Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Pharmacokinetics wikipedia , lookup
Drug interaction wikipedia , lookup
Psychedelic therapy wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Plateau principle wikipedia , lookup
Intravenous therapy wikipedia , lookup
Theralizumab wikipedia , lookup
Discovery and development of direct thrombin inhibitors wikipedia , lookup
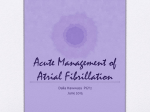
Management of New Onset Atrial Fibrillation William E Lawson, MD Professor of Medicine SUNY, Stony Brook Magnitude of the Problem • AF is the most common tachyarrhythmia requiring therapy and the most common arrhythmia leading to hospitalization. • AF patients have increased mortality and impaired quality of life. – Associated with the AF – Associated with its therapy • Economic costs are in the billion of $/yr range Question #1 An 82 year old man is in your office for an annual Medicare physical. What is the chance he has atrial fibrillation? 1. 1% 2. 5% 3. 10% 4. 25% Prevalence of Diagnosed AF Stratified by Age and Sex 12.0 10.0 Women Men 11.1 10.3 9.1 8.0 7.3 6.0 5.0 4.0 3.0 1.7 2.0 0.0 0.1 0.2 0.4 <55 0.9 7.2 5.0 x-axis = % y-axis = # of men/women 3.4 1.7 1.0 55-59 60-64 65-69 70-74 75-79 80-84 > 85 # Women 530 310 566 896 1498 1572 1291 1132 # Men 1529 634 934 1426 1907 1886 1374 759 Go AS, JAMA. 2001 May 9;285(18):2370-5. Pub Med PMID: 11343485 Question #2 A 46 year old male patient is in for an annual physical exam. What is his lifetime risk of developing AF? 1. 1% 2. 5% 3. 10% 4. 25% Incidence of AF Lifetime Risk for AF at Selected Index Ages by Sex Index Age, yrs Men Women 40 26.0% (24.0 – 27.0) 23.0% (21.0 – 24.0) 50 25.9% (23.9 – 27.0) 23.2% (21.3 – 24.3) 60 25.8% (23.7 – 26.9) 23.4% (21.4 – 24.4) 70 24.3% (22.1 – 25.5) 23.0% (20.9 – 24.1) 80 22.7% (20.1 – 24.1) 21.6% (19.3 – 22.7) 1 in 4 Men & women >40 Years will develop AF Lifetime risk if currently free of AF Lloyd-Jones DM, et al. Circulation. 2004 Aug 31;110(9):1042-6. Pub Med PMID: 15313941. Atrial Fibrillation Definitions Term Definition Paroxysmal A Fib Terminates spontaneously or with Rx within 7 days Persistent A Fib Continuous A Fib sustained ≥ 7 days Long-standing persistent A Fib Continuous A Fib ≥ 12 months duration Permanent A Fib Joint decision of Pt and Physician to stop attempts to restore or maintain sinus rhythm Nonvalvular A Fib A Fib in absence of rheumatic mitral stenosis, valve replacement or mitral repair Magnitude of the Problem • Inadequate recognition and treatment • Controversy regarding optimal approach, therapy is evolving – Rate versus rhythm control – Antiarrhythmic drug (AAD) vs nonpharmacologic therapy – Hybrid therapies – Anticoagulation/ bleeding risk AF Comorbidities/ Risk Factors (Top Offenders) • • • • Hypertension Diabetes mellitus Hyperthyroidism Hypertrophic cardiomyopathy • Congestive heart failure • Valvular heart disease • Pericardial disease • Obstructive sleep apnea • Pulmonary disorders • Obesity • Alcohol • Stimulants • Occasionally ischemic heart disease • Post CT surgery Comorbidity Resulting from AF • Congestive heart failure – Tachycardia [>120 bpm] mediated cardiomyopathy – Loss of atrial kick • Stroke – Thromboembolic (usually LAA) – Risk increases with advancing age and other risk factors [CHA2DS2-VASc score] Overview of AF Management AF Detected Management of Arrhythmia Assessment of Thromboembolic Risk (CHADS2) ASA OAC Rate Control No antithrombotic therapy may be appropriate in selected young patients with no stroke risk factors Rhythm Control Dr. YD, Age 42, Family Practitioner • Last evening he was out celebrating the marriage of his receptionist and consumed about 12 ounces of Johnny Walker Black label. • He went home by taxi, slept poorly and realized this morning about 6:00 am that his heart rate was rapid and pulse irregular. • He has a mild bitemporal headache and is driven to the ED by his wife. • He has been well, no known hypertension, DM, heart disease, TIA/stroke and no known arrhythmias although he does have mild palpitations from time to time. No COPD or asthma. • In ED: no chest pain, mild SOB, slightly sweaty. HR 140, irregularly irregular, BP 140/90, JVD 4 cm, Chest clear. ECG shows AF, rate 140. Dr. YD, Age 42, Family Practitioner How will you manage his rhythm? 1. Electrical cardioversion (150-200 j) in ED as soon as it can be done. 2. IV metoprolol 5 mg, repeated Q 5 min up to 3 times if rate remains above 110. Home on po metoprolol 50-100 mg bid if AF persists. 3. IV metoprolol 5 mg, repeated Q 5 min up to 3 times if rate remains above 110. Add propofenone 450 mg po about 10-15 minutes after first dose of metoprolol if AF persists. 4. IV metoprolol 5 mg, repeated Q 5 min up to 3 times if rate remains above 110. Electrical cardioversion if AF persists. 5. Digoxin 0.25 mg IV, repeat at 1 hour intervals up to 4 doses if AF persists. How will you manage his rhythm? 1.Electrical cardioversion (150-200 j) in ED as soon as it can be done. 2.IV metoprolol 5 mg, repeated Q 5 min up to 3 times if rate remains above 110. Home on po metoprolol 50-100 mg bid if AF persists. 3.IV metoprolol 5 mg, repeated Q 5 min up to 3 times if rate remains above 110. Add propofenone 450 mg po about 10-15 minutes after first dose of metoprolol if AF persists. 4.IV metoprolol 5 mg, repeated Q 5 min up to 3 times if rate remains above 110. Electrical cardioversion if AF persists. Best answer! * 5.Digoxin 0.25 mg IV, repeat at 1 hour intervals up to 4 doses if AF persists. *This is a young man with no stroke risk factors. His AF has been present for only a few hours. It is likely the AF was precipitated by his alcohol indiscretion and he is likely to return to NSR with cardioversion and likely to remain in sinus rhythm. Accordingly, electrical cardioversion is a good option. It makes sense to give IV metoprolol to slow his rate before cardioversion. The cardioversion may be done without prior anticoagulation. He requires no ongoing OAC or ASA. Hence, the best answer is #4. #3 would be acceptable if there is some reason not to do electrical cardioversion, or if there is any expectation that he may have recurrent episodes of AF and might be suitable for a pill in the pocket regimen, but this does not appear indicted in this first presentation of AF. #2 is OK, but in a young person with acute onset, electrical (or pharmacological) cardioversion has a high likelihood of resolving the AF. #1 is not advised since there is no rush to cardiovert him and giving metoprolol will be likely to decrease symptoms prior to cardioversion. #5 would not be a good choice. Atrial Fibrillation in the ED Is Patient Stable? Immediate Risk for Stroke? Low Risk 1. Clear onset <48 hours, or 2. Therapeutic OAC ≥ 3 wks Pharmacological or electrical CV at 150-200 J (Immediate anticoagulation in ED before CV not required) * Antithrombotic therapy -Initiate OAC upon discharge from ED (or continue current OAC) if age ≥ 65 or CHADS2 ≥ 1 -Otherwise, initiate ASA if CAD or vascular disease -Early follow-up to review long-term OAC YES NO High Risk** No therapeutic OAC ≥ 3 weeks and one of: 1. Onset >48 hours or unknown, or 2. Stroke/TIA <6 months or 3. Mechanical or rheumatic valve disease. Rate-control Therapeutic OAC for 3 Trans-esophageal weeks before echocardiography (TEE) outpatient CV guided CV Antithrombotic therapy - Continue OAC for ≥4 weeks after CV - Early follow-up to review long-term OAC Antithrombotic therapy - Initiate immediate OAC* in ED and continue for ≥4 weeks - Early follow-up to review long-term OAC Unstable – AF causing: 1. Hypotension, or 2. Cardiac ischemia, or 3. Pulmonary edema Consider urgent electrical CV if rate control not effective Antithrombotic therapy - Initiate immediate OAC* in ED and continue for ≥4 weeks if any ‘high risk’ ** features present - Early follow-up to review long-term OAC Emergency Management of AF * Immediate OAC = a dose of OAC should be given just prior to cardioversion - either a novel direct oral anticoagulant (NOAC) or a dose of heparin or low molecular weight heparin with bridging to warfarin if a NOAC is contraindicated. Dr. YD, Age 42, Family Practitioner How will you reduce his risk of stroke if you decide to cardiovert him? 1. IV LMWH or a NOAC po about 1 hour prior to any cardioversion attempt. 2. IV LMWH or a NOAC po about 1 hour prior to electrical cardioversion, but not required for pharmacologic cardioversion. 3. No anticoagulant required pre cardioversion attempt. 4. Start dabigatran 150 mg bid and have him return for cardioversion after 3 weeks of dabigatran. How will you reduce his risk of stroke if you decide to cardiovert him? 1. IV LMWH or a NOAC po about 1 hour prior to any cardioversion attempt. 2. IV LMWH or a NOAC po about 1 hour prior to electrical cardioversion, but not required for pharmacologic cardioversion. 3. No anticoagulant required pre cardioversion attempt. Best answer! He is young, has no risk factors for stroke, and the duration of AF has been short. The risk of a stroke with cardioversion and no anticoagulation is very low. He requires no anticoagulation pre cardioversion. 4. Start dabigatran 150 mg bid and have him return for cardioversion after 3 weeks of dabigatran. How will you reduce his risk of stroke post discharge from ED? 1. If AF persists, he requires maintenance ASA 81 mg daily at least until follow-up at 1 month. 2. Whether AF persists or resolves, he requires maintenance ASA 81 mg at least until follow-up at 1 month. 3. If AF persists, he requires maintenance OAC at least until followup at 1 month. 4. Whether AF persists or resolves, he requires maintenance OAC at least until follow-up at 1 month. 5. Whether AF persists or resolves, he requires no maintenance antithrombotic therapy. How will you reduce his risk of stroke post discharge from ED? 1. If AF persists, he requires maintenance ASA 81 mg daily at least until follow-up at 1 month. 2. Whether AF persists or resolves, he requires maintenance ASA 81 mg at least until follow-up at 1 month. 3. If AF persists, he requires maintenance OAC at least until follow-up at 1 month. 4. Whether AF persists or resolves, he requires maintenance OAC at least until follow-up at 1 month. 5. Best Answer! Whether AF persists or resolves, he requires no maintenance antithrombotic therapy. - He is young, has no risk factors for stroke. He fits the CCS algorithm of no antithrombotic therapy for AF. New CCS Algorithm 80 year old female with hypertension • She lives alone with her dog. She is without other significant medical problems other than obesity [5 feet 5 inches, 190 lbs]. • Medications: Ramipril 10 mg/d, bisoprolol 5mg/d. • Comes to the office for routine BP follow-up. Her BP is 145/85 on repeat readings, pulse is 85 bpm and irregularly irregular. No heart murmurs or clinical evidence of heart failure. • With further discussion she admits to a decrease in exercise tolerance and increase in fatigue and dyspnea on exertion. • ECG demonstrates atrial fibrillation with a ventricular response of 88. What next? Why does she have AF? 1. Thyroid 2. Hypertension 3. Sleep apnea 4. Ethanol 5. Obesity History Establish Severity (including impact on QOL) Identify Etiology Identify reversible causes (hyperthyroidism, ventricular pacing, SVT, exercise) Identify factors whose treatment could reduce recurrent AF or improve overall prognosis (i.e. hypertension, sleep apnea, left ventricular dysfunction) Identify potential triggers (i.e. alcohol, intensive aerobic training) Identify potentially heritable causes of AF (particularly in lone AF) Determine thromboembolic risk (e.g. CHA2DS2 - VASc Score) Determine bleeding risk to guide antithrombotic therapy (HASBLED) Review prior pharmacologic therapy for AF, for efficacy and adverse effects Rate vs Rhythm; Effect on Mortality ? Rate or Rhythm control • Quality of Life significantly affected by atrial fibrillation • Choices: – More tightly control heart rate (increase BB) – Attempt to restore sinus rhythm • CHA2DS2- VASc score = 4 [4.0% annual risk of CVA] • TT Echocardiogram to assess valves, LA and LV size and function. • OAC for 3 weeks of therapeutic anticoagulation prior to attempted Electrical Cardioversion. Continue anticoagulation regardless of result. Rate vs Rhythm Control for with Symptomatic AF SYMPTOMATIC AF ATTEMPT RATE CONTROL Beta-blocker Calcium channel blocker Special circumstances in which to consider early rhythm control: Highly symptomatic Multiple recurrences Extreme impairment in QOL Arrhythmia-induced cardiomyopathy YES SYMPTOMS RESOLVE NO CONTINUE RATE CONTROL MODIFY RATE CONTROL - CONSIDER RHYTHM CONTROL Paroxysmal AF Low burden recurrence Pill in pocket antiarrhythmic therapy High burden recurrence Maintenance antiarrhythmic therapy Catheter ablation Persistent AF Consider cardioversion Symptoms Symptoms improve, improve, and patient but AF recurs maintains sinus rhythm Symptoms don’t change in sinus rhythm and AF recurs Observe. If AF recurs, determine if symptomatic Overview of AF Management AF Detected Assessment of Thromboembolic Risk (CHADS2) Appropriate Antithrombotic Therapy Detection and Treatment of Precipitating Causes Management of Arrhythmia Rate Control Rhythm Control Rhythm Control in A Fib Rhythm Control Choices Normal Systolic Function No Hx of CHF Dronedarone+ Flecainide* Propafenone* Sotalol# Rhythm Control Choices Hx of CHF or Left Ventricular Systolic Dysfunction EF > 35% EF ≤ 35% Amiodarone Sotalol** Amiodarone Catheter Ablation Amiodarone Catheter Ablation Drugs are listed in alphabetical order + Dronedarone should be used with caution in combination with digoxin • Class I agents should be AVOIDED in CAD and should be COMBINED with AV-nodal blocking agents # Sotalol should be used with caution in those at risk for torsades de pointes VT (e.g. female, age > 65 yr, taking diuretics) ** Sotalol should be used with caution with EF 35-40% and those at risk for torsades de pointes VT (e.g. female, age > 65 yr, taking diuretics) Rate Control in A Fib Rate Control Drug Choices Heart Failure CAD No Heart Failure or CAD β-blocker ± Digoxin β-blocker* Calcium Channel Blocker# Combination Rx β-blocker* Calcium Channel Blocker# Digoxin† Combination Rx Drugs are listed in alphabetical order *β-blockers preferred in CAD # Non-dihydropyridine calcium channel blockers (diltiazem, verapamil) †Digoxin may be considered as monotherapy only in particularly sedentary individuals Rate Control Drugs ß-Blockers Drug Dose Adverse Effects Atenolol 50 - 150 mg p.o. daily bradycardia, hypotension, fatigue, depression Bisoprolol 2.5 - 10 mg p.o. daily as per atenolol Metoprolol 25 mg - 200 mg p.o. bid as per atenolol 20 - 160 mg p.o daily - bid as per atenolol 80 - 240 mg p.o. tid as per atenolol Nadolol Propranolol Calcium Channel Blockers and Digoxin Drug Dose Adverse Effects Verapamil 120 - 480 mg p.o. daily 120 - 240 mg p.o. bid bradycardia, hypotension, constipation Diltiazem 120 - 480 mg p.o. daily 120 - 240 mg p.o. bid bradycardia, hypotension, ankle swelling Digoxin 0.0625 mg - 0.25 mg p.o. daily bradycardia, nausea, vomiting,visual disturbance Rhythm Control - Drugs Drug/Dose Flecainide 50-150 mg BID Propafenone 150-300 mg TID Amiodarone 100-200 mg OD (after 10g loading) Dronedarone 400 mg BID Sotalol 80-160 mg BID Efficacy Toxicity Comments 30-50% Ventricular tachycardia Bradycardia Rapid ventricular response to AF or atrial flutter (1:1 conduction) Contraindicated in patients with CAD or LV dysfunction Should be combined with an AV nodal blocking agent 30-50% Ventricular tachycardia Bradycardia Rapid ventricular response to AF or atrial flutter (1:1 conduction) Abnormal taste Contraindicated in patients with CAD or LV dysfunction Should be combined with an AV nodal blocking agent 60-70% Photosensitivity, Bradycardia, GI upset, Thyroid dysfunction, Hepatic toxicity, Neuropathy, Tremor, Pulmonary toxicity, Torsades de pointes (rare) Low risk of proarrhythmia Limited by systemic side effects Most side effects are dose & duration related GI upset Bradycardia Hepatic toxicity Should not be used for rate control or for rhythm control in patients with a history of CHF or LV EF < 40%. Should be used with caution when added to digoxin. Liver enzyme monitoring required. New agent – limited experience outside clinical trials. Torsades de pointes Bradycardia Beta-blocker side effects Should be avoided in patients at high risk of torsades de pointes VT – especially women >65 years taking diuretics or those with renal insufficiency QT interval should be monitored 1 week after starting Use cautiously when EF<40% 40% 30-50% New Rate/Rhythm Algorithm Changes in A Fib Management 1. 2. 3. 4. 5. 6. Removal of Class 1A antiarrhthymic agents. Potential use of “pill-in-pocket” approach. Increasing role for catheter ablation. Novel oral anticoagulants. Assessment of bleeding risk. Joint decision making patient and physician “Pill-in-Pocket” Approach • Paroxysmal and sporadic AF may be treated with intermittent rather than daily AAD therapy. • Self administration of AAD: – Improves QOL, decreases hospitalizations, reduces treatment costs • Class 1C drugs are recommended (propafenone & felecainide) for their efficacy, rapid action, and safety. – Low organ toxicity, low proarrhythmia risk Role of Catheter Ablation • Catheter ablation is reasonable in patients with symptomatic atrial fibrillation. • Radiofrequency ablation may be preferred in symptomatic young patients. • May be an effective adjunct procedure in pts undergoing cardiac surgery (e.g. cardiac bypass, mitral valve repair). Limitations of Catheter Ablation • Limited data on long term efficacy. • Recurrence rates of 10- 44% have been reported. • Major complication rate is 1-6%. • Embolic stroke has an incidence of 0-5%. • Results dependent on operator expertise. AF Ablation • First line therapy for patients in whom anticoagulation is contraindicated? • First line therapy for patients who will be noncompliant with chronic anticoagulation? • First line therapy for patients who do not wish to be chronically anticoagulated? Who is a Candidate for AF Ablation? • Symptomatic AF (paroxysmal or persistent). • At least 1 antiarrhythmic drug failure. • Younger pts with “lone” paroxysmal AF are the best candidates, but pts with persistent AF, older pts, and those with comorbidities (structural heart disease, CHF) may also be appropriate candidates. Consensus Indications for Catheter Ablation of Atrial Fibrillation Indications for Catheter Ablation of AF Class LOE Symptomatic AF refractory or intolerant to at least 1 class 1 or class 3 antiarrhythmic medication Paroxysmal AF: Catheter ablation is recommended* I A Persistent AF: Catheter ablation is reasonable IIa B Longstanding persistent AF: Catheter ablation may be considered IIb B Symptomatic AF before initiation of antiarrhythmic drug therapy with a class 1 or class 3 antiarrhythmic agent Paroxysmal AF: Catheter ablation is reasonable IIa B Persistent AF: Catheter ablation may be considered IIb C Longstanding persistent AF: Catheter ablation may be considered IIb C Electroanatomic map of the left atrium (left), with dots marking areas of radiofrequency energy delivered during ablation. Chinitz J S et al. Circulation 2013;127:408-416 Copyright © American Heart Association Bleeding Risk Scores in AF ATRIA HAS-BLED HEMORR2HAGES Anemia1 3 Hypertension4 1 Hepatic10 or disease2 1 1 Severe renal disease2 3 Abnormal Renal5 or 1 1 Ethanol abuse 1 Age ≥75 yrs 2 Stroke 1 Malignancy 1 Any prior hemorrhage 1 Bleeding 1 Older Age (>75 yrs) 1 Hypertension3 1 Labile INR8 1 Reduced platelet number 1 Elderly (>65 yrs) 1 Rebleeding12 2 Drugs9 or 1 1 Hypertension4 1 Anemia13 1 Genetic factors14 1 Excessive fall risk15 1 Stroke 1 1. 2. 3. 4. 5. 6. 8. 9. 10. 11. 12. 13. 14. 15. Liver function6 Alcohol Hemoglobin <13 g/dl men; <12 g/dl women Estimated glomerular filtration rate <30 ml/min or dialysis-dependent Diagnosed hypertension Systolic blood pressure >160 mmHg Presence of chronic dialysis or renal transplantation or serum creatinine ≥200 mmol/L Chronic hepatic disease (eg cirrhosis) or biochemical evidence of significant hepatic derangement (eg bilirubin 2 x upper limit of normal, in association with aspartate aminotransferase/alanine aminotransferase/alkaline phosphatase >3 x upper limit normal, etc.) Unstable/high INRs or poor time in therapeutic range (eg <60%) Concomitant use of drugs, such as antiplatelet agents, non-steroidal anti-inflammatory drugs, or alcohol abuse etc. Cirrhosis, two-fold or greater elevation of AST or APT, or albumin <3.6 g/dl Platelets <75,000, use of antiplatelet therapy (eg daily aspirin) or NSAID therapy; or blood dyscrasia Prior hospitalization for bleeding Most recent hematocrit <30 or hemoglobin <10 g/dl CYP2C9*2 and/or CYP2C9*3 Alzheimer's dementia, Parkinson's disease, schizophrenia, or any condition predisposing to repeated falls Renal or function11 Apostolakis S, Lane DA, Guo Y, Buller H, Lip GY. J Am Coll Cardiol 2012;60:000–000. 2012 Jul 24. [Epub ahead of print] Online Appendix. PMID: 22858389. AMADEUS Cohort Stratified by the HEMORR2HAGES, HAS-BLED, and ATRIA Schemes All Patients Clinically Relevant Bleeding Major Bleeding 1,738 (76.6) 182 (10.5) 25 (1.4) 517 (22.8) 63 (12.2) 13 (2.5) 13 (0.5) 3 (23.1) 1 (7.7) 2,268 248 (10.9) 39 (1.7) Low Risk (<3) 1,739 (75.9) 159 (9.1) 22 (1.3) High Risk (≥3) 553 (24.1) 92 (16.6) 17 (3.1) 2,292 251 (11.0) 39 (1.7) Scheme HEMORR2HAGES Low (≤1) Risk Intermediate Risk (2–3) High Risk (>3) TOTAL HAS-BLED TOTAL ATRIA Low Risk (<4) 2,038 (90) 220 (10.8) 31 (1.5) Intermediate Risk (4) 102 (4.4) 13 (12.7) 3 (2.9) High Risk (>4) 128 (5.6) 18 (14.1) 5 (3.9) 2,268 248 (10.9) 39 (1.7) TOTAL Apostolakis S, Lane DA, Guo Y, Buller H, Lip GY. J Am Coll Cardiol 2012;60:000–000. 2012 Jul 24. [Epub ahead of print] Online Appendix. PMID: 22858389. 44 CVA & Bleeding Rates CHA2DS2VASc Score Adjusted Thromboem bolism Rate, %/y† HAS-BLED Score Major Bleeding Rate, %/y‡ 1.9 0 0 0 0 1 2.9 1 1.3 1 1.2 2 4.0 2 2.2 2 2.2 3 5.9 3 3.2 3 5.9 4 8.5 4 4.0 4 7.0 5 12.5 5 6.7 5–6 19.4 6 18.2 6 9.8 7 9.6 8 6.7 9 15.2 Adjusted Stroke Rate, %/y* 0 CHADS2 Score Advantages of new oral anticoagulants (NOACs) over vitamin K antagonists (VKAs) for thromboembolic prevention in patients with non-valvular AF • predictable effect without need for monitoring • fewer food and drug interactions • more predictable half-life/elimination • improved efficacy/safety ratio www.escardio.org/EHRA 1 Checklist during follow-up of AF patients on NOACs Interval Comments Compliance Each visit Inspect remaining medication Stress importance of compliance Inform about compliance aids Thrombo-embolism Each visit Cerebral, systemic and pulmonary circulation Bleeding Each visit Side effects Each visit Co-medications Each visit “Nuisance” bleeding – prevention possible? Bleeding with risk or impact on QoL – prevention possible? Need to revise dose? Continuation? Temporary cessation with bridging? Change of anticoagulant drug? Prescription or over-the counter drugs? Even temporary use can be risky Yearly 6-monthly Haemoglobin, renal, liver function Renal function if CrCl 30-60 ml/min or if on dabigatran and aged >75 years or fragile 3-monthly on indication If CrCl 15-30 ml/min If intercurring condition may impact renal or hepatic function. Blood sampling www.escardio.org/EHRA 8 Drug-drug interactions and pharmacokinetics of NOACs Absorption and metabolism of NOACs www.escardio.org/EHRA 15 Absorption and metabolism of NOAC Dabigatran Apixaban Edoxaban 3-7% 50% 62% yes no no 66% (w/o food) ~100% with food no 20%/80% 73%/27% 50%/50% 65%/35% no yes (elimination; minor CYP3A4) minimal (<4% of elimination) yes (elimination) no effect no effect 6-22% more +39% no no no official recommendation yet mandatory Absorption with H2B/PPI plasma level -12 to -30% no effect no effect no effect Asian ethnicity plasma level +25% no effect no effect no effect dyspepsia 5-10% no problem no problem no problem 12-17h 12h 9-11h 5-9h (young)/11-13h (elderly) Bioavailability Prodrug Clearance: non-renal/renal of adsorbed dose if normal renal function Liver metabolism: CYP3A4 Absorption with food Intake with food? GI tolerability Elimination half-life www.escardio.org/EHRA 16 Rivaroxaban Drug-drug interactions – NOAC plasma levels Pradaxa Atorvastatin P-gp/ CYP3A4 Digoxin P-gp Verapamil P-gp/ wk CYP3A4 Diltiazem P-gp/ wk CYP3A4 Quinidine Eliquis Savaysa Xarelto Dabigatran Apixaban Edoxaban Rivaroxaban +18% no data yet no effect no effect no effect no data yet no effect no effect +12–180% no data yet + 53% (slow release) minor effect no effect +40% No data minor effect P-gp +50% no data yet +80% +50% Amiodarone P-gp +12–60% no data yet no effect minor effect Dronedarone P-gp/CYP3A4 +70–100% no data yet +85% no data yet Ketoconazole; itraconazole; voriconazole; posaconazole; P-gp and BCRP/ CYP3A4 +140–150% +100% no data yet up to +160% Red – contraindicated; orange – reduce dose; yellow – consider dose reduction if another yellow factor present; hatching – no data available; recommendation made from pharmacokinetic considerations www.escardio.org/EHRA 19 Drug-drug interactions – NOAC plasma levels Interaction Fluconazole Cyclosporin; tacrolimus Clarithromycin; erythromycin Pradaxa Eliquis Savaysa Xarelto Dabigatran Apixaban Edoxaban Rivaroxaban CYP3A4 no data no data no data +42% P-gp no data no data no data +50% +15–20% no data no data +30–54% P-gp/ CYP3A4 HIV protease inhibitors P-gp and BCRP/ CYP3A4 no data strong increase no data up to +153% Rifampicin; St John’s wort; carbamezepine; phenytoin; phenobarbital P-gp and BCRP/ CYP3A4/CYP2J2 -66% -54% -35% up to -50% Antacids GI absorption -12-30% no data no effect no effect Red – contraindicated; orange – reduce dose; yellow – consider dose reduction if another yellow factor present; hatching – no data available; recommendation made from pharmacokinetic considerations www.escardio.org/EHRA 20 Factors associated with raised plasma levels of NOACs part 3 Pradaxa Eliquis Savaysa Xarelto Dabigatran Apixaban Edoxaban Aged ≥ 80 years Increased plasma level no data Aged ≥ 75 years Increased plasma level no data Weight ≤ 60 kg Increased plasma level Renal function Increased plasma level Rivaroxaban Pharmacodynamic interactions – antiplatelet drugs, NSAIDs Other increased bleeding risk Systemic steroid therapy Other anticoagulants Recent surgery on critical organ (brain, eye) Thrombocytopenia (e.g. chemotherapy) HAS-BLED ≥ 3 Orange – reduce dose; yellow – consider dose reduction if another yellow factor present; hatching – no data available; recommendation made from pharmacokinetic considerations www.escardio.org/EHRA 21 Switching between anticoagulant regimens VKA to NOAC Parenteral anticoagulant to NOAC: Intravenous unfractioned heparin (UFH) Low molecular weight heparin (LMWH) INR <2.0: immediate INR 2.0–2.5: immediate or next day INR >2.5: use INR and VKA half-life to estimate time to INR <2.5 Start once UFH discontinued (t½=2h). May be longer in patients with renal impairment Start when next dose would have been given NOAC to VKA Administer concomitantly until INR in appropriate range Measure INR just before next intake of NOAC Re-test 24h after last dose of NOAC Monitor INR in first month until stable values (2.0–3.0) achieved NOAC to parenteral anticoagulant Initiate when next dose of NOAC is due NOAC to NOAC Initiate when next dose is due except where higher plasma concentrations expected (e.g. renal impairment) Aspirin or clodiprogel to NOAC Switch immediately, unless combination therapy needed www.escardio.org/EHRA 22 How to deal with dosing errors Missed dose: BID: take missed dose up to 6 h after scheduled intake. If not possible skip dose and take next scheduled dose. QD: take missed dose up to 12 h after scheduled intake. If not possible skip dose and take next scheduled dose. Double dose: BID: skip next planned dose and restart BID after 24 h. QD: continue normal regimen. Uncertainty about intake: BID: continue normal regimen. QD: take another dose then continue normal regimen. Overdose: Hospitalization advised. www.escardio.org/EHRA 25 NOACs in renal dysfunction – dosing in chronic kidney disease Pradaxa Eliquis Savaysa Xarelto Dabigatran Apixaban Edoxaban Rivaroxaban When CrCl 30-49 ml/min, 150 CrCl 15-29 ml/min: 2.5 mg not available 15 mg OD when CrCl mg BID is possible (SmPC) but BID is possible 110 mg BID if ‘high risk of Serum creatinine ≥ 1.5 mg/dl bleeding’ (SmPC) or in combination with age ≥80 ‘recommended’ (GL update)1 years or weight ≤60 kg 15-49 ml/min (SmPC) or with other yellow’ Note: 75 mg BID approved in US factor: 2.5 mg BID only ** -if CrCl 15-30 ml/min - if CrCl 30-49 ml/min -and other orange factor (e.g. verapamil) **FDA recommendation based on pharmacokinetics. Carefully consider benefits and risks of this approach Note that 75 mg capsules are not available in Europe for AF indication. 1. Camm et al, Eur Heart J 2012;33:2719-47 www.escardio.org/EHRA 28 When to stop NOACs before a planned surgical intervention Last intake of drug before elective surgical intervention Pradaxa Dabigatran Eliquis Savaysa Apixaban Xarelto Edoxaban Rivaroxaban No important bleeding risk and/or local haemostasis possible: perform at trough level (i.e. ≥12h or 24h after last intake) Low risk High risk Low risk High risk CrCl ≥80 ml/min ≥24h ≥48h ≥24h ≥48h CrCl 50–80 ml/min ≥36h ≥72h ≥24h ≥48h CrCl 30–50 ml/min § ≥48h ≥96h ≥24h ≥48h CrCl 15–30 ml/min § not indicated not indicated ≥36h ≥48h CrCl <15 ml/min Low risk no data yet no data yet no data yet no data yet High risk Low risk High risk no data yet no data yet no data yet ≥24h ≥48h ≥24h ≥48h ≥24h ≥48h no data yet ≥36h ≥48h no official indication for use Low risk: surgery with low risk of bleeding. High risk: surgery with high risk of bleeding § many of these patients may be on the lower dose of dabigatran (i.e. 2x110 mg/d) or apixaban (i.e. 2x2.5 mg/d), or have to be on the lower dose of rivaroxaban (15 mg/d). www.escardio.org/EHR A 40 When to restart NOACs after a planned surgical intervention Procedures with immediate and complete Resume 6–8 h after surgery haemostasis: Atraumatic spinal/epidural anethesia Clean lumbar puncture Procedures associated with immobilization: Initiate reduced venous or intermediate dose of LMWH 6–8 h after surgery if haemostasis achieved. Procedures with post-operative risk of Restart NOACs 48–72h after surgery upon bleeding: complete haemostasis Thromboprophylaxis (e.g. with LMWH) can be initiated 6-8 h after surgery www.escardio.org/EHR A 41 Lariat Device WATCHMAN LAA Closure 3000838-20 Atrial Fibrillation- One heart beat away from a Stroke