Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
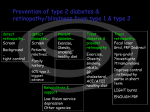
DIABETES AND YOUR EYES Josephine Carlos-Raboca, M.D. Makati Medical Center DIABETES MELLITUS ABNORMALITY IN GLUCOSE METABOLISM ALTERED INSULIN PRODUCTION OR ACTIVITY ELEVATED BLOOD SUGAR LEVELS NUMEROUS COMPLICATIONS ENORMOUS SOCIAL/ECONOMIC IMPACT ANATOMY OF THE EYE Mga Simtomas panlalabo ng paningin pagdilim ng paningin pagdoble ng paningin itim na ‘spots’ sa paningin EYE COMPLICATIONS CORNEAL ABNORMALITIES CATARACTS IRIS NEW VESSELS GLAUCOMA NEUROPATHIES RETINOPATHY CORNEAL PROBLEMS More prone to abrasions, infections Delayed/poor wound healing LENS Earliest sign is blurring of vision Drastic changes in blood sugar affects the grade of your eye Diabetics prone to develop cataracts earlier Diabetic Cataract Glaucoma A rise in the internal pressure of the eye Usually a result of the new vessels in the iris which block the outflow Neuropathies Can affect muscles that move the eye Or the optic nerve DIABETIC RETINOPATHY Normal Retina DIABETIC RETINOPATHY MOST COMMON CAUSE OF NEW CASES OF BLINDNESS 10-20% OF ALL NEW CASES OF BLINDNESS (US & EUROPE) INCREASING PREVALENCE DUE TO INCREASING SURVIVAL OF DM PATIENTS RISK FACTORS TYPE DURATION GLUCOSE CONTROL RENAL DISEASE SYSTEMIC HYPERTENSION ELEVATED SERUM LIPIDS PREGNANCY TYPE OF DIABETES MELLITUS 10-15%: Type 1 MAJORITY: Type 2 OCULAR COMPLICATIONS SIMILAR Type 1: HIGH INCIDENCE OF SEVERE OCULAR COMPLICATIONS/FASTER PROGRESSION Type 2: MAJORITY OF CLINICAL CASES OF EYE DISEASE DURATION DURATION 0-5 YEARS Type 1 Type 2 0% 10-15 YEARS 25-50% 23 -43% 15-29 YEARS 75-95% 60% 30+ YEARS 100% GLUCOSE CONTROL INTENSIVE GLUCOSE CONTROL REDUCED INCIDENCE AND PROGRESSION OF RETINOPATHY IN IDDM • Diabetes Control and Complications Trial GLYCOSYLATED Hg <7% RENAL DISEASE PROTEINURIA, ELEVATED BUN/CREA LEVELS: EXCELLENT PREDICTOR MICROANGIOPATHY AGGRESSIVE MANAGEMENT IS BENEFICIAL SYSTEMIC HYPERTENSION HTN + NEPHROPATHY: EXCELLENT PREDICTOR OF RETINOPATHY MAY BE SUPERIMPOSED MUST BE CONTROLLED ELEVATED SERUM LIPIDS MAY COMPLICATE RETINOPATHY INCREASES VESSEL LEAKAGE AND HARD EXUDATE FORMATION REASON???? PREGNANCY PREGNANT WOMEN W/O DM RETINOPATHY: 10% RISK FOR NPDR PREGNANT WOMEN WITH NPDR: 4% RISK FOR PDR THOSE WITH PDR: VERY POOR PROGNOSIS BASELINE AND STRICT FOLLOW UP RETINAL HEMORRHAGE HARD EXUDATES COTTON WOOL SPOTS NEOVASCULARIZATION RESPONSE TO SEVERE AND PROLONGED LACK OF OXYGEN ANGIOGENIC FACTORS GROWTH OF NEW BLOOD VESSELS IN THE RETINA POOR QUALITY OF VESSELS Normal Retina NEOVACULARIZATION VITREOUS HEMORRHAGE VITREOUS/PRERETINAL HEME TRACTIONAL DETACHMENT TRACTIONAL DETACHMENT STAGING/TERMINOLOGY “BACKGROUND” OR NON-PROLIFERATIVE DIABETIC RETINOPATHY (BDR/NPDR) PROLIFERATIVE DIABETIC RETINOPATHY (PDR) MILD BACKGROUND MODERATE BACKGROUND SEVERE BACKGROUND PROLIFERATIVE RETINOPATHY PROGNOSIS W/O TREATMENT MODERATE VISUAL LOSS IN BDR: 30% IN 3 YEARS SEVERE VISUAL LOSS( VISION LESS THAN 5/200) IN PDR: 35% YEARS IN 2 TREATMENT GLUCOSE CONTROL LASER THERAPY FOCAL PANRETINAL PHOTOCOAGULATION VITRECTOMY BP CONTROL LIPID CONTROL LASER THERAPY LASER THERAPY GOAL IS TO PRESERVE VISION !!! Improvement is secondary RECOMMENDATIONS Get at Baseline DILATED eye exam Type 1 DM: FIVE YEARS AFTER DIAGNOSIS Type 2 DM: IMMEDIATELY AFTER DIAGNOSIS GESTATIONAL DM: DURING 1ST TRIMESTER IMMEDIATE EXAM IF SYMPTOMATIC RECOMMENDATIONS MILD BDR: YEARLY EXAM MODERATE BDR: EVERY 4-8 MONTHS SEVERE BDR: EVERY 2-4 MONTHS PDR: IMMEDIATE LASER TX THEN EVERY 2-4 MONTHS UNTIL STABLE THANK YOU!