Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
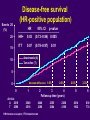
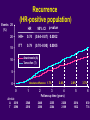
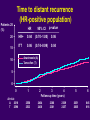
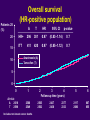
Best first ? The ATAC completed treatment analysis Professor Jack Cuzick Wolfson Institute of Preventive Medicine, London, UK Aims of the ATAC trial Can we improve on tamoxifen as adjuvant therapy for early breast cancer? Can we reduce recurrences, especially in the first few years of treatment? Can we improve the tolerability profile of adjuvant tamoxifen? Is anastrozole superior to tamoxifen in the initial adjuvant setting? ATAC trial design 9366 Postmenopausal women with invasive breast cancer mean age 64 years; 84% hormone receptor positive 61% node negative; 64% with tumour 2 cm in diameter Surgery radiotherapy chemotherapy Randomisation 1:1:1 for 5 years Anastrozole n=3125 Tamoxifen n=3116 Combination arm Combination discontinued following initial n=3125 analysis as no efficacy or tolerability benefit compared with tamoxifen arm Regular follow-up Primary trial endpoints: Disease-free survival Safety / tolerability Secondary trial endpoints: Incidence of contralateral breast cancer Time to distant recurrence Overall survival Time to breast cancer death ATAC completed treatment analysis Follow-up: – data cut-off 31st March 2004 – 68 months’ median follow-up – beyond completion of treatment – only 8% of patients remain on treatment the great majority of these nearing completion Efficacy analysis Disease-free survival (HR-positive population) Events 25 (%) HR 20 15 95% CI p-value HR+ 0.83 (0.73–0.94) 0.005 ITT 0.87 (0.78–0.97) 0.01 Anastrozole (A) 10 Tamoxifen (T) 5 Absolute difference: 1.6% 0 0 At risk: A 2618 T 2598 1 2 2540 2516 2448 2398 HR=hormone receptor; ITT=intent-to-treat 2.6% 3 4 Follow-up time (years) 2355 2304 2268 2189 2.5% 3.3% 5 6 2014 1932 830 774 Recurrence (HR-positive population) Events 25 (%) HR 20 15 95% CI p-value HR+ 0.74 (0.64–0.87) 0.0002 ITT 0.79 (0.70–0.90) 0.0005 Anastrozole (A) 10 Tamoxifen (T) 5 Absolute difference: 1.7% 0 0 At risk: A 2618 T 2598 1 2 2540 2516 2448 2398 2.4% 3 4 Follow-up time (years) 2355 2304 2268 2189 2.8% 3.7% 5 6 2014 1932 830 774 Incidence of contralateral breast cancer (HR-positive population) HR No. of cases 60 95% CI p-value HR+ 0.47 (0.29–0.75) 0.001 ITT 0.58 (0.38–0.88) 0.01 54 6 DCIS 50 40 30 26 20 5 DCIS 21 Invasive* 10 0 Anastrozole (n=2618) *p=0.001 for invasive cancers 48 Invasive* Tamoxifen (n=2598) Time to distant recurrence (HR-positive population) Patients 25 (%) 20 15 HR 95% CI p-value HR+ 0.84 (0.70–1.00) 0.06 ITT 0.86 (0.74–0.99) 0.04 Anastrozole (A) 10 Tamoxifen (T) 5 0 0 At risk: A 2618 T 2598 1 2 3 4 Follow-up time (years) 2550 2533 2464 2438 2386 2361 2309 2257 5 6 2051 2005 845 816 Patients 25 (%) Time to breast cancer death (HR-positive population) 20 15 A T HR 95% CI p-value HR+ 152 172 0.87 (0.70–1.09) 0.2 ITT 235 265 0.88 (0.74–1.05) 0.2 10 Anastrozole (A) Tamoxifen (T) 5 0 0 At risk: A 2618 T 2598 1 2566 2549 2 3 4 Follow-up time (years) 2505 2502 2437 2430 2377 2333 5 2117 2080 6 867 855 Overall survival (HR-positive population) Patients 25 (%) 20 15 A T HR 95% CI p-value HR+ 296 301 0.97 (0.83–1.14) 0.7 ITT 411 420 0.97 (0.85–1.12) 0.7 Anastrozole (A) 10 Tamoxifen (T) 5 0 0 At risk: A 2618 T 2598 1 2 2566 2549 2505 2502 Includes non breast cancer deaths 3 4 Follow-up time (years) 2437 2430 2377 2333 5 6 2117 2080 867 855 Summary of efficacy endpoints In the HR + population, compared with tamoxifen, anastrozole lowers the risk of : – all events: 17% (p=0.005) – recurrence: 26% (p=0.0002) – distant recurrence: 16% (p=0.06) – contralateral tumours: 53% (p=0.001) Yearly risk of recurrence in early breast cancer in untreated patients 10 9 8 7 6 5 4 3 2 1 0 1 5 Years 10 Adapted from EBCTCG meta-analysis. Lancet, 1998; 351:1451 Event rates for recurrence (HR-positive population) Annual hazard rate (%) 3.0 Substantial benefit with anastrozole in the first 3 years 2.5 2.0 1.5 1.0 Anastrozole Tamoxifen 0.5 0 0 1 2 3 4 Follow-up time (years) 5 6 Howell A. Breast Cancer Res Treat 2004; 88 (Suppl 1): S7, abs 1 Tolerability analysis Overview of adverse events Anastrozole (%) Tamoxifen (%) (n=3092) (n=3094) Adverse events leading to withdrawal* p-value 11.1 14.3 0.0002 6.5 8.9 0.0005 33.3 36.0 0.03 Serious adverse events leading to withdrawal 4.7 5.9 0.04 Serious adverse events leading to death 3.3 3.6 0.6 Drug-related serious adverse events leading to death 0.2 0.3 0.5 Drug-related adverse events leading to withdrawal* All serious adverse events *Adverse events on treatment or within 14 days of discontinuation Pre-defined adverse events Completion analysis Hot flushes Vaginal bleeding Vaginal discharge Endometrial cancer* Ischaemic cerebrovascular event Venous thromboembolic events Deep venous thromboembolic events Joint symptoms Total fractures** p-value A 35.7 5.4 3.5 0.2 2.0 T 40.9 10.2 13.2 0.8 2.8 <0.0001 <0.0001 <0.0001 0.02 0.03 2.8 4.5 0.0004 1.6 2.4 0.02 35.6 11.0 29.4 7.7 <0.0001 <0.0001 *Excludes patients with prior hysterectomy and includes on- and off-therapy AEs; **Fractures occurring at anytime prior to recurrence (includes patients no longer receiving treatment); pink text indicates p-value in favour of anastrozole and blue text in favour of tamoxifen Annual fracture rates over time Annual rates, %* 3 2.5 2 1.5 1 Anastrozole 1 mg od Tamoxifen 20 mg od 0.5 0 0 Number at risk Years 0 Arimidex 3092 Tamoxifen 3094 1 2 3 4 5 6 5 2070 2100 6 845 846 Years since randomisation 1 2923 2932 *Calculated using Kaplan-Meier estimates 2 2724 2741 3 2553 2579 4 2393 2401 Indirect fracture rate comparison Clinical study Setting Average age (years) Annual Fracture rate (%) ATAC (n=6,186) Early breast cancer (adjuvant) Anastrozole = 2.26 Tamoxifen = 1.56 PI (n=13,175) Breast cancer prevention WHI (n=16,608) Healthy women Age = 64 Age >50 (61%) Age = 63 Tamoxifen = 1.80 Placebo = 1.84 HRT = 1.48 Placebo = 1.91 ATAC Trialists’ Group. Lancet 2005; 365: 60–62 Fisher et al. J Natl Cancer Inst 1998; 90: 1371–1388 Women's Health Initiative Writing Group. JAMA 2002; 288: 321–333 Tolerability summary Compared with tamoxifen, anastrozole is associated with significantly fewer: – SAEs, treatment-related AEs and withdrawals due to SAEs or AEs – potentially life threatening AEs such as endometrial cancer, thromboembolic, and cerebrovasular events No new safety concerns have emerged with long-term follow-up Anastrozole is the only AI that has a mature tolerability profile covering the full 5 year treatment period ATAC Conclusions ATAC completed treatment analysis extends and strengthens the evidence that 5 years of anastrozole is significantly more effective and better tolerated than 5 years of tamoxifen Substantial benefits for anastrozole were seen within the first 3 years The efficacy benefit continues to increase with time and extends beyond the completion of therapy These data support using anastrozole as initial adjuvant therapy