Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Remote ischemic conditioning wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Rheumatic fever wikipedia , lookup
Electrocardiography wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Coronary artery disease wikipedia , lookup
Jatene procedure wikipedia , lookup
Heart failure wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Heart arrhythmia wikipedia , lookup
Atrial septal defect wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
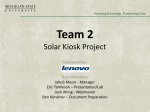
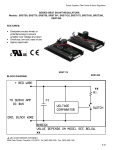
Acute and Chronic Heart Dilation Model-Induced in Goats by Carotid Jugular A-V Shunt Gil Bolotin, Roberto Lorusso, Hans Kaulbach, Jan Schreuder, Gideon Uretzky and Frederik H. Van Der Veen Cardiovascular Research Institute, Maastricht, The Netherlands Abstract Congestive heart failure is characterized by impaired quality of life and markedly shortened life expectancy. There are currently many medical and surgical modalities that aim to treat patients with heart failure, which implies the need for an animal heart failure model for the development and testing of these therapeutic modalities. A variety of animal heart failure models have been developed, including those in which heart failure is induced via drugs, rapid ventricular pacing, genetic alteration, viral sources, idiopathic dilated cardiomyopathy, coronary arteries’ embolization, pressure overload, and volume overload by arteriovenous (A-V) shunt. The purpose of this study was to evaluate the acute and chronic effect of carotid-jugular A-V shunt in goat model of heart dilation. After cross clamping of the left carotid artery, an end-to-side anastomosis of 10 mm in diameter was performed between the free end of the vein and the side of the artery. A dual-micromanometer transducer conductance catheter was used to determine the volume of the ventricle on-line, by measuring the time-varying electrical conductance of the segments of intraventricular blood. During and at the end of the eight weeks none of the animals showed signs of heart failure or distress. The acute and chronic hemodynamic changes were demonstrated by pressure-volume loops at baseline, immediately after the shunt, and after 8 weeks. There was an immediate rise in the LVEDV (104±27 ml) compared to the baseline volume (75±26 ml), and eight weeks later the LVEDV reached 111±22 ml. None of the eight goats demonstrated clinical signs of pulmonary congestion. The Swan-Ganz and the conductance catheters that were used to monitor the heart hemodynamic changes immediately after the creation of the A-V shunt revealed interesting results. Another advantage of the shunt model is that it is possible to evaluate the patency of the shunt by palpating blood thrill in the neck. The carotid jugular A-V shunt in goats causes significant left heart dilation without signs of heart failure, and is reproducible with low animal mortality. The study ended 8 weeks after the creation of the A-V shunt, leaving unanswered the question of possible heart failure development in this model after a longer follow up period. Key words: animal heart failure model, arterio-venous (A-V) shunt, congestive heart failure, hemodynamic changes carotid-jugular A-V shunt. Basic Appl. Myol. 9 (5): 219-222, 1999 Congestive heart failure is characterized by impaired quality of life and markedly shortened life expectancy [1]. Optimal medical treatment of patients with congestive heart failure improves the quality of life and survival rates, but mortality is still unacceptably high [9]. There are currently many medical and surgical modalities that aim to treat patients with heart failure, which implies the need for an animal heart failure model for the development and testing of these therapeutic modalities. A variety of animal heart failure models have been developed, including those in which heart failure is induced via drugs [5], rapid ventricular pacing [13], genetic alteration [10], viral sources [6], idiopathic dilated cardiomyopathy [4], coronary arteries’ embolization [8], pressure overload [2], and volume overload by arteriovenous (A-V) shunt [3]. The A-V shunt model induces left heart dilation that mimics the clinical situation in patients with dilated cardiomyopathy [11]. - 219 - Acute and chronic heart dilation model-induced in goats by carotid jugular A-V shunt played a typical phasic LV volume tracing. A Leycom Sigma-5DF signal conditioner-processor (CardioDynamics, Zoetermeer, The Netherlands) provided the current source and processed the segmental conductance, producing an on-line display of the LV contours, as well as continuous and instantaneous volume signals. The volume signals were combined with the pressure signals on an X-Y oscilloscope to provide an instantaneous and uninterrupted display of pressure-volume loops. Readings of the volume signal were corrected to account for the parallel conductance caused by tissues surrounding the ventricular cavities. A bolus of 7.5 ml of hypertonic NaCl (9%) was injected into the central venous compartment via the Swan-Ganz catheter. As the bolus mixed with the fluid in the ventricular cavity, its conductivity increased, causing the overall conductance signal to increase while the parallel component remained constant. End-systolic overall conductance was then plotted as a function of end-diastolic overall conductance during the mixing of the bolus; the conductance was equal to the intersection point between the regression line of these values and the line of identity. The purpose of this study was to evaluate the acute and chronic effect of carotid-jugular A-V shunt in goat model of heart dilation. Methods Experiments were performed in eight female goats, weighing 51 to 80 kg, in accordance with the Guide for the Care and Use of Laboratory Animals published by the National Institutes of Health (NIH publication 8623, revised 1985). Dilated cardiomyopathy was induced by a left carotid jugular A-V shunt. The acute and chronic hemodynamic changes were followed for 8 to l0 weeks by three different monitoring modalities: Swan-Ganz catheters measured cardiac output before, immediately after the creation of the A-V shunt, and 8 weeks later; conductance catheters measured left ventricle dimensions and performance before, immediately after the creation of the A-V shunt, and 8 weeks later; and echocardiography was performed before and every two weeks after the AV shunt operation. A-V shunt procedure General anesthesia was induced by thiopental sodium (Pentothal, Abbott S.P.A., Italy), administered intravenously at 15 mg per kg body weight, and maintained after endotracheal intubation with oxygen/nitrous oxide (1:2) and 1.5% Fluothane (Halothane, Zeneca Ltd., Macclesfield, Cheshire, UK). During the experiments, the lungs were ventilated with a positive pressure respirator (Harvard, Apparatus Inc., South Natick, Massachusetts) and body temperature was kept constant with a heating mattress. A single dose of 10.000 IU heparin i.v. was administered. Through a cervical incision, the left jugular vein and the left carotid artery were mobilized over a length of approximately 5 cm and ligated distally. After crossclamping of the left carotid artery, an end-to-side anastomosis of 10 mm in diameter was performed between the free end of the vein and the side of the artery, using 6-0 polypropylene non-absorbable running sutures (Ethicon, Edinburgh, Scotland). Clamps were removed and the patency of the fistula was visually confirmed by the pulsatile filling of the jugular vein. Results During and at the end of the eight weeks none of the animals showed signs of heart failure or distress. One animal died three weeks after the A-V shunt operation most probably due to lung infection. The carotid-jugular A-V-shunt induced both immediate and long-term hemodynamic changes. The immediate effect of the shunt, an abrupt rise in cardiac output, was observed within 30 minutes after opening of the shunt and measured by Swan-Ganz thermodilution technique: 7.9±1.9 l/min compared to the baseline cardiac output of 4.9±1.3 l/min. Eight weeks after the shunt procedure, an increase in cardiac output was observed in comparison not only to the baseline value but also to the measurements obtained immediately after opening of the shunt, measuring 9.9±2.7 l/min. Echocardiography tests revealed a gradual increase in left ventricular end-diastolic diameter, reaching the maximal left ventricle dilation at 8 weeks (Fig. 1). The acute and chronic hemodynamic changes were demonstrated by pressure-volume loops at baseline, immediately after the shunt, and after 8 weeks (Fig. 2). There was an immediate rise in the LVEDV (104±27 ml) compared to the baseline volume (75±26 ml), and eight weeks later the LVEDV reached 111±22 ml. Heart catheterization A dual-micromanometer transducer conductance catheter (7F, Sentron, The Netherlands) was used to determine the volume of the ventricle on-line, by measuring the time-varying electrical conductance of the segments of intraventricular blood [8]. The catheter’s position along the long axis of the left ventricular cavity via the left femoral artery was set under fluoroscopic guidance and verified by inspection of the segmental conductance signals: a correct position was assumed if the signals of at least the four most distal segments dis- Discussion This study demonstrates that the A-V shunt heart failure model is capable of producing stable, immediate and long-term high cardiac output (overload) dilation. None of the eight goats demonstrated clinical signs of pulmonary congestion. Fortunately, these results are in contrast with the high mortality rates (77%) and signs of - 220 - Acute and chronic heart dilation model-induced in goats by carotid jugular A-V shunt The Swan-Ganz and the conductance catheters that were used to monitor the heart hemodynamic changes immediately after the creation of the A-V shunt revealed interesting results. The abrupt rise in cardiac output generated huge hemodynamic changes. The LVEDV increased from 75 ml to 104 ml, while the LVESV reduced from 27 ml to 20 ml, together resulting in an abrupt rise in left ventricle ejection fraction (from 57% to 79%) and stroke volume (from 37 ml to 72 ml). Strangely, no changes in heart rate were observed. We observed a moderate rise in the dPdt max (from 1361 mmHg/s to 1423 mmHg/s), as well as a significant rise in peak ejection rate (PER) from 280 (ml/s) before the shunt to 446 (ml/s) immediately afterward. All these dramatic changes were reversible at this point in time, by closure of the shunt. These results suggest that the wide changes in left ventricle model are within the efficient part on Starling’s curve. Another advantage of the shunt model is that it is possible to evaluate the patency of the shunt by palpating the blood thrill in the neck. The shunt’s location facilitates access to ultrasonic measures for a more precise evaluation, as well as temporary closure, obtained by applying manual pressure at the animal’s neck. Our study ended 8 weeks after the creation of the A-V shunt, leaving unanswered the question of possible heart failure development in this model after a longer follow up period. In conclusion, the carotid jugular A-V shunt in goats causes significant left heart dilation without signs of heart failure, and is reproducible with low animal mortality. Figure 1. Left ventricular end-diastolic volume assessed by echo cardiography at 2-4 weeks intervals. Address correspondence to: Dr Ir FH van der Veen, Cardiothoracic Surgery, PO Box 5800, 6202 AZ, Academic Hospital, Maastricht, Netherlands, Email [email protected]. Figure 2. Pressure volume loops before I, 45 minutes after II, and 8 weeks after the creation of the shunt. References pulmonary congestion that commonly occur within 24 hours of performing the A-V shunt in small animals, as reported by Flaim and coworkers [10]. This discrepancy is probably due to the relatively small A-V shunt of approximately 10mm, used in our study (in goats weighing 51 to 80 kg). Moreover, in the present study the animals presented neither clinical nor hemodynamic signs of heart failure, such as tachycardia or an increase in LVEDP, as was observed with inferior vena cava aortic A-V shunt applied in mongrel dogs [7]. The successful compensatory mechanism in the goat carotid jugular A-V shunt is the reason for the lack of signs of renal failure such as were demonstrated in a rat aortovenocaval fistula by Wegner and coworkers [12]. Therefore, the described model should be considered a compensatory overload dilation model rather than a heart failure model. [1] Cohn JN: Current therapy of failing heart. Circulation 1988; 78: 1099-1107. [2] Desjardins S, Mueller RW, Cauchy MJ: A pressure overload model of congestive heart failure in rats. Cardiovasc Res 1988; 22 (10): 696-702. [3] Flaim SF, Minteer WJ, Nellis SH, Clark DP: Chronic arteriovenous shunt: evaluation of a model for heart failure in rat. Am J Physiol 1979; 236 (5): H698-704. [4] Genao A, Seth K, Schmidt U, Carles M, Gwathmey JK: Dilated cardiomyopathy in turkeys: an animal model for the study of human heart failure. Lab Anim Sci 1996; 46 (4): 399-404. [5] Muders F, Friedrich E, Luchner A, Pfeifer M, Ickenstein G: Hemodynamic changes and neurohemoral regulation during development of congestive - 221 - Acute and chronic heart dilation model-induced in goats by carotid jugular A-V shunt [9] Swedberg K: Reduction in mortality by pharmacological therapy in congestive heart failure. Circulation 1993; 87 (suppl. IV): IV-126-IV-129. [10] Tofovic SP, Kusake H, Rominski B, Jackson EK: Caffeine increases renal renin secretion in a rat model of genetic heart failure. J Cardiovasc Pharmacol 1999; 33 (3): 440-450. [11] Vasan RS, Larson MG, Benjamin EJ, Evans JC, Levy D: Left ventricular dilatation and the risk of congestive heart failure in people without myocardial infarction. Engl J Med 1997; 336 (19): 13501355. [12] Wegner M, Hirth-Dietrich C, Stasch JP: Role of neutral endopeptidase 24.11 in AV fistular rat model of heart failure. Cardiovasc Res 1996; 31 (6): 891-898. [13] Winslow RL, Rice J, Jafri S, Marban E, O’Rourke B: Mechanisms of altered excitation-contraction coupling in canine tachycardia-induced heart failure, II: model studies. Circ Res 1999; 19; 84 (5): 571-586. heart failure in a model of epinephrin-induced cardiomyopathy in conscious rabbits. J Card Fail 1999; 5 (2): 109-116. [6] Nishio R, Matsumori A, Shioi T, Wang W, Yamada T, Ono K, Sasayama S: Denopamine, a b 1 – adrenergic agonist, prolongs survival in a murine model of congestive heart failure induced by viral myocarditis: suppression of tumor necrosis factor-alpha production in the heart. J Am Coll Cardiol 1998; 32 (3): 808-815. [7] Porter CB, Walsh RA, Badke FR, O’Rourke RA: Differential effects of diltiazem and nitroprusside on left ventricular function in experimental chronic volume overload. Circulation 1983; 68: 685-692. [8] Sabbah HN, Stein PD, Kono T, Gheorghiade M, Levine TB, Jafri S, Hawkins ET, Goldstein S: A canine model of chronic heart failure produced by multiple sequential coronary microembolizations. Am J Physiol 1991; 260 (4 Pt 2): H1379-1384. - 222 -