSerono)
Serostim (MerckSerono)
Omnitrope (Sandoz)
Valtropin (BioPartners)
Proleukin (Prometheus)
Neumega (Pfizer)
Leukine (Bayer)
Neupogen (Amgen)
GRAN (Kirin)
Neutrogin (Roche)
Avonex (BiogenIDEC)
Rebif (MerckSerono)
Betaferon (BayerShering)
IntronA (MerckShering Plough) Roferon (Roche)
Pegasys (Roche)
Actimmune (Intermune)
NovoSeven (Novo Nordisk)
ReFacto (Pfizer Wyeth)
Recombinate (Baxter)
Advate (Baxter)
Kogenate (Bayer)
Helixate (CSL Behring)
BeneFIX (PfizerWyeth)
Recothrom (Zymogenetics)
Activase (Roche)
Actilyse (Boehringer Ingelheim)
Abbokinase (Abbot Labs)
Rapilysin/retavase (EKR Therapeutics)
TNKase (Roche)
Metalyse (Boehringer Ingelheim)
Streptase (ZLB Behring)
Recombinant CSFs
Recombinant INFs
Recombinant blood clotting factors
Recombinant plasminogen activators
INF-b1b§
INF-a2b{
INF-a2a#
INF-g 1b**
Factor VIIazz
Factor VIII§§
Factor IX{{
Thrombinzz
Alteplase##
Urokinase***
Reteplase##
Tenecteplase##
Streptokinase##
*Metastatic melanoma and renal cell carcinoma.
z
To enhance production of these cells after chemotherapy.
§
Multiple sclerosis.
{
Melanoma.
#
Hepatitises B and C.
**Chronic granulomatous disease and severe, malignant osteopetrosis.
zz
To aid in hemostasis.
§§
Control of hemorrhagic episodes in hemophilia A.
{{
Control of hemorrhagic episodes in hemophilia B.
##
Thrombolytic agent for treatment of myocardial infarction/stroke.
***Pulmonary embolism.
HGH: Human growth hormone.
Expert Opin. Drug Discov. (2010) 5(11)
1125
Advances in targeted therapeutic agents
Table 2. Approved fusion and soluble receptor recombinant proteins.
Generic name
Molecule (indication)
Trade name (company)
Etanercept
Abatacept
Soluble TNF-a receptor (treatment of inflammatory disease)
CTLA4--IgG fusion protein (treatment rheumatoid arthritis)
Alefacept
Rilonacept
LFA3--IgG1 Fc fusion (treatment of severe chronic plaque psoriasis)
Soluble IL-1 receptor--IgG1 Fc fusion (treatment of cryopyrin-associated
periodic syndrome)
Enbrel (Amgen)
Orencia
(Bristol-Myers Squibb)
Amevive (Astellas)
Arcalyst (Regeneron)
2.
Classes of TTAs
mAbs, antibody fragments, bifunctional
antibodies and recombinant protein receptors
Expert Opin. Drug Discov. Downloaded from informahealthcare.com by Eisai Inc on 02/18/11
For personal use only.
2.1
A number of recombinant proteins have been developed over
the years that can specifically suppress or replace the biological
activity/deficiency of an endogenous protein responsible for
promoting and/or maintaining human disease. A representation of the various classes of these proteins for the broad variety of disease indications they are used for is provided
in Tables 1 and 2. For the purposes of this review, we focus
on TTAs that can specifically bind and antagonize a soluble
factor, a cell surface protein or an mRNA target within a
disease-associated cell as well as provide an overview of
the types of TTAs that can specifically deliver cytotoxic
compounds via disease-specific cell surface proteins. This
last class of TTAs includes mAbs, antibody fragments, peptides, recombinant fusion proteins, protein--SCE cytotoxin
conjugates and nucleic acid-based therapies.
mAbs
Over the past decade, the use of therapeutic mAbs has
demonstrated significant success in specifically targeting
and suppressing the activity of proteins modulating diseaseassociated pathways [7]. mAbs have been shown to elicit their
pharmacological activity by a number of mechanisms. They
can bind and sequester soluble factors, thereby suppressing
the ability of these factors to interact with cell surface receptors or proteins that in turn activate biological pathways
within the cell. They can bind to pathogenic agents and
remove them from the patients’ system via clearance mechanism. mAbs can also bind to cell surface proteins of disease
cells and recruit immunological molecules such as complement or immune cells (macrophages, neutrophils or NK cells)
to specifically kill the mAb-bound cell via complementdependent cytotoxicity (CDC) or antibody dependent cytotoxicity, respectively. These mechanisms of action are referred
to as immune-effector function. There have been 30 mAbs
approved for treating a wide array of diseases including cancer, hematological and bone disorders as well as inflammatory
and infectious diseases. Table 3 provides an overview of
these mAbs and their approved indications. In addition to
these compounds, > 300 antibodies are in various stages of
development for a wide range of potential indications.
2.1.1
1126
A description of a subset of these development-stage antibodies being pursued across the different disease indications is
included in Table 4. While canonical full length IgG-type
mAbs have been the predominate antibody isotypes to achieve
clinical and regulatory approval, the pursuit of antibody therapies using IgM isotype and antibody fragment-based TTAs
has increased as these platforms have matured and offer additional therapeutic benefits. For example, the ability to deliver
robust target binding, specificity, unique epitope recognition,
enhanced tissue penetration and/or high efficiency immuneeffector activity in addition to the improved technologies
that support their scaleable manufacturing have all made
IgM and antibody fragment-based TTAs a reasonable alternative to IgG-based therapies. While it is generally understood
that IgMs have the ability to effectively kill antigen expressing
cells via the highly potent CDC mechanism, their broad pursuit as pharmaceutical products has been limited due to their
inherent low-binding affinities as well as the technical difficulties in scaleable cGMP manufacturing due to their large
molecular mass (> 750,000 kDa) [8,9]. Recent studies and
new technologies have enabled the advancement of IgM
development in light of the recognition that an IgM’s low
affinity-binding is offset by its high avidity, which is enabled
by the presence of 10 (pentameric IgM) or 12 (hexameric
IgM) antigen-binding domains, thereby providing good
targeting and disease tissue retention. In addition, new
manufacturing technologies have yielded cell-based systems
producing high titers of IgM under scaleable GMP
manufacturing conditions in quantities comparable to IgGs
as well as new analytical methods that have advanced the
characterization of these large biomolecular structures for
regulatory documentation requirements [10]. Due to these
major advancements and breakthroughs in technology and
with future success in clinical trials, the pursuit of IgMs as
bona fide TTAs, particularly for oncology indications, may
become more accepted by the biopharmaceutical industry [11].
Antibody fragments
Antibody fragment-based TTAs are molecules that are engineered to contain the antigen-binding site of an antibody
within a small scaffold thereby enabling the molecule to retain
target specificity as well as high-binding affinity. These
platforms, called fabs (fragment antigen-binding region
containing an antibody V region without the Fc domain),
2.1.2
Expert Opin. Drug Discov. (2010) 5(11)
Nicolaides, Sass & Grasso
Expert Opin. Drug Discov. Downloaded from informahealthcare.com by Eisai Inc on 02/18/11
For personal use only.
Table 3. Approved monoclonal antibodies.
Target
First approved indication
Generic name (manufacturer)
Anthrax toxin
a4 Integrin
CD11a
CD20
Anthrax inhalation
MS
Psoriasis
B-cell lymphoma
CD3
CD3 and EPCAM
CD33
CD52
Complement Ca5
EGFR
Chronic lymphocytic leukemia
Organ transplant rejection
Ovarian cancer ascites
Acute myeloid leukemia
B-cell leukemia
Paroxysmal nocturnal hemoglobinuria
Colorectal cancer
GPIIb/IIIa
HER2
IgE
IL-12 and IL-23
IL-1b
IL-2Ra
Squamous head and neck cancer
Ischemia
Breast cancer
Atopic asthma
Psoriasis
Cryopyrin-associated periodic syndrome
Organ transplant rejection
RANK ligand
RSV-F protein
TNF-a
Osteoporosis
RSV infections
Rheumatoid arthritis
VEGF
Crohn’s disease
Colorectal cancer
Macular degeneration
Raxibacumab (Human Genome Science)
Natalizumab (BiogenIDEC)
Efalizumab (Genetech)
Rituximab (Roche/BiogenIDEC)
Ibritumomab (Celldex)
Tositumomab (GSK)
Ofatumumab (GSK/Genmab)
Muromonab-CD3 (J&J)
Catumaxomab (Trion)
Gemtuzumab (Pfizer)
Alemtuzumab (Genzyme)
Eculizumab (Alexion)
Cetuximab (Eli Lilly)
Panitumumab (Amgen)
Nimotuzumab (Biocon)
Abciximab (J&J/Eli Lilly)
Trastuzumab (Roche)
Omalizumab (Roche)
Ustekinumab (J&J)
Canakinumab (Novartis)
Daclizumab (Roche/Sanofi-Aventis)
Basiliximab (Novartis)
Denosumab (Amgen)
Palivizumab (AstraZeneca)
Infliximab (J&J)
Adalimumab (Abott/Eisai)
Golimumab (J&J)
Certoluzimab (UCB)
Bevacizumab (Roche)
Ranibizumab (Roche)
RANK: Receptor activator of NF-kB; RSV: Respiratory syncytial virus.
scFVs (a single chain fab), domain antibodies, diabodies or
non-immunoglobulin protein domains that can be structurally altered to have antigen-specific binding, offer flexibility
in their use to develop small antigen-specific therapeuticbinding proteins or as conjugates linked to other scaffolds to
improve bio-distribution and/or pharmacology [12,13]. Several
types of antibody fragment technologies exist. These include
single domain antibodies derived from human variable heavy
chain or variable light chain domains (i.e., scFVs, dAbs) as
well as naturally occurring single domain antibodies that
are derived from shark or camelidae immune systems. An
advanced camelidae single domain antibody platform called
Nanobody technology has been applied broadly to develop
a number of therapeutic antibodies to a wide array of disease
antigens based on the need of obtaining good target penetration, which was not optimal using canonical tetrameric
mammalian-derived IgG type antibodies. These single chain
antibodies lack a light chain that is normally found within
most mammalian-derived antibodies yet retain the ability to
get high affinity and target specificity through a specific
spatial arrangement of the antigen-binding domain regions
on a single heavy chain backbone [14]. Preclinical experiments
have demonstrated the ability of nanobodies to bind to
therapeutic targets in regions not as accessible using IgG/
IgM type mAbs offering the ability to develop a broader
library of targeted agents depending on the need for maximal
target suppression. Finally, a more distinct antibody-like fragment platform that utilizes the ability of protein-binding
domains contained within host proteins such as fibronectin
(FN), T-cell receptors, ankyrins, and ‘A-domain’ (Figure 1),
has been manipulated to develop libraries of peptides with
altered amino-acid residues within their protein-binding
domains to generate target-specific fragments for therapeutic
use [15]. One such platform called adnectins has been developed that takes advantage of the inherent promiscuous
protein-binding properties that FN-binding domains contain.
Experimental data have shown that adnectins are capable of
being engineered to specifically target binding to a broad
number of antigens by altering amino-acid residues within or
flanking the FN-binding domain. This feature enables these
molecules to act in a manner similar to an antibody fragment,
concomitant with a low molecular mass. This combination enables the use of these compounds to target disease-associated proteins by tailoring the FN-binding domain to bind to certain
epitopes on a target antigen by in vitro engineering, which is
not possible using other antibody-based platforms that require
Expert Opin. Drug Discov. (2010) 5(11)
1127
Advances in targeted therapeutic agents
Expert Opin. Drug Discov. Downloaded from informahealthcare.com by Eisai Inc on 02/18/11
For personal use only.
Table 4. Therapeutic mAbs under development.
Generic name
Antibody target
Lead indication
Adecatumumab
Amatuximab
Belimumab
Bertilimumab
Blinatumomab
Briakinumab
Canakinumab
Catumaxomab
CDX-011 ADC
Cixutumumab
Conatumumab
CT-011
EB10
Elotuzumab
Farletuzumab
Figitumumab
Galiximab
Ipilimumab
J591 (111In)
Lexatumumab
Lucatumumab
Mapatumumab
MEDI-547
MNRP1685A
MORAb-004
MORAb-028
Ofatumumab
Olaratumab
Pritumumab
Robatumumab
Siltuximab
Telimomab aritox
Trastuzumab
TRC105
Tremelimumab
EPCAM
Mesothelin
LymphostatB
Eotaxin 1
CD19/CD3
IL-12 and IL-23
IL1-b
Epcam/CD3
GPNMB
IGFR1
Trail R2
PD1 receptor
FLT3
CS1 glycoprotein
Folate receptor a
IGFR1
CD80
CTLA-4
PSMA
Trail R2
CD40
Trail R1
EphA2
Neuropilin-1
Endosialin
GD2
CD20
Anti-PDGFR a
Vimentin
IGFR1
IL-6
CD5
HER2
CD105
CTLA4
Prostate cancer
Mesothelioma
Lupus
Allergic disorders
Lymphoma
Psoriasis
COPD
Ovarian cancer
Melanoma
Islet cell carcinoma
Breast cancer
Follicular lymphoma
AML
Multiple myeloma
Ovarian cancer
NSCLC
Hodgkin’s lymphoma
Melanoma
Prostate cancer
Pediatric
Hodgkin’s lymphoma
Non-Hodgkin’s
Multiple cancers
Multiple cancers
Multiple cancers
Melanoma
Follicular lymphoma
Ovarian cancer
Brain cancer
Ovarian cancer
Castleman disease
Graft rejection
Breast cancer
Prostate cancer
Bladder cancer
AML: Acute myeloid leukemia; COPD: Chronic obstructive pulmonary disease.
immune recognition and precursor backbones derived from the
host’s immune response [16]. Figure 1 reviews and provides a
schematic diagram of the various antibody and antibody
fragment technologies.
Bifunctional antibodies
In addition to the ability to generate smaller targetspecific binding proteins that can offer different advantages
over canonical IgG and IgM type mAbs, another use of
antibody fragment-based TTAs is the ability to engineer
them as a bifunctional antibody capable of binding to a
disease-associated target and a receptor on immune cells to
facilitate immune-mediated cell killing. Research has found
that antitumor responses and overall survival are highly correlated with the degree of inflammatory cells infiltrated into
tumors [17]. Hosts containing tumors that are infiltrated
with high numbers of T cells have been shown to have a longer overall survival and greater antitumor effects than those
lacking T-cell infiltration [18]. To enhance T-cell recruitment
2.1.3
1128
to tumors, an antigen-binding domain from one of the various platforms described above that can recognize a diseaseassociated protein is assembled with an antibody domain
that can bind to a T-cell receptor to form a bifunctional antibody that can bind target cells and recruit T cells via direct
T-cell receptor binding. Bifunctional antibodies can contain
or lack an Fc domain depending on whether macrophage
recruitment is desired. Several bifunctional antibodies have
been developed using this platform. The most advanced is
catumaxomab, an Fc containing bifunctional antibody that
recognizes the EpCam cell surface protein on tumor cells
and the CD3 receptor on T cells. This antibody has shown
the ability to suppress the growth of ascites in ovarian cancer
patients and is currently approved in Europe for treating ascites in patients with ovarian cancer [19]. Another bifunctional
mAb is blinatumomab, an antibody being developed for the
treatment of leukemia and lymphoma. This TTA is a nonFc containing bifunctional mAb that binds CD19 antigen
on malignant cells and CD3 receptor on T cells. Clinical
studies have shown it to have robust therapeutic activity in
cancers that do not respond to standard treatment. This class
of TTA adds yet an additional opportunity to leverage targetspecific binding molecules and the use of the host’s immune
system to fight against diseased tissues.
Antibody fragment-based TTAs represent one of the most
contemporary fields of research and development that can
complement traditional IgG and IgM mAb platforms to
improve on therapeutic efficacy of targeting antigens of new
and approved therapeutic antibodies. While antibody fragments have certain limitations such as short serum halflife and the inability to deliver immune-effector activity by
the natural mechanism, they have unique attributes when
compared to standard full length mAbs. Because of their small
molecular size, these antibodies offer some advantages over
standard antibodies including: i) the ability to penetrate tissue
and have access to epitopes that may not be accessible by larger
mAbs due to steric hindrance; ii) the ability to obtain better tissue penetration than the larger IgG/IgM-based mAbs; iii) a
shorter serum half-life than full length antibodies that depending on the preferential means of treatment maybe more advantageous and iv) competitive cost of goods due to manufacturing
using less expensive prokaryotic-based fermentation systems
which are still more cost-effective despite the vast improvement
observed in mammalian cell-based biological manufacturing.
While these features offer significant advantages, the ultimate
fate of these agents as valid therapeutics will depend on their
ability to deliver clinically meaningful outcomes in pivotal
clinical trials.
Recombinant protein receptors
Recombinant protein receptors that target soluble factors or
cell surface proteins have been shown in clinical studies to
be effective in treating a variety of diseases. This class of
molecules consists of a fusion between the ligand-binding
domain of a receptor and the constant region (Fc) of the
2.1.4
Expert Opin. Drug Discov. (2010) 5(11)
VH
/V
L
Nicolaides, Sass & Grasso
Mo
CL
no
y
od
iab
me
r
D
CH1–3
IgG
IgM
H
Vh
A-
do
bo
o
an
ma
in
dy
Expert Opin. Drug Discov. Downloaded from informahealthcare.com by Eisai Inc on 02/18/11
For personal use only.
N
Camelid Ig
Non-Ig domain
Figure 1. Top left: IgG is a hetero-tetrameric protein formed by two light chains (light green and red) and two heavy chains
(dark green and red). CL region; CH1-3, heavy chain constant domains. The VL and the VH regions pair up to form the
antigen-binding domain. In a ‘diabody’ (top middle), a VL/VH domain specific for one ligand (green) is assembled with a VL/
VH domain specific for another ligand (orange). Top right: a pentameric IgM is composed of five IgG-like structures
(monomer) linked together by disulfide bonds. A J-chain (not shown here) may be present to stabilize this multimer. Bottom
left: A camelid antibody is a homodimeric protein. Unlike an IgG, the camelid constant region (red) contains only two
domains, while the variable region (VhH, green) is represented by a single antigen-binding domain. If separated from the rest
of the molecule, a VhH domain forms a ‘nanobody’. Bottom right: An ‘A-domain’ contains ~ 35 amino acids including
6 conserved cysteine residues forming disulfide bonds (S-S). They occur naturally in some human receptors, including lowdensity lipoprotein-related proteins and are known to form various tandem repeat combinations binding > 100 different
natural ligands. A-domain shuffling technology allows deriving non-immunoglobulin domain molecules with new
ligand-binding specificities.
CL: Light chain constant; VH: Heavy chain variable; VL: Light chain variable.
immunoglobulin IgG1 protein which provides protein stability, improved systemic delivery and an anchor for purification
during manufacturing [20]. One of the most commercially successful recombinant protein receptors to date is etanercept
(Table 2), a fusion protein containing a ligand-binding
domain from the TNF-a receptor2 (TNFR) soluble receptor
fused to the Fc immunoglobulin region [21]. Etanercept
exerts its therapeutic action by sequestering the soluble
TNF-a inflammatory-associated cytokine, which in turn suppresses membrane-associated TNFR activity in inflammatory
cells and the inflammatory cascade underlying a number of
diseases, including rheumatoid arthritis (RA) and inflammatory bowel disease. Etanercept has been shown in numerous
clinical trials to be efficacious and has the ability to suppress
the aberrant immune cascade associated with inflammatory
disease and in turn improve patient health [22]. Other recombinant fusion receptor-based TTAs include abatacept, alefacept, aflibercept and rilonacept (Table 2). Abatacept is
approved for use in the treatment of RA in patients nonresponsive to disease-modifying antirheumatic drugs [23]. It is
a fusion protein consisting of the high affinity binding site
for the B7 co-stimulatory receptor expressed by antigen presenting cells (APCs) and the Fc immunoglobulin domain.
In host immune response, APCs interact with T cells via
antigenic presentation of processed proteins and interaction
of the B7 and CD28 co-receptors expressed by the APC and
T cells, respectively. Abatacept’s mechanism of action is to
block the ability of the CD28 protein to bind the
B7 receptor on APCs, which in turn suppresses immune cascades that underlie several inflammatory disorders including
RA. Alefacept is a fusion protein consisting of the
lymphocyte function-associated antigen 3 fused to the Fc
immunoglobulin domain. It has been approved for treatment
of patients with moderate to severe chronic plaque psoriasis
and functions by suppressing the activation of T cells via
binding to the CD2 T-cell surface protein thereby blocking
the ability of T cells to interact with co-stimulatory receptors
on APCs [24]. Aflibercept and rilonacept are fusion proteins containing cytokine receptor-binding domains for the
VEGF and IL-1 cytokines, respectively, fused to the Fc
domain. Aflibercept is being tested in Phase III clinical
studies for the treatment of neovascular diseases while rilonacept is approved for treating a subset of rare genetic autoimmune disorders [25,26]. Receptor fusion proteins have been
proven to be very effective in specifically blocking the biological activity of growth stimulatory/activation molecules.
While a subset of this class of TTAs have been mentioned
here, there are several others in development that are
Expert Opin. Drug Discov. (2010) 5(11)
1129
Advances in targeted therapeutic agents
specific for blocking ligands associated with a variety of
diseases (Table 5).
Protein immunotoxins
Another recombinant protein-based platform incorporates
the antigen-binding domain of an antibody or a cell surface
ligand fused to a cytotoxic protein (toxin) that when internalized via a cell surface receptor/protein is able to specifically kill
the host cell. An example of immunotoxin is denileukin diftitox, a recombinant protein consisting of the IL-2 cytokine
fused to the diphtheria toxin (DT) fragments A and B. On
binding to the IL-2 receptor on T cells, the compound is
internalized and kills host cells by DT’s ability to block protein translation via binding to the elongation factor eEF-2.
The drug is approved for treatment of cutaneous T-cell lymphoma and represents a class of toxin fusion proteins that
have demonstrated robust therapeutic activity in treating cancer [27]. A number of immunotoxins are currently being pursued in clinical trials to treat cancer, inflammatory and
infectious diseases (Table 6). Preclinical and clinical results
have shown promise in the ability of these TTAs to be active
in effectively eradicating disease-promoting cells whereby
non-toxin containing fragments were less effective. An example of an immunotoxin fusion protein is the SS1-P molecule
that contains a mouse IgG1 derived antigen-binding fragment
that is specific for the mesothelin tumor-associated antigen
fused to the Pseudomonas exotoxin PE38. Preclinical and clinical trials have shown the ability of SS1-P to specifically bind
and kill tumor cells expressing mesothelin [28]. While early
stage clinical studies have shown patient benefit, the broad
use of this agent has been limited by the highly immunogenic
nature of PE38 toxin in mammalian hosts thereby restricting
repeated administration. Efforts are being pursued to generate
less- or non-immunogenic PE38 toxin as well as other pathogens that can be potentially used for chronically treated diseases [29]. Other attempts at developing immunotoxins
include the use of antibody fragments that recognize
GP120 expression of HIV infected cells fused to either ricin
or PE38 toxins, and the BL22 antibody-immunotoxin that
targets CD22 and contains the PE38 toxin [30,31]. Clinical
studies of patients with relapsed/refractory hairy cell leukemia
have shown that single agent BL22 is able to elicit a 47%
complete response and a 25% partial response. A second generation BL22 is currently being developed with the goal of
creating an anti-CD22-immunotoxin fusion that has a higher
antigen-binding affinity to improve on efficacy and target cell
specificity. Immunotoxins are able to leverage the use of a
target-specific binding domain and a highly potent toxin to
selectively kill disease-associated cells while avoiding toxicity
in cells not expressing the antigen. In light of the positive preclinical and early-stage clinical results, interest in pursuing
immunotoxin therapeutic agents is increasing; however, hurdles still exist for the efficient development of this class.
Immunotoxins are highly toxic once internalized into a cell;
hence, developing molecules to cell surface antigens that are
Expert Opin. Drug Discov. Downloaded from informahealthcare.com by Eisai Inc on 02/18/11
For personal use only.
2.2
1130
expressed primarily on disease tissue is critical to avoid toxicities of normal cells. Another developmental challenge for this
class is the ability to develop an immunotoxin that can deliver
highly toxic effects to target cells but is not recognized by the
host’s immune system after long-term repeat dosing to avoid
drug neutralization. The refinement of these areas will
undoubtedly enable the expansion of this class of targeted
agent across various disease indications.
Protein--drug conjugates
Antibody and non-antibody protein-based TTAs have demonstrated pharmacological activity across a wide spectrum of
diseases; however, in most part, their effects in cancer and in
a subset of other disease types have been less than ideal for
delivering long-term clinical benefits to patients. One area
being actively pursued to improve TTA pharmacological
activity is the use of proteins (antibody and non-antibody)
conjugated to chemotoxins or radionuclides (Table 7). These
efforts aim to deliver highly cytotoxic chemical-based agents
or radioactive isotopes (radionuclides) to disease cells via
disease-associated cell surface antigens [32,33]. Technologies
that enable robust linkage of targeting proteins to cytotoxins
such as radionuclides, chemotherapeutic SCEs and nucleic
acid-based targeting agents have led to the establishment of
a variety of novel therapeutic approaches. The protein carriers
themselves have varied from full length antibodies to recombinant proteins and small polypeptides while different linkage
chemistries coupling cytotoxin to the protein carrier have
been implemented depending on where in the tissue it is
most desirable to have the cytotoxin liberated from the carrier,
if at all. The success of antibody conjugates using radionuclides, such as 90Y-labeled-ibritumomab tiuxetan and
131
I-labeled tositumomab, in treating refractory lymphoma
as well as the success of the chemotoxin-antibody conjugate
gemtuzumab ozogamicin support the concept of using a
targeting agent coupled to a cytotoxin to treat cancers and
other diseases in cases where nontoxin-conjugated biologicals have little therapeutic activity [34-36]. In the case of
the two radionuclide conjugated mAbs mentioned above,
both antibodies target the CD20 antigen, which is expressed
on B-cell lymphomas, and both were approved for use in
rituximab-refractory lymphoma. Rituximab is a chimeric
mouse-human IgG1 mAb directed to CD20 and approved
for treatment of B-cell lymphomas. Clinical studies using
these molecules showed a statistical improvement in patients
treated with these conjugates as compared to rituximab or
chemotherapy alone. While both are approved, their use in
clinical practice is limited due to the complexity of handling
radioisotope-labeled antibody before and after patient treatment. These limitations have fostered the generation of alternate molecules, including nonradioactive cytotoxins such as
calichaemycin, the cytotoxic molecule contained in the gemtuzumab ozogamicin antibody, as well as others that can be
effectively conjugated to an antibody, protein or peptide
targeting agent without affecting the pharmacokinetic or
2.3
Expert Opin. Drug Discov. (2010) 5(11)
Nicolaides, Sass & Grasso
Expert Opin. Drug Discov. Downloaded from informahealthcare.com by Eisai Inc on 02/18/11
For personal use only.
Table 5. Recombinant receptor fusion proteins under development.
Compound name
Ligand-binding domain
Disease indication
Target
Ref.
ActRIIA-IgG1
ActRIIB
Aflibercept
ALK1-Fc
APG101
Atacicept
Belatacept
Briobacept
FP1039
sEGFR501.F
YSPSL
Type II activin receptor IIA
Type II activin receptor IIB
VEGFR
Activin like receptor
CD95 receptor
TACI receptor
CTLA-4
BAFF receptor
FGFR
EGFR
PSGL-1
Anemia
Neuro-muscular disease
Angiogenesis cancer
Angiogenesis cancer
Glioblastoma multiforme
Lymphoma
Graft rejection
Rheumatoid arthritis
Cancer
Cancer
Delayed graft function
Activin
Myostatin
VEGF
GDF
CD95 ligand
BLyS
CD80 and CD86
BAFF ligand
FGF1, FGF2, FGF4
EGF
P-selectin
[91]
[92]
[25]
[93]
[94]
[95]
[96]
[97]
[98]
[99]
[100]
Table 6. Immunotoxins under development.
Immunotoxin name
Target
Disease indication
Toxin
Ref.
Anti-B4-blocked ricin
IL13PE
H22ETA
scFv35-ETA
Affitoxin
VB6-845
FR betaPE
26292(Fv)-PE38
SS1P
BL22
CD19-ETA
scFv(MUC1)-ETA
CD19
IL13Ra2
CD64
Acetylcholine receptor g
HER2
EpCAM
Folate receptor b
CD123/IL3Ra
Mesothelin
CD22
CD19
MUC1
Lymphocytic leukemia
Pancreatic cancer
Arthritis
Rhabdo-myosarcoma
HER2+ cancers
Various cancers
Inflammation
Acute myeloid leukemia
Lung cancer
Hairy cell leukemia
Lymphocytic leukemia
Breast cancer
Ricin
PE
PE
PE
PE
Bouganin
PE
PE
PE
PE
PE
PE
[101]
[102]
[103]
[104]
[105]
[106]
[107,108]
[109]
[28]
[31]
[110]
[111]
PE: Pseudomonas exotoxin.
Table 7. Protein--chemotoxin/radionuclide conjugates.
Compound name
Target
Disease indication
Chemotoxin/radionuclide
Ref.
Trastuzumab-DM1
Lorvotuzumab mertansine
PTX:C225
BT062
J591-111In
MAb 81C6
SGN-35
SGN-75
131
I-TM601
HER2
CD56
EGFR
CD138
PSMA
Tenascin C
CD30
CD70
Annexin A2
Breast cancer
Myeloma
Various cancers
Myeloma
Prostate cancer
Glioblastoma
Hodgkin’s lymphoma
Non-Hodgkin’s lymphoma
Glioma
Maytansinoid
Maytansinoid
Paclitaxel
Maytansinoid
Various isotopes
111
Iodide
Monomethyl auristatin E
Monomethyl auristatin F
131
Iodide
[39-41]
[112]
[113]
[114]
[115]
[116]
[43]
[117]
[53]
pharmacodynamic properties of the carrier protein (i.e.,
diminished ability to maximally access its target expressed by
the disease tissue).
In addition to the cytotoxic agents used in the commercially approved protein conjugates described above, two
chemotoxins that are being broadly pursued by biopharmaceutical companies developing protein conjugate TTAs
are the maytansine and auristatin microtubule disrupting
agents [37,38]. These molecules have both shown broad cytotoxic activity on mammalian cells; however, when conjugated
to a protein carrier these compounds lose their cytotoxic activities which is regained on liberation of intact cytotoxin. The
increased use of these agents has been swayed by the refinement of linker chemistries that provide greater stability of
the cytotoxin--protein conjugate in serum and effective
intracellular cytotoxin--antibody dissociation by cleavage of
Expert Opin. Drug Discov. (2010) 5(11)
1131
Expert Opin. Drug Discov. Downloaded from informahealthcare.com by Eisai Inc on 02/18/11
For personal use only.
Advances in targeted therapeutic agents
the linker in the highly reducing environment of the cell or by
intracellular enzymes, depending on the type of linker used.
While several antibody conjugates using these cytotoxins are
in various stages of clinical development (a few examples are
listed in Table 7), two of the most advanced therapeutic conjugates include trastuzumab-DM1 (T-DM1) and brentuximab vedotin (SGN35). T-DM1 is an antibody conjugate
comprised of the anti-HER2 antibody, trastuzumab, linked
to the maytansine derivative DM1 via a modified disulfide
linker that is resistant to reduction in serum [39]. The conjugate has been tested in a single arm Phase II clinical trial in
female patients with HER2-positive advanced breast cancer
whose disease has progressed after trastuzumab treatment,
and an average of six other chemotherapeutic regimens
including anthracycline, taxane and capecitabine. Results of
the study showed that approximately a third of patients
treated with T-DM1 had tumor regressions with limited toxicities [40]. Based on the positive outcome of this Phase II
study, the drug has recently been filed for marketing approval
with the US FDA while additional Phase II and larger
Phase III clinical studies are being pursued [41]. SGN35 is an
antibody conjugate consisting of a mAb that targets the cell
surface antigen CD30, which is overexpressed by Hodgkin’s
lymphoma cells and a subset of other hematologic cancers,
linked to an auristatin microtubule inhibitor. The linkage of
this conjugate occurs via a cathepsin protease sensitive substrate [42]. In the low pH intracellular environment, cathepsin
is a highly active protease that can cleave the conjugate linker
and produce a liberated active cytotoxic agent. This cathepsinsensitive linker is highly stable in the extracellular serum environment because of the presence of protease inhibitors and
high pH which significantly reduces cathepsin’s proteolytic
activity. In a SGN35 Phase I open-labeled study in patients
with relapsed or refractory Hodgkin’s lymphoma, 54% of
patients achieved an objective response, 39% of whom
exhibited a complete response. Clinical studies using the
non-conjugated anti-CD30 antibody had no objective responders, again demonstrating the ability of protein--cytotoxin
conjugates to increase therapeutic benefit [43]. As the use
of antibody--cytotoxin conjugates increases in development
and begins to deliver clinically successful results, it is likely
that more first generation compounds of this class will
be pursued.
As discussed above, antibody--cytotoxin conjugates offer a
great deal of promise in enhancing the therapeutic activity of
antibody or antibody-fragment-based TTAs. In light of the
improved therapeutic potential, a number of development
candidates are currently being pursued as first or second generation therapeutics [44]. Despite their therapeutic potential,
a number of challenges still remain for their clinical and
commercial success. The effectiveness of cytotoxin conjugates depends in part on the inherent features of the mAb
used as the targeting component of the conjugate. Less
desired properties of the mAb include: i) insufficient tumor
penetration; ii) relatively long serum half-life, which may
1132
lead to liberation of the cytotoxin in serum and higher side
effects; iii) limited ability of targeting epitopes within an
antigen that can support maximal conjugate internalization
and iv) technical challenges of universal, large scale conjugation of cytotoxins for GMP manufacturing at a reasonable
cost of goods. Smaller targeting proteins such as antibody
fragment platforms offer the ability to circumvent some of
these potential challenges in developing protein drug conjugates. Studies using antibody fragments have demonstrated
the ability of these agents to have better tumor penetration [45], preferred binding specificities [46] and lower
serum half-lives that may avoid prolonged circulation
and unwanted conjugate degradation in serum leading to
toxic side effects via organ accumulation. Furthermore,
smaller protein conjugates offer the ability to use alternative
manufacturing approaches to maximize success in cGMP
manufacturing by maintaining high quality production at
a reasonable cost of goods in contrast to mammalian cell
fermentation that is required for manufacturing fulllength mAbs. These factors need to be considered when
deciding to develop a protein--cytotoxin conjugate that will
probably be influenced by the nature of the disease, type of
antigen being targeted and market dynamics.
Pathogenic targeting proteins
Antibody and antibody fragment conjugate-based TTAs offer
many benefits for developing disease-specific therapies; however, a major drawback of using an antibody-based targeting
agent is the limited frequency by which a cell surface target
is expressed across a heterogeneous disease. In cancer, many
cell surface targets have been identified that appear to be
tumor-specific but the frequency of expression is quite variable from one tumor type to another thereby limiting the
breadth of which an approved antibody/protein--conjugate
TTA can be used across different cancer indications. The
identification of broadly expressed molecular targets that
are present on a diseased cell and not on normal tissues and
can be selectively targeted by a protein conjugate is limited.
Nevertheless, several disease-specific antigens have been identified as a result of epigenetic mechanisms, alternative splicing, gene rearrangement and overexpression that have been
targeted and been able to deliver robust clinical activity, supporting the notion that this class of strictly expressed target
exist and is important for maximizing the therapeutic potential of TTAs [47,48]. While efforts are currently being pursued
to identify more disease-specific targets using a variety of
genomic and proteomic discovery approaches (discussed
below), disease-specific targets have been identified by naturally occurring pathogenic agents that are able to bind to these
targets expressed on a broad class of normal and diseased cell
types. Research has shown that some of these naturally occurring agents are able to identify differentially expressed and
conformation-specific proteins that are not easily recognized
by nucleic acid or proteomic analysis nor may be easily
targeted using traditional protein/antibody approaches [49].
2.4
Expert Opin. Drug Discov. (2010) 5(11)
Expert Opin. Drug Discov. Downloaded from informahealthcare.com by Eisai Inc on 02/18/11
For personal use only.
Nicolaides, Sass & Grasso
The identification of targets and binding agents using natural
product screens from pathogenic organisms may provide
additional opportunities for effective targeting of molecules.
One source of natural proteins capable of binding to specific
mammalian cell surface proteins comes from the venom of
insects and reptiles. An example of this class is chlorotoxin,
one of several dozen proteins found in the venom of the Israeli
scorpion, Leiurus quinquestriatus. Screening of venom subunits identified proteins that were able to suppress the growth
of stimulated epithelial cells [50]. Subsequent analysis revealed
the ability of a 4 kDa peptide, later identified as chlorotoxin,
to have preferential binding to tumor versus normal cells.
Recently, molecular studies have identified that chlorotoxin
binds and internalizes into a wide range of tumor types via
annexin A2, a ubiquitously expressed intracellular protein in
normal tissues that is found expressed on the extracellular
membrane of transformed cells thereby giving it disease
specificity [51]. Preclinical studies have shown the ability of
chlorotoxin to deliver radionuclides, complex dyes, as well as
nanoparticles preferentially to tumor cells in vitro and
in vivo [52]. Synthetic chlorotoxin has been tested in clinical
trials and showed the ability to deliver conjugated 131I radionuclide to tumors via local and systemic delivery while no
detectable uptake was observed in normal tissues. The platform is currently being expanded to identify delivery of other
potential compounds to tumors for diagnosis and therapy
while the radionuclide conjugate strategy continues to be
advanced [53]. Other natural compounds have also been
shown to internalize on binding to cell-specific surface proteins. These proteins include vacuolating toxin A, which
enters human cells via sphingomyelin; hepatitis C viral coat
protein, which enters cells via claudin-1; and crotamine, a
toxin from rattlesnake venom that enters cells via heparan sulfate proteoglycans [54-56]. Natural proteins with broad diseased
cell-binding properties may enable shorter development and
target discovery timelines and offer the ability to treat a wider
class of disease indications due to the selected nature of a
pathogenic molecule to maximize its ability to penetrate its
infected host for propagation.
3.
Nucleic acid TTAs
Suppression of gene expression via knock down of mRNA
steady-state levels or suppression of translation offers some
of the most powerful opportunities to expand targeted therapy. Some examples of nucleic acid-based TTAs being developed across a differing spectrum of disease indications are
listed in Table 8. Early attempts to regulate disease pathways
by decreasing mRNA levels used antisense deoxynucleotide
(AS) that can bind to complementary RNA transcripts and
either block translation or decrease message via RNase H
mediated degradation [57]. While gene-specific suppression
has been proven in cell-based assays and in in vivo animal
models, recapitulation of AS effects in human clinical trials
has been unsuccessful [58]. Over the past 2 decades, enhanced
efforts have been used to create improved AS that are more
stable in serum, have enhanced cellular uptake and improved
intracellular mRNA targeting [59]. In addition, the discovery
of naturally occurring small RNAis has led to the development of the novel siRNA and miRNA platform technologies
for targeted therapy. The two most advanced nucleic acidbased TTAs to date are Vitravene, an AS to treat CMV retinitis, and mipomersen, an AS compound that targets
apolipoprotein B (apoB) to reduce low-density lipoprotein
cholesterol (LDL-C) levels in patients with high cholesterol [60,61]. The use of mipomersen as a single agent in a
Phase II clinical study showed its ability to suppress apoB
and lower LDL-C in all patients treated [61]. In addition to
this program, which is currently in Phase III randomized controlled clinical studies, over a dozen other antisense programs
are ongoing that target mRNAs encoding for proteins associated with cancer, cardiovascular, metabolic, neurodegenerative, inflammatory and infectious disease [62]. Many
development hurdles still exist in fully maximizing the therapeutic potential of nucleic acid-based TTAs. These include
further development of nucleic acid chemistries and carrier
strategies that can enhance the preferential accumulation of
nucleic acid fragments in disease cells versus normal, as well
as maintain sufficient steady-state serum and intracellular
concentrations for maximizing binding and suppression of
perpetually transcribed mRNA. Strategies to improve
stability by using phosphorothioated oligodeoxynucleotides
in which a non-bridging oxygen atom in the phosphate backbone is replaced by sulfur have proven to be effective in
increasing serum and intracellular stability. Additional technologies are being attempted to further improve serum stability, cellular uptake, target selectivity, reduced toxicity, while
maintaining support of RNase H activity for DNA--RNA
degradation [63]. Similar modification strategies are being
pursued with RNAi-based therapies to enhance stability and
pharmacokinetic profiles [64]. While improvements to the
nucleic acid moiety of these agents are needed, delivery to target cells also needs to be improved to help offset some of the
development hurdles listed above. In vivo studies using RNAibased therapies have shown off-target RNA suppression as a
result of inducing host immune responses which subsequently
alters gene expression in target cells as well as intracellular offtarget gene expression, again suggesting the need for better
nucleic acid TTA delivery [65,66]. Early attempts to address
nucleic acid delivery have used the lipid encapsulation methods as well as direct linkage to carrier proteins such as folate,
transferrin, somatostatin and antibodies to shuttle nucleic
acid fragments across the bilipid cell membrane through pathways that allow nucleic acid fragments to remain intact [67-70].
These studies demonstrated the ability to improve internalization in vitro; however, their therapeutic activity in vivo has
been equivocal. Several reasons may explain these results,
including uptake by receptor pathways expressed ubiquitously
among disease and normal cell types. Other reasons may
include conjugate instability in serum and intracellular
Expert Opin. Drug Discov. (2010) 5(11)
1133
Advances in targeted therapeutic agents
Table 8. Nucleic acid-based TTAs.
Compound name
Target
Disease indication
Nucleic acid platform
Ref.
Vitravene
Mipomersen
ISIS113715
OGX-011
AIR645
ALN-RSV01
QPI-1002
CMV
Apolipoprotein B
Protein tyrosine phosphatase-1B
Clusterin
IL-4Ra
RSV nucleocapsid protein
p53
CMV-induced retinitis
Cholesterol reduction
Type 2 diabetes
Cancer
Asthma
RSV infection
Acute kidney injury
PT antisense
PT antisense
PT antisense
PT antisense
PT antisense
siRNA
siRNA
[60]
[61]
[118]
[119]
[120]
[121]
[122]
oligonucleotide
oligonucleotide
oligonucleotide
oligonucleotide
oligonucleotide
Expert Opin. Drug Discov. Downloaded from informahealthcare.com by Eisai Inc on 02/18/11
For personal use only.
CMV: Cytomegalovirus; PT: Phosphorothioated; RSV: Respiratory syncytial virus; TTA: Targeted therapeutic agent.
trafficking of the conjugate that may result in sequestering the
nucleic acid in a compartment of the cell that prohibits its
ability to access and bind target mRNA [71,72]. Whatever the
reason for the observed discordance between in vitro and
in vivo studies, improving delivery and intracellular activity
of nucleic acid-based TTA will undoubtedly enhance the
overall therapeutic potential of these agents.
4.
Target identification and selection
Although TTAs with their ability to deliver molecules to cells
expressing disease-causing pathways promise the potential for
improving the treatment of a wide variety of diseases, important factors need to be considered in fully realizing their pharmacological potential. As discussed above, a major hurdle for
developing successful TTAs is the generation of targeting
molecules that can deliver robust pharmacological activity.
The other is developing TTAs to bona fide diseaseassociated targets that are exclusively expressed in the disease
versus normal tissues. Targets may include those that are
widely expressed in normal and disease tissues but in the disease state are more accessible to TTAs or are present in an
altered conformation or contain a different post-translational
form that may enable a TTA to specifically bind to the
disease-associated conformation that is absent in normal
cells [73]. An important factor to consider when searching for
disease-specific targets is selecting the method to be used to
identify and validate them. A number of approaches have
been used to identify disease-specific targets including differential RNA and protein analysis, immunological approaches
and genetic polymorphisms. Here, we discuss these platforms
and types of targets identified that may be suitable for
TTA-based strategies.
Methods for target identification
Several platforms and technologies have been used in an
attempt to identify targets suitable for disease-specific therapies. These include genomic-based technologies such as
microarrays, serial analysis of gene expression and RNA subtraction analysis that can identify differential expression patterns of mRNA in normal versus diseased tissues [74]. In
general, a good correlation exists between steady-state
4.1
1134
mRNA and protein levels; however, post-transcriptional
mechanisms and post-translational modification of proteins
have been shown to result in differential levels in diseased versus normal tissues [75]. In light of this caveat, proteinbased differential analysis has proven to be an effective
method for identifying disease-associated targets. In particular, proteomic technologies such as 3D electrophoresis
and quantitative mass spectrometry have been helpful in
identifying proteins whose overexpression is observed in the
disease state [76]. While target discovery via these platforms
have yielded a number of candidates that are being pursued
for targeted therapy, these techniques omit the identification
of proteins whose tertiary structures are modified to induce
disease-associated signaling [77]. These types of targets can be
best identified using immune-based systems that can generate
immunological reagents such as antibodies to identify aberrantly folded proteins whose altered structure may be associated with disease state but are not obvious using denaturing
or differential expression platforms. Immunological-based
platforms include the use of patient B cells to identify
those producing antibodies to antigens restricted to the
disease tissue, whole disease cell immunization of rodent
hosts and SEREX, a platform that utilizes the serological
analysis of recombinant complementary DNA to identify
humoral and cellular immune responses in patients with
disease [78-82]. These methods have led to the discovery of
many disease-specific antigens that are being targeted in
advanced clinical trials such as folate receptor a, mesothelin,
NY-ESO-1 and a number of other antigens whose diseaseassociated epitope may not have been found using traditional
large scale RNA/protein differential analysis methods. Finally,
in cancer, the identification of chromosomal regions that are
amplified or deleted as well as genetic loci that accumulate
point mutations or translocations offers the ability to identify
gene pathways that are involved in initiating, expanding or
maintaining the disease state. The use of altered genomic
information along with other platforms that measure altered
steady-state mRNA levels may help identify gene products
involved in supporting a disease phenotype. An example of
this would be the case whereby a disease-associated gene
product whose expression is only moderately enhanced in
the disease state versus normal is not obvious as a candidate
Expert Opin. Drug Discov. (2010) 5(11)
Nicolaides, Sass & Grasso
in contrast to gene products exhibiting dramatic increases in
expression in the disease versus the normal cell. However,
combining low overexpression with incidence of genetic
mutation may help flag a particular gene product as a
target candidate for therapy. These types of combined metaanalytical approaches may be beneficial in increasing the
list of ‘bona fide’ disease-specific targets which may often
be overlooked because of highly expressed gene products that are easily detected using large scale gene
expression technologies.
to deliver robust clinical benefit to patients. As discussed
here, traditional nucleic acid or proteomic analysis and pursuit of candidates based on the level of expression may not
always yield the best therapeutic target. Strategies that
incorporate expression profiling, evidence of disease involvement via genetic or genomic locus modification(s) in addition to biological validation will help in identifying targets
whose antagonism via TTAs may result in significant
clinical benefit.
5.
Expert Opin. Drug Discov. Downloaded from informahealthcare.com by Eisai Inc on 02/18/11
For personal use only.
4.2
TTAs in development
Selection of targets and criteria
Because of the plethora of disease-associated targets identified
using the garden of discovery technologies, it is crucial to have
available algorithms that can prioritize those that have a
higher probability of supporting the disease state. An ideal target is one in which its involvement in a disease is supported by
strong scientific rationale. The most definitive of targets are
those that are found mutated or containing a functional polymorphism that is highly correlative with and can recapitulate
the manifestations of a disease pathway in experimental systems. Targets of this class have been identified via genetic
mapping studies of families affected with a particular disease
and, in the case of cancer, by comparing genetic information
of malignant versus nonmalignant tissue [83,84]. Traditional
genetic mapping of affected kindred has led to the discovery
of several disease-associated targets that encode for intracellular and extracellular proteins. In cancer, several germline genetic mutations have been identified in genes that predispose individuals to cancer, including BRCA1, MLH1,
MSH2 and the RB1 genes. Unfortunately, most of these targets encode for inactivating mutations in proteins that are
intracellular and not accessible via protein-based TTAs.
A unique feature of cancer is the ability to isolate cells from
the transformed tissue and compare nucleic acid and protein
products in the tumor material from the normal tissue cells
using differential expression analysis and genomic technologies as described above. This approach has led to the identification of a number of gene targets that are mutated via point
mutation or translocation that in turn supports the disease
state [85,86]. Targets such as BCR-ABL, KIT, RAS and
PTEN have been identified by these methods. Again, most
of these targets encode for intracellular proteins which are
not easily amenable to non-SCE or protein-based TTAs, but
could be inhibited by nucleic acid-based TTA strategies.
Genetic mapping of other disease types has also led to the discovery of a handful of extracellular targets which are mutated
in the disease state and are amenable to therapy via a broader
array of TTAs. These include targets such as ACVR1, a
mutated cell surface receptor that causes constitutive signaling
in the rare genetic disease fibrodysplasia ossificans progressive,
a disorder that leads to ossification of muscle [87].
A combination of diverse target identification methods
coupled with validation strategies will aid in identifying ideal
disease-associated targets that can be manipulated by TTAs
Here, we present the use of TTA platforms in developing
novel therapies for treating a broad spectrum of diseases.
Monoclonal IgG1-type antibodies and recombinant fusion
proteins containing the receptor of a ligand have been the
most successful agents of this class to date. A number of preclinical and clinical stage compounds are currently being pursued using a variety of next generation targeting platforms as
discussed above. Tables 4 -- 8 provide a sampling overview of
TTAs from these various platforms being developed to treat
diseases across various therapeutic areas. The successful clinical development of one or more of these newer TTAs will
undoubtedly support their broader pursuit by the biopharmaceutical sector as companies attempt to deliver novel medicines to treat diseases with unmet medical needs. In
addition, with the new legislative challenges being placed on
healthcare, the need for showing potential patient benefit of
drugs is increasing as international regulatory agencies try to
limit the high costs of drugs in various healthcare reform initiatives. The implementation of TTAs will enable biopharmaceutical engineers in developing diagnostic tools that can be
used to predetermine whether a targeted pathway is intact in
patients selected to receive a particular TTA-based medicine.
Meeting these criteria will support the ability of novel TTAs
to receive approval and reimbursement that will help pharmaceutical companies recoup a portion of their R&D investment, and in turn deliver patient benefit and provide those
companies resources to support the development of additional
innovative drugs.
6.
Expert opinion
Targeted therapy offers the medical community and patients
an opportunity to vastly improve treatment and potentially
cure disease. This era of targeted biopharmaceuticals provides
an exciting time to leverage the combined information of the
human genome along with the number of novel drug discovery technologies to create innovative medicines that can specifically bind to a disease target and suppress its associated
pathway to relieve patients from morbidity and decrease
disease-associated mortalities. While the concept of targeted
therapy has been around for > 2 decades, the time to realize
the potential benefits of this class of therapy has never been
nearer. mAbs and other recombinant therapeutic proteins
Expert Opin. Drug Discov. (2010) 5(11)
1135
Expert Opin. Drug Discov. Downloaded from informahealthcare.com by Eisai Inc on 02/18/11
For personal use only.
Advances in targeted therapeutic agents
have paved the way for demonstrating how TTAs can
improve patient health. These TTAs have been developed
with the notion that a patient prescreen can identify those
that may benefit from targeted therapy. Two examples of
successful TTAs that use a patient prescreen to determine
therapeutic treatment are the HER2 screen of patients with
advanced breast cancer for treatment with Herceptin and
the identification of leukemia patients containing the
Philadelphia chromosome for treatment with Gleevec [88].
With the advent of new antibody fragment technologies,
nucleic acid-based TTAs along with the current mAb and
recombinant fusion protein therapies ongoing, the future of
personalized medicine is at the cusp of delivering promising
treatments in helping patients combat disease without the
risk of experiencing unwanted side effects that commonly
occur with chemical-based drugs [89]. As drug developers
gain more experience and insight into how these new
platforms perform as monotherapies or in combination therapy from analysis of large randomized controlled clinical trials, they will be able to further refine TTAs to make them
even more amenable for robust treatment. This experience
will be similar to the one that led to the refinement of
therapeutic mAbs as they evolved from a platform with
unproven therapeutic potential in the 1970s to one of
the most successful drug-based platforms in modern
medicine [90]. As in the case of mAb therapies, further optimization of next generation TTA platforms by engineering
features to improve target-specific delivery, optimal drug stability and robust manufacturing along with selecting bona
fide disease-associated targets via applying stringent criteria
(i.e., expression restricted to disease tissues, accessible by
TTA in disease state, target required to support disease cell
growth/maintenance, etc.) should support further developmental success of new compounds that have clinically relevant effects on the targeted disease. If these two conditions
are met, we believe that there will be a continuum of regulatory successes utilizing TTAs. Moreover, the pursuit of
TTAs will be further endorsed by the growing focus of international regulatory agencies whose priority is to support
affordable drug pricing of therapies that can show patient
benefit as well as exhibit good safety and efficacy results in
pivotal clinical trials. These criteria should be achievable
using TTAs, which by definition require the presence of a
target for therapeutic treatment.
Declaration of interest
NC Nicolaides, PM Sass and L Grasso are all employees of
Morphotek, Inc. NC Nicolaides is also a board member of
TransMolecular, Inc.
Bibliography
1.
2.
Wilhelm SM, Carter C, Tang L, et al.
BAY 43-9006 exhibits broad spectrum
oral antitumor activity and targets the
RAF/MEK/ERK pathway and receptor
tyrosine kinases involved in tumor
progression and angiogenesis. Cancer Res
2004;64:7099-109
Wang WL, Healy ME, Sattler M, et al.
Growth inhibition and modulation of
kinase pathways of small cell lung cancer
cell lines by the novel tyrosine kinase
inhibitor STI 571. Oncogene
2000;19:3521-8
3.
Johnson IS. Human insulin from
recombinant DNA technology.
Science 1983;219:632-7
4.
Trail PA, Willner D, Lasch SJ, et al.
Cure of xenografted human carcinomas
by BR96-doxorubicin immunoconjugates.
Science 1993;261:212-15
5.
Junutula JR, Raab H, Clark S, et al.
Site-specific conjugation of a cytotoxic
drug to an antibody improves the
therapeutic index. Nat Biotech
2008;26:925-32
6.
1136
Dimond PF. Making sense of antisense
and its rebound potential. Genet Eng
Biotech News 2009;11:1
13.
Jeong KJ, Mabry R, Georgiou G.
Avimers hold their own. Nat Biotech
2005;23:1493-4
14.
Revets H, De Baetselier P,
Muyldermans S. Nanobodies as novel
agents for cancer therapy. Expert Opin
Biol Ther 2005;5:111-24
15.
Binz HK, Amstutz P, Pluckthun A.
Engineering novel binding proteins
from nonimmunoglobulin domains.
Nat Biotech 2005;23:1257-68
16.
Azuma Y, Ishikawa Y, Kawai S,
et al. Recombinant human
hexamer-dominant IgM
monoclonal antibody to ganglioside
GM3 for treatment of melanoma.
Clin Cancer Res 2007;13:2745-50
Koide A, Bailey CW, Huang X, Koide S.
The fibronectin type III domain as a
scaffold for novel binding proteins.
J Mol Biol 1998;284:1141-51
17.
Vollmers HP, Brandlein S.
Natural IgM antibodies: the
orphaned molecules in immune
surveillance. Adv Drug Deliv Rev
2006;58:755-65
Li J, Hu P, Khawli LA, Epstein AL.
Complete regression of experimental
solid tumors by combination
LEC/chTNT-3 immunotherapy and
CD25+ T-cell depletion. Cancer Res
2003;63:8384-92
18.
Holliger P, Winter G. Diabodies:
small bispecific antibody fragments.
Cancer Immunol Immunother
1997;45:128-30
Bargou R, Leo E, Zugmaier G, et al.
Tumor regression in cancer patients
by very low doses of a T cell-engaging
antibody. Science 2008;321:974-7
19.
Shen J, Zhu Z. Catumaxomab, a
rat/murine hybrid trifunctional bispecific
monoclonal antibody for the treatment
7.
Nicolaides NC, Sass PM, Grasso L.
Monoclonal antibodies: a morphing
landscape for therapeutics. Drug Dev Res
2006;67:781-9
8.
Asakura K, Miller DJ, Pease LR,
Rodriguez M. Targeting of IgMk
antibodies to oligodendrocytes promotes
CNS remyelination. J Neurosci
1998;18:7700-8
9.
10.
11.
12.
Xing PX, Hu XF, Pietersz GA, et al.
Cripto a novel target for antibody-based
cancer immunotherapy. Cancer Res
2004;64:4018-23
Expert Opin. Drug Discov. (2010) 5(11)
Nicolaides, Sass & Grasso
of cancer. Curr Opin Mol Ther
2008;10:273-84
20.
21.
Expert Opin. Drug Discov. Downloaded from informahealthcare.com by Eisai Inc on 02/18/11
For personal use only.
22.
Vogel CL, Burris HA, Limentani S, et al.
A phase II study of trastuzumab-DM1
(T-DM1), a HER2 antibody-drug
conjugate (ADC), in patients (pts) with
HER2+ metastatic breast cancer (MBC):
final results. J Clin Oncol 2009;27:1017
41.
Genentech Submits Application to
FDA for Trastuzumab-DM1 in
Previously Treated Advanced
HER2-Positive Breast Cancer.
Genentech, press release; 7 July
2010. Available from: www.gene.com
42.
Doronina SO, Toki BE, Torgov MY,
et al. Development of potent monoclonal
antibody auristatin conjugates for cancer
therapy. Nat Biotech 2003;21:778-84
43.
Bartlett N, Forero-Torres A,
Rosenblatt J, et al. Complete remissions
with weekly dosing of SGN-35, a novel
antibody-drug conjugate (ADC) targeting
CD30, in a phase I dose-escalation study
in patients with relapsed or refractory
Hodgkin lymphoma (HL) or systemic
anaplastic large cell lymphoma (sALCL).
J Clin Oncol 2009;27:8500
44.
Senter PD. Potent antibody drug
conjugates for cancer therapy.
Curr Opin Chem Biol 2009;13:235-44
45.
Adams GP. High affinity restricts the
localization and tumor penetration of
single-chain Fv antibody molecules.
Cancer Res 2001;61:4750-5
46.
Hulahov A, Chester KA. Engineered
single chain antibody fragments for
radioimmunotherapy. Q J Nucl
Med Mol Imaging 2004;48:279-88
47.
Erickson HK, Widdison WC, Mayo MF,
et al. Tumor delivery and in vivo
processing of disulfide-linked and
thioether-linked antibody-maytansinoid
conjugates. Bioconjugate Chem
2010;21:84-92
Kavak E, Unlu M, Nister M, Koman A.
Meta-analysis of cancer gene expression
signatures reveals new cancer genes,
SAGE tags and tumor associated regions
of co-regulation. Nucl Acid Res; In press
48.
Smith LM, Nesterova A, Alley SC,
et al. Potent cytotoxicity of an
auristatin-containing antibody-drug
conjugate targeting melanoma cells
expressing melanotransferrin/p97.
Mol Cancer Ther 2006;5:1474-82
Sugawa N, Ekstrand AJ, James CD,
Collins VP. Identical splicing of aberrant
epidermal growth factor receptor
transcripts from amplified rearranged
genes in human glioblastomas. Proc Natl
Acad Sci USA 1990;87:8602-6
49.
Escoubas P, King GF. Venomics
as a drug discovery platform.
Expert Rev Proteomics 2009;6:221-4
50.
DeBin JA, Maggio JE, Strichartz GR.
Purification and characterization of
chlorotoxin, a chloride channel ligand
from the venom of the scorpion.
Am J Physiol 1993;264(2 Pt 1):C361-9
Peppel K, Crawford D, Beutler B.
A tumor necrosis factor (TNF)
receptor-IgG heavy chain chimeric
protein as a bivalent antagonist of TNF
activity. J Exp Med 1991;174:1483-9
Kreitman RJ, Wilson WH,
Stetler-Stevenson M, et al. Long term
results of BL22 (CAT-3888) in multiple
relapsed hairy cell leukemia. 52nd ASH
Annual Meeting and Exposition; 2009
32.
Vitetta ES, Krolick KA,
Miyama-Inaba M, et al. Immunotoxins:
a new approach to cancer therapy.
Science 1983;219:644-50
33.
Siegall CB, Chaudhary VK,
FitzGerald DJ, Pastan I. Cytotoxic
activity of an interleukin 6-Pseudomonas
exotoxin fusion protein on myeloma
cells. Proc Natl Acad Sci USA
1988;85:9738-42
Weinblatt ME, Kremer JM,
Bankhurst AD, et al. A trial of
etanercept, a recombinant tumor necrosis
factor receptor:Fc fusion protein, in
patients with rheumatoid arthritis
receiving methotrexate. N Engl J Med
1999;340:253-9
24.
Lebwohl M, Christophers E, Langley R,
et al. An international, randomized,
double-blind, placebo-controlled
phase 3 trial of intramuscular alefacept
in patients with chronic plaque psoriasis.
Arch Dermatol 2003;139:719-27
25.
Tew WP, Gordon M, Murren J, et al.
Phase 1 study of aflibercept administered
subcutaneously to patients with advanced
solid tumors. Clin Cancer Res
2010;16:358-66
26.
Gillespie J, Mathews R, McDermott MF.
Rilonacept in the management of
cryopyrin-associated periodic syndromes
(CAPS). J Inflamm Res 2010;2010:1-8
27.
Litzinger MT, Fernando R, Curiel TJ,
et al. IL-2 immunotoxin denileukin
diftitox reduces regulatory T cells and
enhances vaccine-mediated T-cell
immunity. Blood 2007;110:3192-201
Hassan R, Bullock S, Premkumar A,
et al. Phase I study of SS1P, a
recombinant anti-mesothelin
immunotoxin given as a bolus I.V.
infusion to patients with
mesothelin-expressing mesothelioma,
ovarian, and pancreatic cancers.
Clin Cancer Res 2007;13:5144-9
Onda M, Beers R, Xiang L, et al. An
immunotoxin with greatly reduced
immunogenicity by identification and
removal of B cell epitopes. Proc Nat
Acad Sci USA 2008;105:11311-16
34.
Kaminski MS, Zelenetz AD,
Press OW, et al. Pivotal study of
iodine I 131 tositumomab for
chemotherapy-refractory low-grade
or transformed low-grade B-cell
non-Hodgkin’s lymphomas.
J Clin Oncol 2001;19:3918-28
35.
Witzig TE, Gordon LI, Cabanillas F,
et al. Randomized controlled trial of
yttrium-90-labeled ibritumomab tiuxetan
radioimmunotherapy versus rituximab
immunotherapy for patients with
relapsed or refractory low-grade,
follicular, or transformed B-cell
non-Hodgkin’s lymphoma. J Clin Oncol
2002;20:2453-63
36.
37.
38.
39.
HER2+ metastatic breast cancer (BC).
J Clin Oncol 2007;25:1042
40.
31.
Genovese MC, Becker JC, Schiff M,
et al. Abatacept for rheumatoid
arthritis refractory to tumor necrosis
factor alpha inhibition. N Engl J Med
2005;353:1114-23
29.
Matsushita S, Koito A, Maeda Y, et al.
Selective killing of HIV-infected cells by
anti-gp120 immunotoxins. AIDS Res
Hum Retroviruses 1990;6:193-203
Schriebl K, Trummer E, Lattenmayer C,
et al. Biochemical characterization of
rhEpo-Fc fusion protein expressed in
CHO cells. Prot Exp Purification
2006;49:265-75
23.
28.
30.
Lowenberg B, Beck J, Graux C,
et al. Gemtuzumab ozogamicin as
postremission treatment in AML at
60 years of age or more: results of a
multicenter phase III study. Blood
2010;115:2586-91
Beeram M, Krop I, Modi S, et al.
A phase I study of
trastuzumab-MCC-DM1 (T-DM1),
a first-in-class HER2 antibody-drug
conjugate (ADC), in patients (pts) with
Expert Opin. Drug Discov. (2010) 5(11)
1137
Advances in targeted therapeutic agents
51.
52.
Expert Opin. Drug Discov. Downloaded from informahealthcare.com by Eisai Inc on 02/18/11
For personal use only.
53.
54.
55.
56.
57.
Kesavan K, Ratliff J, Johnson EW, et al.
Annexin A2 Is a molecular target for
TM601, a peptide with tumor-targeting
and anti-angiogenic effects. J Biol Chem
2010;285:4366-74
Akella NS, Nabors LB, Rosenfeld SS,
et al. A phase I evaluation of intravenous
TM601 in recurrent glioblastoma: use of
perfusion MRI to monitor antiangiogenic
effects. J Clin Oncol 2009;27:2041
Phase 2 Clinical Study Substantiates
Peptide’s Ability to Deliver Cytotoxic
Payloads to Refractory Tumors.
Transmolecular press release;
23 October 2009. Available from:
www.transmolecular.com
Gupta VR, Wilson BA, Blanke SR.
Sphingomyelin is important for the
cellular entry and intracellular
localization of Helicobacter pylori.
Cell Microbiol; In press
66.
74.
Chui Yl, Rana TM. siRNA function in
RNAi: a chemical modification analysis.
RNA 2003;9:1034-8
Matsumura H, Ito A, Saitoh H, et al.
SuperSAGE. Cell Microbiol
2005;7:11-18
75.
Sioud M. Induction of inflammatory
cytokines and interferon responses by
double-stranded and single-stranded
siRNAs is sequence-dependent and
requires endosomal localization.
J Mol Biol 2005;348:1079-90
Bae CD, Juhnn YS, Park JB.
Post-transcriptional control of c-erb
B-2 overexpression in stomach cancer
cells. Exp Mol Med 2001;33:15-19
76.
Jackson AL, Burchard J, Leake D, et al.
Position-specific chemical modification
of siRNAs reduces “off-target” transcript
silencing. RNA 2006;12:1197-1205
Hood BL, Conrads TP, Veenstra TD.
Mass spectrometric analysis of
formalin-fixed paraffin-embedded
tissue: unlocking the proteome within.
Proteomics 2006;6:4106-14
77.
Lu KP. Pinning down cell signaling,
cancer and Alzheimer’s disease.
Trends Biochem Sci 2004;29:200-9
78.
Evans MJ, von Hahn T, Tscherne DM,
et al. Claudin-1 is a hepatitis C virus
co-receptor required for a late step in
entry. Nature 2007;446:801-5
Li J, Sai T, Berger R, et al. Human
antibodies for immunotherapy
development generated via a human
B-cell hybridoma technology. Proc Natl
Acad Sci USA 2006;103:3557-62
68.
79.
Nascimento FD, Hayashi MAF,
Kerkis A, et al. Crotamine mediates
gene delivery into cells through the
binding to heparan sulfate proteoglycans.
J Biol Chem 2007;282:21349-60
Citro G, Perrotti D, Cucco C, et al.
Inhibition of leukemia cell proliferation
by receptor-mediated uptake of c-myb
antisense oligodeoxynucleotides.
Proc Natl Acad Sci USA 1992;89:7031-5
69.
Sun L, Fuselier JA, Murphy WA,
Coy DH. Antisense peptide nucleic acids
conjugated to somatostatin analogs and
targeted at the n-myc oncogene
display enhanced cytotoxity to human
neuroblastoma IMR32 cells expressing
somatostatin receptors. Peptides
2002;23:1557-65
Garin-Chesa P, Campbell I, Saigo PE,
et al. Trophoblast and ovarian cancer
antigen LK26. Sensitivity and specificity
in immunopathology and molecular
identification as a folate- binding protein.
Am J Pathol 1993;142:557-67
80.
Sahin U, Tureci O, Pfreundschuh M.
Serological identification of human
tumor antigens. Curr Opin Immunol
1997;9:709-16
81.
Katano M, Irie RF. Human monoclonal
antibody to tumor-associated ganglioside
GD2: suppressed growth of human
melanoma in nude mice. Immunol Lett
1984;8:169-74
82.
Ollert MW, David K, Schmit C, et al.
Normal human serum contains a natural
IgM antibody cytotoxic for human
neuroblastoma cells. Proc Natl Acad
Sci USA 1996;93:4498-503
83.
Rommens JM, Iannuzzi MC, Kerem B,
et al. Identification of the cystic fibrosis
gene: chromosome walking and jumping.
Science 1989;245:1059-65
84.
Baker SJ, Fearon ER, Nigro JM, et al.
Chromosome 17 deletions and p53 gene
mutations in colorectal carcinomas.
Science 1989;244:217-21
85.
Liaw D, Marsh DJ, Li J, et al. Germline
mutations of the PTEN gene in Cowden
disease, an inherited breast and thyroid
cancer syndrome. Nat Genet
1997;16:64-7
Szczylik C, Skorski T, Nicolaides NC,
et al. Selective inhibition of leukemia cell
proliferation by BCR-ABL antisense
oligodeoxynucleotides. Science
1991;253:562-5
59.
Kurrek J. Antisense technologies.
Improvement through novel chemical
modifications. Eur J Biochem
2003;270:1628-44
60.
de Smet MD, Meenken CJ,
van den Horn GJ. Fomivirsen -- a
phosphorothioate oligonucleotide for
the treatment of CMV retinitis.
Ocul Immunol Inflamm 1999;7:189-98
1138
65.
epitope of the epithelial mucin (MUC1).
Glycobiology 2004;14:681-92
Hasegawa T, Fujisawa T, Haraguchi S,
et al. Schizophyllan--folate conjugate as
a new non-cytotoxic and cancer-targeted
antisense carrier. Bioorg Med Chem Lett
2005;15:327-30
Crooke ST. Antisense drug technology.
CRC Press; 2008
62.
64.
Crooke ST. Advances in understanding
the pharmacological properties of
antisense oligonucleotides.
Adv Pharmacol 1997;40:1-49
67.
58.
61.
63.
Raal FJ, Santos RD, Blom DJ, et al.
Mipomersen, an apolipoprotein B
synthesis inhibitor, for lowering of LDL
cholesterol concentrations in patients
with homozygous familial
hypercholesterolaemia: a randomised,
double-blind, placebo-controlled trial.
Lancet 2010;375:998-1006
Dickman S. Clouds over the
VC sky. Available from:
www.bostonbiotechwatch.com 2009
70.
71.
72.
73.
Zhang Y, Lee HJ, Boado RJ,
Pardridge WM. Receptor-mediated
delivery of an antisense gene to human
brain cancer cells. J Gene Medicine
2002;4:183-94
Islam A, Handley SL, Thompson KSJ,
Akhtar S. Studies on uptake, sub-cellular
trafficking and efflux of antisense
oligodeoxynucleotides in glioma cells
using self-assembling cationic lipoplexes
as delivery systems. J Drug Targeting
1999;7:373-82
Mae M, Andaloussi SE, Lehto T,
Langel U. Chemically modified
cell-penetrating peptides for the delivery
of nucleic acids. Expert Opin Drug Deliv
2009;6:1195-205
Karsten U, Serttas N, Paulsen H,
et al. Binding patterns of
DTR-specific antibodies reveal a
glycosylation-conditioned tumor-specific
Expert Opin. Drug Discov. (2010) 5(11)
Nicolaides, Sass & Grasso
86.
87.
Expert Opin. Drug Discov. Downloaded from informahealthcare.com by Eisai Inc on 02/18/11
For personal use only.
88.
99.
Shore EM, Xu M, Feldman GJ.
A recurrent mutation in the BMP type I
receptor ACVR1 causes inherited and
sporadic fibrodysplasia ossificans
progressive. Nat Genet 2006;38:525-7
Adams TE, Koziolek EJ, Hoyne PH,
et al. A truncated soluble epidermal
growth factor receptor-Fc fusion ligand
trap displays anti-tumour activity in vivo.
Growth Factors 2009;27:141-54
100.
Diaz-Ricart M, Bozzo J. rPSGL-Ig.
Drugs Fut 2002;27:346-9
101.
Tsimberidou AM, Giles FJ,
Kantarjian HM, et al. Anti-B4
blocked ricin post chemotherapy in
patients with chronic lymphocytic
leukemia -- long-term follow-up of a
monoclonal antibody-based approach
to residual disease. Leuk Lymphoma
2003;44:1719-25
Wolff AC, Hammond EH, Schwartz JN,
et al. American Society of Clinical
Oncology/College of American
Pathologists guideline recommendations
for human epidermal growth factor
receptor 2 testing in breast cancer.
J Clin Oncol 2007;25:118-45
89.
Adams J. Pharmacogenomics and
personalized medicine. Nat Educat
2008;1:1-2
90.
Han J. Monoclonal antibodies as cancer
therapeutics. NAMJS 2010;3:1-6
91.
Ruckle J, Jacobs M, Kramer W, et al.
Single-dose, randomized, double-blind,
placebo-controlled study of ACE-011
(ActRIIA-IgG1) in postmenopausal
women. J Bone Miner Res
2009;24:744-52
92.
Lee SJ, McPherron AC. Regulation
of myostatin activity and muscle
growth. Proc Nat Acad Sci USA
2001;98:9306-11
93.
102.
Fujisawa T, Nakashima H, Nakajima A,
et al. Targeting IL-13Ralpha2 in human
pancreatic ductal adenocarcinoma with
combination therapy of IL-13-PE and
gemcitabine. Int J Cancer; In press
103.
Ribbert T, Thepen T, Tur MK,
et al. Recombinant, ETA’-based
CD64 immunotoxins: improved
efficacy by increased valency, both
in vitro and in vivo in a chronic
cutaneous inflammation model in human
CD64 transgenic mice. Br J Dermatol
2010;163:279-86
104.
Mitchell D, Pobre EG, Mulivor AW,
et al. ALK1-Fc inhibits multiple
mediators of angiogenesis and suppresses
tumor growth. Mol Cancer Ther
2010;9:379-88
94.
Available from: www.apogenix.com
95.
Ansell SM, Witzig TE, Inwards DJ,
et al. Phase I clinical study of atacicept
in patients with relapsed and refractory
B-cell non-Hodgkin’s lymphoma.
Clin Cancer Res 2008;14:1105-10
96.
Vincenti F, Larson C, Durrbach A, et al.
Costimulation blockade with belatacept
in renal transplantation. N Engl J Med
2005;353:770-81
97.
Hughes LB, Danila MI, Bridges SL.
Recent advances in personalizing
rheumatoid arthritis therapy and
management. Personalized Med
2009;6:159-70
98.
with advanced malignancies.
Mol Cancer Ther 2009;8:A103
Isozaki K, Terris B, Belghiti J, et al.
Germline-activating mutation in the
kinase domain of KIT gene in familial
gastrointestinal stromal tumors.
Am J Pathol 2000;157:1091-5
Tolcher A, Papadopoulos K, Agnew J,
et al. Preliminary results of a
phase 1 study of FP-1039 (FGFR1:Fc),
a novel antagonist of multiple fibroblast
growth factor (FGF) ligands, in patients
Gattenlohner S, Jorissen H, Huhn M,
et al. A human recombinant
autoantibody-based immunotoxin
specific for the fetal acetylcholine
receptor inhibits rhabdomyosarcoma
growth in vitro and in a murine
transplantation model.
J Biomed Biotechnol 2010;1:1-11
108. Nagai T, Tanaka M, Tsuneyoshi Y,
et al. In vitro and in vivo efficacy of a
recombinant immunotoxin against folate
receptor beta on the activation and
proliferation of rheumatoid arthritis
synovial cells. Arthritis Rheum
2006;54:3126-34
109. Du X, Ho M, Pastan I. New
immunotoxins targeting CD123, a stem
cell antigen on acute myeloid leukemia
cells. J Immunother 2007;30:607-13
110. Schwemmlein M, Stieglmaier J,
Kellner C, et al. A CD19-specific
single-chain immunotoxin mediates
potent apoptosis of B-lineage leukemic
cells. Leukemia 2007;21:1405-12
111. Singh R, Samant U, Hyland S, et al.
Target-specific cytotoxic activity of
recombinant immunotoxin
scFv(MUC1)-ETA on breast carcinoma
cells and primary breast tumors.
Mol Cancer Ther 2007;6:562-9
112. Whiteman K, Ab O, Bartle L, et al.
Efficacy of IMGN901 (huN901-DM1)
in combination with bortezomib and
lenalidomide against multiple myeloma
cells in preclinical studies.
AACR Meeting Abstracts
2008;2008:2146
113. Quiles S, Raisch KP, Sanford LL, et al.
Synthesis and preliminary biological
evaluation of high-drug-load
paclitaxel-antibody conjugates for
tumor-targeted chemotherapy.
J Med Chem 2010;53:586-94
105.
Zielinski R, Lyakhov I, Jacobs A, et al.
Affitoxin -- a novel recombinant,
HER2-specific, anticancer agent for
targeted therapy of HER2-positive
tumors. J Immunother 2009;32:817-25
114. Ikeda H, Hideshima T, Fulciniti M,
et al. The monoclonal antibody
BT062 conjugated to cytotoxic
maytansinoids has potent and selective
cytotoxicity against CD138 positive
multiple myeloma cells in vitro and
in vivo. Dana Farber Cancer Care
Conference; 2009
106.
Cizeau J, Grenkow DM, Brown JG,
et al. Engineering and biological
characterization of VB6-845, an
anti-EpCAM immunotoxin containing
a T-cell epitope-depleted variant of the
plant toxin bouganin. J Immunother
2009;32:574-84
115. Bander NH, Milowsky MI,
Nanus DM, et al. Phase I trial
of 177Lutetium-labeled J591, a
monoclonal antibody to prostate-specific
membrane antigen, in patients with
androgen-independent prostate cancer.
J Clin Oncol 2005;23:4591-601
107.
Nagai T, Tanaka M, Tsuneyoshi Y,
et al. Targeting tumor-associated
macrophages in an experimental
glioma model with a recombinant
immunotoxin to folate receptor beta.
Cancer Immunol Immunother
2009;58:1577-86
116. Bigner DD, Brown M, Coleman RE,
et al. Phase I studies of treatment
of malignant gliomas and neoplastic
meningitis with131I-radiolabeled
monoclonal antibodies anti-tenascin
81C6 and anti-chondroitin proteoglycan
sulfate Me1-14 F (ab¢)2. J Neurooncol
1995;24:109-25
Expert Opin. Drug Discov. (2010) 5(11)
1139
Advances in targeted therapeutic agents
117. Available from: www.seagen.com
118. Rondinone CM, Trevillyan JM,
Clampit J, et al. Protein tyrosine
phosphatase 1B reduction regulates
adiposity and expression of genes
involved in lipogenesis. Diabetes
2002;51:2405-11
119. Chi KN, Zoubeidi A, Gleave ME.
Custirsen (OGX-011):
a second-generation antisense inhibitor
of clusterin for the treatment of cancer.
Expert Opin Investig Drugs
2008;17:1955-62
Expert Opin. Drug Discov. Downloaded from informahealthcare.com by Eisai Inc on 02/18/11
For personal use only.
120. Available from: www.altairtherapeutics.
com
121. DeVincenzo J, Lambkin-Williams R,
Wilkinson T, et al. A randomized,
double-blind, placebo-controlled study of
an RNAi-based therapy directed against
respiratory syncytial virus. Proc Natl
Acad Sci USA 2010;107:8800-5
122. Molitoris BA, Dagher PC, Sandoval RM,
et al. A chemical inhibitor of p53 that
protects mice from the side effects of
cancer therapy. Science 1999;285:1733-7
Affiliation
Nicholas C Nicolaides†, Philip M Sass &
Luigi Grasso
†
Author for correspondence
Morphotek, Inc.,
210 Welsh Pool Road,
Exton, PA 19341, USA
Tel: +1 610 423 6100;
E-mail: [email protected]
1140
Expert Opin. Drug Discov. (2010) 5(11)























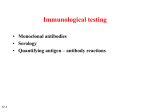

![Anti-PCB antibody [3H2AD9] ab110314 Product datasheet 3 Images Overview](http://s1.studyres.com/store/data/000076345_1-acbfa58e194757c519d151062b812354-150x150.png)

