Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
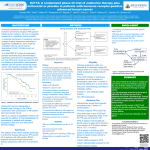
EXEMESTANE VERSUS ANASTROZOLE IN POSTMENOPAUSAL WOMEN WITH EARLY BREAST CANCER A RANDOMIZED CONTROLLED PHASE III TRIAL Paul E. Goss, James N. Ingle, Kathleen I. Pritchard, Matthew J. Ellis, George W. Sledge, G. Thomas Budd, Manuela Rabaglio, Rafat H. Ansari, David B. Johnson, Richard Tozer, David P. D’Souza, Haji Chalchal, Silvana Spadafora, Vered Stearns, Edith A. Perez, Pedro E.R. Liedke, Istvan Lang, Catherine Elliott, Karen A. Gelmon, Judy-Anne W. Chapman, and Lois E. Shepherd JOURNAL OF CLINICAL ONCOLOGY, VOLUME 31 NUMBER 11 APRIL 10 2013 R2 김형오 INTRODUCTION Anastrozole and letrozole Nonsteroidal oral aromatase inhibitors, The most common adjuvant endocrine therapy for hormonedependent early breast cancer in postmenopausal women Superior to tamoxifen, 5 years usage Exemestane Steroidal aromatase inhibitor Superior to 5 years of tamoxifen, when used 2-3 years after 2-3 years of prior tamoxifen INTRODUCTION Adjuvant aromatase inhibitors Accelerated bone resorption from estrogen suppression Exemestane may have less net impact on bone than the nonsteroidals Exemestane v.s. Anastrozole and letrozole Exemestane may suppress estrogen more than anastrozole, and may yield superior efficacy Both are non-cross-resistant Switching one to another may be considered with PD OBJECTIVE MA-27 Exemestane might have advantages over anastrozole for 1st line adjuvant treatment of hormone-dependent early breast cancer in postmenopausal women PATIENTS AND METHODS Study population Histologically confirmed Adequately excised, locally determined, hormone receptor (+) primary invasive cancer Postmenopausal status Age ≥60 years Age 45~59 spontaneous cessation of menses, ≥12 months cessation of menses, ≤12 months, FSH postmenopausal Bilateral oophorectomy PATIENTS AND METHODS Study population 3 wks ≤ completion of CTx ≤ 3 months ECOG 0~2 Min. life expectancy 5 years Exclusion criteria Premenopausal Hormone receptor (-) Contralateral primary breast cancer History of other cancer Except non-melanoma skin cancer or carcinoma in situ of cervix PATIENTS AND METHODS Study end points The primary end point Event free survival Time to loco-regional/distant disease recurrence New primary breast cancer Death from any cause Secondary end points Overall survival Distant disease free survival Incidence of contralateral new primary breast cancer Clinical, laboratory safety RESULTS RESULTS RESULTS • Event frequency – Exemestane vs anastrozole • Distant metastasis – 138 vs 138 • Local in-breast recur – 54 vs 54 • Death – 144 vs 122 • Contralateral breast ca. – 46 vs 33 • Overall survival – Exemestane vs anastrozole 4 year EFS rate 91% on exemestane 91.2% on anastrolzole • Death – 208 vs 204 • Due to breast ca. – 89 vs 98 RESULTS RESULTS DISCUSSION Neither exemestane nor anastrozole was superior in terms of breast cancer outcomes Adverse effects more in Anastrozole Osteoporosis, abnormal lipid levels Exemestane Mild LFT abnormality, atrial fibrillation DISCUSSION Exemestane was not superior to anastrozole Different adverse effect profile Particularly concerning bone health Exemestane should be considered another option to anastrozole or letrozole with hormone receptor positive postmenopausal breast cancer