Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Yellow fever wikipedia , lookup
Hepatitis B wikipedia , lookup
Sexually transmitted infection wikipedia , lookup
Creutzfeldt–Jakob disease wikipedia , lookup
Dirofilaria immitis wikipedia , lookup
Trichinosis wikipedia , lookup
Brucellosis wikipedia , lookup
Gastroenteritis wikipedia , lookup
Meningococcal disease wikipedia , lookup
Typhoid fever wikipedia , lookup
Chagas disease wikipedia , lookup
Sarcocystis wikipedia , lookup
Onchocerciasis wikipedia , lookup
Marburg virus disease wikipedia , lookup
Visceral leishmaniasis wikipedia , lookup
Middle East respiratory syndrome wikipedia , lookup
Rocky Mountain spotted fever wikipedia , lookup
Hospital-acquired infection wikipedia , lookup
Leishmaniasis wikipedia , lookup
Oesophagostomum wikipedia , lookup
African trypanosomiasis wikipedia , lookup
Schistosomiasis wikipedia , lookup
Eradication of infectious diseases wikipedia , lookup
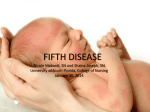
What’s Your Diagnosis? Slapped Cheeks Vanessa Hum, BASc; and Simon Lee, MD, FRCPC A 10-year-old previously healthy boy developed a three-day history of prodromal symptoms including: • low grade fever, • sore throat and • malaise. Just when his mother thought he was improving, the young boy suddenly developed bright red cheeks associated with a widespread eruption on his upper body. There is no history of drug ingestion. Figure 1. Frontal view of cheeks with “slapped cheek” appearance. Examination reveals a well nourished male in no apparent distress. Bright red plaques are © noted on both cheeks associated with circum, oa d l n oral pallor and relative sparing of the nasolabiow n d use a c al folds. The conjunctivae and oropharynx are l s ser rsona u d e clear. Bilateral shotty cervical lymph nodes are rp ise hor opy fo t u palpable. Scattered red papules and plaques are c .A ited single noted on the trunk, forming a lacyhib pattern. ro ta Palms and soles are clear. use p d prin t h is g D i l r y cia ion t u trib Copommer rC o le a S r ed an oauthorisay, view f t o is Uyour n What diagnosis? ispl N d a. b. c. d. e. Chickenpox Molluscum contagiosum Erythema infectiosum HPV infection Rocky Mountain spotted fever Answer: Erythema infectiosum (EI) (fifth disease) Figure 2. Lateral view with erythema extending to the ears. About EI EI is usually a benign, self-limited childhood illness caused by Human Parvovirus B19. It is also commonly referred to as the “slapped cheek disease” due to its dramatic clinical presentation. Historically, EI is the “fifth” disease in the nomenclature description of the six classic childhood exanthems. They include: 1. Measles 2. Scarlet fever The Canadian Journal of Diagnosis / April 2010 33 What’s Your Dx? 3. Rubella 4. Duke’s disease (existence controversial) 5. EI 6. Roseola EI is transmitted primarily by respiratory secretions as well as infected blood. The incubation period ranges from one to three weeks. Twothirds of cases occur in the age group of five- to 15-years-old. There is no sex predilection. Patients are no longer infectious upon appearance of exanthem. Community outbreaks typically occur in the winter time in nurseries and schools. Sporadic cases are infrequent. ommunity outbreaks typically occur in the winter time in nurseries and schools. Sporadic cases are infrequent. C Complications may occur, particularly in high-risk groups. Symmetrical polyarthritis of the small joints (e.g., fingers and feet) may develop, primarily in adults. Vertical transmission of the infection in pregnant women has been linked to hydrops fetalis and spontaneous abortion. In patients with underlying chronic hemolytic anemias such as sickle cell disease, thalassemia or immunodeficiency states such as leukemia, EI infection may trigger aplastic crisis due to cytotoxic destruction of erythropoietic cells in the bone marrow. IV immunoglobulin may be of benefit in these cases. Fortunately, the majority of patients have an excellent prognosis and recover spontaneously in several weeks to two months time. Treatment is symptomatic and may include bed rest, topical steroid creams and analgesic/anti-inflammatory agents. Cutaneous relapses may occur, aggravated by sunlight exposure and exercise. Dx Dr. Lee is a Dermatologist, Richmond Hill, Ontario. Ms. Hum is a Chemical Engineer, Ottawa, Ontario.