Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Clostridium difficile infection wikipedia , lookup
West Nile fever wikipedia , lookup
Sarcocystis wikipedia , lookup
Neglected tropical diseases wikipedia , lookup
Meningococcal disease wikipedia , lookup
Trichinosis wikipedia , lookup
Neonatal infection wikipedia , lookup
Marburg virus disease wikipedia , lookup
Eradication of infectious diseases wikipedia , lookup
Diagnosis of HIV/AIDS wikipedia , lookup
Brucellosis wikipedia , lookup
Middle East respiratory syndrome wikipedia , lookup
Chagas disease wikipedia , lookup
Sexually transmitted infection wikipedia , lookup
Human cytomegalovirus wikipedia , lookup
Dirofilaria immitis wikipedia , lookup
Hepatitis C wikipedia , lookup
Hepatitis B wikipedia , lookup
Leishmaniasis wikipedia , lookup
Hospital-acquired infection wikipedia , lookup
Leptospirosis wikipedia , lookup
Oesophagostomum wikipedia , lookup
Onchocerciasis wikipedia , lookup
Schistosomiasis wikipedia , lookup
Multiple sclerosis wikipedia , lookup
Tuberculosis wikipedia , lookup
African trypanosomiasis wikipedia , lookup
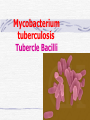
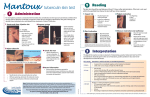
Chapter 13 Respiratory Bacilli •M. tuberculosis (结核分枝杆菌) •C. diphtheria (白喉棒状杆菌) •L. pneumophila(嗜肺军团菌) •B .pretussis (百日咳鲍特菌) •H. influenzae(流感嗜血杆菌) •K. pneumoniae(肺炎克雷伯菌) Section 1 M. tuberculosis 结核分支杆菌 Ziehl-Neelsen stain pink in a contrasting background Mycobacterium (fungus-bacterium) : form mould-like pellicles when grow in the liquid media acid-fastness : impermeability by certain dyes and stains once stained, acid-fast bacteria will retain dyes when heated and treated with acidified organic compounds. ??? thick, complex, lipid-rich, waxy cell walls ! Mycobacterium tuberculosis Tubercle Bacilli Characteristics large nonmotile rod-shaped bacterium facultative intracellular parasite obligate aerobe slow generation time, 15-20 hours Chains of cells in smears made from in vitrogrown colonies often form distinctive serpentine cords. (cord factor) Characteristics Middlebrook's medium Lowenstein-Jensen medium •small and buff colored colonies •4-6 weeks inhibitors to keep contaminants from out-growing M.TB. Characteristics M.TB acid-fast bacteria(AFB) Ziehl-Neelsen stain the M.TB. smear is fixed, stained with carbolfuchsin (a pink dye) decolorized with acid-alcohol. The smear is counterstained with methylene-blue or certain other dyes. Characteristics very sensitive to ultraviolet light heat-sensitive destroyed in the process of pasteurization susceptible to alcohol, formaldehyde and glutaralddehyde resistant acid, alkalis and quaternary ammonium compounds. Constituents A. Cell Wall Structure peptidoglycan Lipid: Mycolic acids unique alpha-branched lipids , strong hydrophobic molecules Cord Factor Wax-D : Freund's complete adjuvant (CFA) Constituents properties of lipids Impermeability to stains and dyes Resistance to many antibiotics Resistance to killing by acidic and alkaline compounds Resistance to osmotic lysis via complement deposition Resistance to lethal oxidations and survival inside of macrophages Constituents B. Proteins: elicit the tuberculin reaction C. Polysaccharides: uncertain D. capsule Virulence Factors M.TB. has special mechanisms for cell entry M.TB. can grow intracellularly. M.TB. interferes with the toxic effects of reactive oxygen intermediates produced in the process of phagocytosis Slow generation time. High lipid concentration in cell wall, Cord factor. Tuberculosis TB infection TB infection means that M.TB. is in the body but the immune system is keeping the bacteria under control. Macrophages surround the tubercle bacilli dfas form a hard shell. ( infiltration of macrophages and lymphocytes with development of granulomas) TB infection: not TB disease, NOT infectious a positive reaction to the tuberculin skin test normal chest x-ray. Tuberculosis: Infection vs Disease TB Infection TB disease in lungs M.TB. present M.TB. present Tuberculin skin test positive Tuberculin skin test positive Chest X-ray normal Chest X-ray usually reveals lesion Sputum smears and cultures negative Sputum smears and cultures positive No symptoms Symptoms such as cough, fever, weight loss Not infectious Often infectious before treatment Not defined as a case of TB Defined as a case of TB Pathogenesis • 10% of infected persons with normal immune systems develop TB at some point in life • HIV strongest risk factor for development of TB if infected - Risk of developing TB disease 7% to 10% each year • Certain medical conditions increase risk that TB infection will progress to TB disease Conditions That Increase the Risk of Progression to TB Disease • HIV infection • Substance abuse • Recent infection • Chest radiograph findings suggestive of previous TB • Diabetes mellitus • Silicosis • Prolonged corticosteriod therapy • Other immunosuppressive therapy Conditions That Increase the Risk of Progression to TB Disease (cont.) • Cancer of the head and neck • Hematologic and reticuloendothelial diseases • End-stage renal disease • Intestinal bypass or gastrectomy • Chronic malabsorption syndromes • Low body weight (10% or more below the ideal) Transmission of M. tuberculosis • Spread by droplet nuclei • Expelled when person with infectious TB coughs, sneezes, speaks, or sings • Close contacts at highest risk of becoming infected • Transmission occurs from person with infectious TB disease (not latent TB infection) Common Sites of TB Disease • Lungs • Pleura • Central nervous system • Lymphatic system • Genitourinary systems • Bones and joints • Disseminated (miliary TB) Stages of the Disease Droplet nuclei are inhaled. Stage 1 Stages of the Disease Stage 2 7-21 days after M.TB. multiplies macrophages are unactivated Stages of the Disease Stage 3 lymphocytes infiltrate: MHC molecules T-cell activation liberate cytokines (IFN) activation of macrophages tuberculin-positive : the result of the host developing a vigorous cell mediated immune (CMI) response Stages of the Disease Stage 3 tubercle formation begins The center of the tubercle is characterized by "caseation necrosis" meaning semisolid or "cheesy" consistency. M.TB. cannot multiply within these tubercles because of the low pH and anoxic environment. M.TB. can persist within these tubercles for extended periods Stages of the Disease Stage 4 M.TB replicate in unactivated macrophages the growing tubercle invade bronchus or blood supply line. hematogenous spread result in extrapulmonary tuberculosis otherwise known as miliary tuberculosis. at almost any anatomical location Stage 4 two types Stages of the Disease 1.Exudative lesions result from the accumulation of PMN's around M.TB. bacteria replicate with virtually no resistance. This situation gives rise to the formation of a "soft tubercle". 2.Productive or granulomatous lesions hypersensitive to tuberculoproteins. This situation gives rise to the formation of a "hard tubercle". Stages of the Disease Stage 5 the caseous centers of the tubercles liquify. M.TB begins to rapidly multiply extracellularly large antigen load causes the walls of nearby bronchi to become necrotic and rupture. cavity formation. M.TB. to spill into other airways and rapidly spread to other parts of the lung. Classification System for TB Description Class Type 0 No TB exposure Not infected No history of exposure Negative reaction to tuberculin skin test 1 TB exposure No evidence of infection TB infection No disease History of exposure Negative reaction to tuberculin skin test 3 TB, clinically active M. tuberculosis cultured (if done) Clinical, bacteriological, or radiographic evidence of current disease 4 TB Not clinically active History of episode(s) of TB or Abnormal but stable radiographic findings Positive reaction to the tuberculin skin test Negative bacteriologic studies (if done) and No clinical or radiographic evidence of current disease 5 TB suspected Diagnosis pending 2 Positive reaction to tuberculin skin test Negative bacteriologic studies (if done) No clinical, bacteriological, or radiographic evidence of active TB Drug-Resistant TB • Drug-resistant TB transmitted same way as drug-susceptible TB • Drug resistance is divided into two types: - Primary resistance develops in persons initially infected with resistant organisms - Secondary resistance (acquired resistance) develops during TB therapy Testing for TB Disease and Infection Purpose of Targeted Testing • Find persons with LTBI who would benefit from treatment • Find persons with TB disease who would benefit from treatment • Groups that are not high risk for TB should not be tested routinely All testing activities should be accompanied by a plan for follow-up care. Administering the Tuberculin Skin Test or Mantoux test • Inject intradermally 0.1 ml of 5TU(0.000lmg) PPD tuberculin • PPD(purified protein derivative) • Produce wheal 6 mm to 10 mm in diameter • Do not recap, bend, or break needles, or remove needles from syringes • Follow universal precautions for infection control Reading the Tuberculin Skin Test • Read reaction 48-72 hours after injection • Measure only induration • Record reaction in millimeters Tuberulin Test positive if the diameter of the resulting lesion is 5 mm or greater. The lesion is characterized by erythema (redness) and swelling and induration (raised and hard). Classifying the Tuberculin Reaction >=5 mm is classified as positive in • HIV-positive persons • Recent contacts of TB case • Persons with fibrotic changes on chest radiograph consistent with old healed TB • Patients with organ transplants and other immunosuppressed patients Classifying the Tuberculin Reaction (cont.) >=10 mm is classified as positive in • Recent arrivals from high-prevalence countries • Injection drug users • Residents and employees of high-risk congregate settings • Mycobacteriology laboratory personnel • Persons with clinical conditions that place them at high risk • Children <4 years of age, or children and adolescents exposed to adults in high-risk categories Classifying the Tuberculin Reaction (cont.) >=15 mm is classified as positive in • Persons with no known risk factors for TB • Targeted skin testing programs should only be conducted among high-risk groups Factors that May Affect the Skin Test Reaction Type of Reaction False-positive False-negative Possible Cause Nontuberculous mycobacteria BCG vaccination Anergy Recent TB infection Very young age (< 6 months) Live-virus vaccination Overwhelming TB disease Anergy • Do not rule out diagnosis based on negative skin test result • Consider anergy in persons with no reaction if - HIV infected - Overwhelming TB disease - Severe or febrile illness - Viral infections - Live-virus vaccinations - Immunosuppressive therapy. • Anergy skin testing no longer routinely recommended Boosting • Some people with LTBI may have negative skin test reaction when tested years after infection • Initial skin test may stimulate (boost) ability to react to tuberculin • Positive reactions to subsequent tests may be misinterpreted as a new infection Two-Step Testing Use two-step testing for initial skin testing of adults who will be retested periodically • If first test positive, consider the person infected • If first test negative, give second test 1-3 weeks later • If second test positive, consider person infected • If second test negative, consider person uninfected Diagnosis of TB Evaluation for TB • Medical history • Physical examination • Mantoux tuberculin skin test • Chest radiograph • Bacteriologic or histologic exam Symptoms of Pulmonary TB • Productive, prolonged cough (duration of >=3 weeks) • Chest pain • Hemoptysis Systemic Symptoms of TB • Fever • Chills • Night sweats • Appetite loss • Weight loss • Easy fatigability Medical History • Symptoms of disease • History of TB exposure, infection, or disease • Past TB treatment • Demographic risk factors for TB • Medical conditions that increase risk for TB disease Mantoux Tuberculin Skin Test • Preferred method of testing for TB infection in adults and children Chest Radiograph • Abnormalities often seen in apical or posterior segments of upper lobe or superior segments of lower lobe • May have unusual appearance in HIV-positive persons Arrow points to cavity in patient's right upper lobe. • Cannot confirm diagnosis of TB Specimen Collection • Obtain 3 sputum specimens for smear examination and culture • Persons unable to cough up sputum, induce sputum, bronchoscopy or gastric aspiration • Follow infection control precautions during specimen collection Smear Examination • Strongly consider TB in patients with smears containing acid-fast bacilli (AFB) • Results should be available within 24 hours of specimen collection • Presumptive diagnosis of TB Smear Examination sputum sample is treated with NaOH to kill other contaminating bacteria detection of acid-fast bacilli in sputum via the Ziehl-Neelsen method culture • Use to confirm diagnosis of TB • Culture all specimens, even if smear negative LowensteinJensen medium 4-6 weeks NEW: BACTEC System 9-16days Drug Susceptibility Testing • Drug susceptibility testing on initial M. tuberculosis isolate • Repeat for patients who - Do not respond to therapy - Have positive cultures despite 2 months of therapy • Promptly forward results to the health department Treatment multiple drugs usually lasts from 6-9 months. rifampin (RIF) isoniazid (INH), pyrazinamide (PZA ) ethambutol (EMB) streptomycin (SM) Basic Principles of Treatment • Provide safest, most effective therapy in shortest time • Multiple drugs to which the organisms are susceptible • Never add single drug to failing regimen • Ensure adherence to therapy Adherence • Nonadherence is a major problem in TB control • Use case management and directly observed therapy (DOT) to ensure patients complete treatment Infection Control in Health Care Settings Infectiousness Patients should be considered infectious if they • Are coughing • Are undergoing cough-inducing or aerosolgenerating procedures, or • Have sputum smears positive for acid-fast bacilli and they • Are not receiving therapy • Have just started therapy, or • Have poor clinical response to therapy Infectiousness (cont.) Patients no longer considered infectious if they meet all of these criteria: • Are on adequate therapy • Have had a significant clinical response to therapy, and • Have had 3 consecutive negative sputum smear results Prevention vaccine against M.TB. : BCG (Bacillus of Calmette and Guerin) BCG consists of a live attenuated strain derived from Mycobacterium bovis. This strain of Mycobacterium has remained avirulent for over 60 years. BCG Vaccination Recommendations for BCG Vaccination • recommended in immunization programs or TB control programs in China BCG Contraindications Contraindicated in persons with impaired immune response from • HIV infection • Congenital immunodeficiency • Leukemia • Lymphoma • Generalized malignancy • Receiving high-dose steroid therapy • Receiving alkylating agents • Receiving antimetabolites • Receiving radiation therapy BCG Vaccination and Tuberculin Skin Testing • Tuberculin skin testing not contraindicated for BCGvaccinated persons • LTBI diagnosis and treatment for LTBI considered for any BCG-vaccinated person whose skin test reaction is >=10 mm, if any of these circumstances are present: - Was contact of another person with infectious TB - Was born or has resided in a high TB prevalence country - Is continually exposed to populations where TB prevalence is high Mycobacterium leprae leprosy (Hansen's Disease) leprosy (Hansen's Disease) • Infect skin, nerves • chronic disease • disfigurement "tuberculoid" leprosy & "lepromatous" leprosy diagnosis The organism does not grow in culture media it grow at low temperature it grows well in the armadillo acid-fast stains of skin biopsies and clinical picture Lepromin is used in skin testing. (but no value for diagnosis) Treatment Treatment with antibiotics (initially dapsone and now multi-drug) is effective and the overall disease incidence worldwide is down. Corynebacteria Gram-positive, aerobic, nonmotile, Rod-shaped "Chinese-letter" arrangement of cells : club-shaped or V-shaped "barred" appearance : polyphosphate inclusions called metachromatic granules(Babes-Ernst bodies ) Corynebacterium Diphtheriae diphtheria a thick gray coating over back of throat. pseudomembrane This coating can eventually expand down through airway and, if not treated, the child could die from suffocation Pathogenicity Invasion Toxigenesis: The diphtheria toxin causes the death eukaryotic cells and tissues by inhibition protein synthesis in the cells Diphtheria Toxin Production Following lysogenic conversion with corynebacteriophage ß, or closely related corynebacteriophages, nontoxigenic strains of C diphtheriae become toxigenic Diagnosis staining for metachromatic bodies : intracellular polyphosphate granules (pink) compared to the rest of the cell (blue) Characteristic black colonies are seen on tellurite agar Production of exotoxin can be determined by in vivo or in vitro tests. Treatment & Prevention toxinneutralizing antibody (antitoxin) antibiotics toxoid a trivalent vaccine containing diphtheria toxoid, pertussis vaccine, and tetanus toxoid (DPT or DTP vaccine).