Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Management of acute coronary syndrome wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Heart failure wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Electrocardiography wikipedia , lookup
Coronary artery disease wikipedia , lookup
Pericardial heart valves wikipedia , lookup
Myocardial infarction wikipedia , lookup
Cardiac surgery wikipedia , lookup
Aortic stenosis wikipedia , lookup
Artificial heart valve wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Ventricular fibrillation wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
Atrial septal defect wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
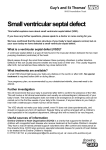
Morphologic demonstration of spontaneous and surgical closure of membranous ventricular septal defect Jong Mi Ko, BA, Joseph E. Guileyardo, MD, Jun Zhang, MD, and William C. Roberts, MD This report demonstrates morphologic features of membranous ventricular septal defect that was closed spontaneously in one patient and operatively in the other. R elatively few reports have illustrated morphologically either spontaneous or surgical closure of membranous ventricular septal defect (VSD) (1–10). Such is the purpose of this report. DESCRIPTION Certain findings in each of the two patients are summarized in Table 1. Patient 1 died from multisystem failure, primarily consequences of severe obesity. Necropsy disclosed an isolated membranous VSD that had closed spontaneously by the adhesion of the septal tricuspid valve leaflet to the margins of the defect (Figure 1). A small, thin layer of fibrous Table 1. Certain clinical and necropsy findings in the two white men with a membranous ventricular septal defect that was closed by two different mechanisms Variables Type of closure Patient 1 Patient 2 Spontaneous Surgical Age (years) at examination of heart 71 48 Age (years) at surgical closure of VSD – 5 44.5 19.8 0 + Body mass index (kg/m2) Precordial murmur Heart block Complete – ICD/pacemaker + + Died + 0 (Transplant) 515 600 Myocardial infarct 0 +* Heart floated in formaldehyde + 0 Heart weight (g) *Secondary to operative damage of the left circumflex coronary artery at the time of mitral valve replacement for severe mitral regurgitation at age 32. ICD indicates implantable cardioverter defibrillator; VSD, ventricular septal defect; –, not available. 514 tissue presumably produced by the left-to-right shunt jet flow through the VSD was present on the mural endocardium in the right ventricular outflow tract in apposition to the “VSD.” Patient 2 had an atrioventricular canal defect, which was closed at age 5 years. At age 31 years, he was found to have severe mitral regurgitation and underwent mitral valve replacement with inadvertent left circumflex coronary artery injury, resulting in one-vessel coronary artery bypass grafting. He developed heart failure symptoms at age 47 and underwent heart transplantation a year later. Pathologic examination of the native heart revealed the surgically closed previous membranous VSD (Figure 2). DISCUSSION Both patients presented in this report had VSDs located immediately caudal to the right aortic valve cusp. One closed spontaneously and the other by operative insertion of a patch. Spontaneous closure of VSD appears to be much more common than operative closure. Although this report focuses exclusively on the membranous location of VSD, muscular VSD, although much less common than the membranous variety, probably has a higher rate of spontaneous closure than does the membranous variety. The result of spontaneous closure can easily be missed at necropsy if the entire ventricular septum is not carefully examined. 1. 2. 3. 4. Albers HJ, Carroll SE, Coles JC. Spontaneous closure of a membranous ventricular septal defect. Necropsy finding with clinical application. Br Med J 1962;2(5313):1162–1163. Roberts WC, Morrow AG, Mason DT, Braunwald E. Spontaneous closure of ventricular septal defect, anatomic proof in an adult with tricuspid atresia. Circulation 1963;27:90–94. Simmons RL, Moller JH, Edwards JE. Anatomic evidence for spontaneous closure of ventricular septal defect. Circulation 1966;34(1):38–45. Suzuki H, Lucas RV Jr. Spontaneous closure of ventricular septal defects. Anatomic evidence in three patients. Arch Pathol 1967;84(1):31–36. From the Baylor Heart and Vascular Institute (Ko, Zhang, Roberts) and the Department of Pathology (Guileyardo, Roberts), Baylor University Medical Center at Dallas. Corresponding author: William C. Roberts, MD, Baylor Heart and Vascular Institute, Baylor University Medical Center at Dallas, 3500 Gaston Avenue, Dallas, TX 75246 (e-mail: [email protected]). Proc (Bayl Univ Med Cent) 2015;28(4):514–515 a b Figure 1. Case 1. Photographs of the basal portion of the heart. (a) Membranous ventricular septal defect (VSD) located immediately below the right aortic valve cusp was spontaneously closed by the septal tricuspid valve leaflet. (b) A close-up of spontaneous closure of VSD showing the adherence of the tricuspid valve leaflet (arrow) to the margins of the defect and a dead-end tunnel-like space between the top and bottom portion of the defect. AML indicates anterior mitral leaflet; ATL, anterior tricuspid leaflet; AV, aortic valve; PML, posterior mitral leaflet; RV, right ventricle; STL, septal tricuspid leaflet; VS, ventricular septum. a b c Figure 2. Case 2. Photographs of the basal portion of the heart. (a) Membranous ventricular septal defect (VSD) located immediately below the right aortic valve cusp was closed surgically at age 5 years. (b) A close-up of the surgically closed VSD shows a Teflon patch (arrow) located at the junction of the anterior and septal tricuspid leaflet just below the aortic valve. (c) A deeper cut of the surgically closed VSD shows the relation of the “defect” to the aorta and aortic valve. ATL indicates anterior tricuspid leaflet; AV, aortic valve; LV, left ventricle; STL, septal tricuspid leaflet; TV, tricuspid valve; VS, ventricular septum. 5. 6. 7. Glancy DL, Roberts WC. Complete spontaneous closure of ventricular septal defect: necropsy study of five subjects. Am J Med 1967;43(6):846– 853. Collins G, Disenhouse R, Keith JD. Spontaneous closure of ventricular septal defect. Can Med Assoc J 1969;100(16):737–743. Tandon R, Edwards JE. Aneurysmlike formations in relation to membranous ventricular septum. Circulation 1973;47(5):1089–1097. October 2015 8. Marino B, Loperfido F, Sardi CS. Spontaneous closure of ventricular septal defect in a case of double outlet right ventricle. Br Heart J 1983;49(6):608–611. 9. Anderson RH, Lenox CC, Zuberbuhler JR. Mechanisms of closure of perimembranous ventricular septal defect. Am J Cardiol 1983;52(3):341–345. 10. Gaines JJ, Rao RN. Closure of membranous ventricular septal defect of heart by septal leaflet of tricuspid valve. Hum Pathol 1983;14(12):1082–1084. Morphologic demonstration of spontaneous and surgical closure of membranous ventricular septal defect 515