Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
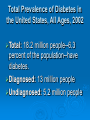
بسم هللا الرحمن الرحيم الحمد هلل رب العالمين والصالة والسالم على نبينا محمد خاتم األنبياء وسيد المرسلين وعلى آله وصحبه أجمعين وبعد Epidemiology of Chronic diseases Non communicable diseases Chronic diseases have been defined as : Chronic illnesses. Non-Communicable. Degenerative. Characteristics: Uncertain etiology. multiple risk factors. long latency period . Prolonged course of illness. non- contagious origin. functional disability and sometimes incurability . Latency period is the period between contact of the causative agent with susceptible host to the onset of first sign a symptoms. The cause of many chronic diseases remains obscure, but risk factors identified for some of the leading chronic diseases. The most important among these risk factor is Tobacco use especially in COPD . Strategies for the prevention Approach to prevention of chronic diseases can be considered under three headings : 1-Primordial prevention: prevention or avoiding the development of risk factors in the community to prevent the disease in the population and as such protects the individuals. This involves the avoidance of risk behaviors. prevention of disease occurrence by altering susceptibility of the host or reducing exposure of susceptible persons to the risk factors Examples : immunization , good nutrition , health education , counseling, environmental sanitation, purification of water , protection against accidents at work place and seat belts. Requires : accurate knowledge of causative agent and process of disease. 2-Primary prevention : Modifying or reducing the risk factors associated with the development of a disease in individuals with or without the use of interventions, It involves modification of established risk behavior and risk factors with specific interventions to prevent clinically manifest disease That is by early detection , screening by examinations altering the course of disease Examples : high blood pressure , T.B. Diabetes , Cancer of the breast , Cancer of the cervix colo-rectal cancers, lung cancer etc. 3- Secondary prevention : Modifying the risk factors in the presence of the manifested disease by changes in lifestyle and/or use of drugs. 4- Tertiary Prevention : alleviation and limitation of disability improvement of quality of life , Rehabilitation and follow up. What would be the top 10 causes of their deaths? 9 The major non communicable diseases are : Cardiovascular Diseases. Chronic Obstructive Pulmonary Disease Diabetes Hypertension Cancers • Accidents in its different types Non communicable diseases also include injuries, which have an acute onset, but may be followed by prolonged convalescence and impaired function, as well as chronic mental diseases. Out of all non-communicable illnesses, cardiovascular diseases stay as the leading cause of morbidity and mortality , especially in developed and rich countries. All over the world, almost 1.5 million adults and elderly died in 1995 from heart disease, stroke or other forms of circulatory disease. Cancer is a growing health problem in developing countries, where more than half of the global total of six million deaths occur. Noncommunicable diseases (NCDs) are a global challenge. During the next several decades, NCDs will govern the health care needs of populations in most low- and middle-income countries because of declines in communicable diseases, conditions related to childbirth and nutrition, changes in lifestyle factors (eg, smoking), and population aging (1). We examined the burden of NCDs in the Hashemite Kingdom of Jordan. We computed the projected prevalence of diabetes, hypertension, and high blood cholesterol. All of these risk factors are associated with an increased risk of cardiovascular disease (CVD) — the leading cause of death in Jordan — and increased health care use. In 2005, Jordan’s population was approximately 5.5 million. By 2050, the population is expected to increase to between 8.5 and 14.8 million people. (2) The proportion of older people (aged 60 years or older) is expected to be 15.6% (or approximately 1.8 million people) in 2050, more than 3 times that in 2000 (2). During 2005, NCDs accounted for more than 50% of all deaths in Jordan. Heart disease and stroke (International Statistical Classification of Diseases, 10th Revision, codes I00-I99) accounted for 35% of all deaths; malignant neoplasms (C00-C97) were responsible for 13% of deaths (3). Nearly 60% of deaths from malignant neoplasms occurred among people younger than 65 years, and approximately one-third of those who died from CVD were aged 65 or younger During 2004, approximately 400,000 (15%) Jordanian adults had diabetes (an increase from 7% in 1996), and an estimated 350,000 (12%) had impaired fasting glucose (4,5). Approximately 15% of adults reported hypertension, and roughly 23% had high blood cholesterol — an increase from 9% in 1996 (4,5). The proportion of all deaths attributable to NCDs in the World Health Organization's Eastern Mediterranean Region is projected to increase from 51% during 2005 to 66% by 2030 (6). Assuming prevalences are similar to that in Jordan, diabetes may affect nearly 10 million people in Egypt, one of the region’s largest countries, and 3 million people in Saudi Arabia. Hypertension may affect 18 million Egyptians and 6.5 million people in Saudi Arabia by 2050. Programs to monitor and control risk factors, clinical services, and a robust health care system will be important to successfully improve NCD outcomes and reduce the burden of disease. Reducing the prevalence of NCDs will require a renewed commitment by governmental and nongovernmental institutions, by public health professionals and clinical practitioners, and by communities and individuals to acknowledge the burden of NCDs and the need for timely action. Moreover, stimulating, strengthening, and sustaining regional efforts and programs are necessary to reduce the prevalence of NCDs through coordinated and integrated programs of health promotion and disease prevention. These programs should involve networks for risk factor surveillance, information sharing, capacity building, advocacy, policy development, and collaboration in generating, disseminating, and applying knowledge. Common CVD Risk Factors 1-Tobacco use. 2-Physical inactivity. 3- Unhealthy diet. Life expectancy in developing countries is rising sharply and people are exposed to these risk factors for longer periods. Newly merging CVD risk factors: Like low birth weight. folate deficiency. Infections. Social class: more frequent among the poorest in low and middle income countries. Hypertension Prevalence: Hypertension is estimated to cause 4.5% of current global disease burden and is as prevalent in many developing countries, as in the developed world. Blood pressure-induced cardiovascular risk rises continuously across the whole blood pressure range. Countries vary widely in capacity for management of hypertension, but worldwide the majority of diagnosed hypertensive are inadequately controlled. Hypertension affects one in four adults, putting them at higher risk for heart attacks, kidney disease, atherosclerosis, macular degeneration and stroke. It is often termed the "silent killer" because as many as 35% of those who have hypertension do not realize it. More than 60% of all women over age 65 have hypertension. Women over age 75 are much more likely to develop the disease than men.. HTN is a major public health problem of worldwide distribution and is the most common cardiovascular disease (CVD) risk factor . It is responsible for one half of coronary heart disease (CHD) and about two thirds of cerebrovascular accidents. By 2030, 23 million cardiovascular deaths are projected to have HTN, with about 85% occurring in low and middle-income countries . Research published between 1980 and 2002 indicate the prevalence of HTN in developing countries increased at a higher rate than in developed countries . Prevention of HTN is possible, and early detection and treatment can reduce the incidence of complications including stroke, CHD, heart failure, and kidney disease , and yet the levels of control of hypertension are low worldwide. Economically developed countries have higher rates of HTN than in developing countries . However, data reported in the last decade indicate that the prevalence, awareness, treatment, and control of hypertension in economically developing countries are coming closer to those in economically developed countries . Recent epidemiological studies on prevalence, awareness, treatment, and control of HTN in Jordan are scarce. The few community-based studies conducted between 1994 and 1996 in Jordan demonstrated a 16.1 and 16.3% prevalence rates of HTN (cut-off point 160/90 mm Hg) with concomitant low levels of awareness, treatment, and control. Since that time, several activities have been implemented to face this challenge in HTN which have not been evaluated. Moreover, the last decades showed a remarkable improvement in treatment of hypertension due to introduction of new antihypertensive medications and the development of international guidelines for detection and management . Meyasser Zindah, head of the Health Ministry's cardiovascular disease department, warned of the high prevalence of heart disease, noting that 662,527 citizens over the age of 18 suffered from high blood pressure in 2007. Risk Factors Uncontrollable risk factors: Increasing age. Family history. Race, African-Americans are at higher risk than Caucasians). Sodium sensitivity. . Controllable risk factors: Overweight or obesity. Physical inactivity. Heavy alcohol consumption. Use of oral contraceptives. Excessive sodium intake. . Diet: Dairy, Fruits & Vegetables, and low fat, high Fibers food may Lower Blood Pressure a recent study suggests that adding certain foods to the diet may also help. The dairy products act in lowering blood pressure in mildly hypertensive adults. Fat: Fatty food increases the risk. Coronary heart disease ( CHD) is the leading cause of death in Industrialized countries CHD is also called Ischemic heart disease or coronary artery disease . These are several disorders that reduce the blood supply to the heart muscle . The underlying impairment is the atherosclerosis which remains sub clinical . Heart Disease Leading Cause of Death in Jordan 2008 Heart disease has become a leading threat to the health of the Jordanian population, with 40.5 percent of deaths last year found to be related with heart ailments . High risk groups: Gender: Men have a higher CHD mortality rates than women twice for men than women , never the less, CHD is the single greatest mortality risk in women : 3 times the risk of breast cancer. Age : CHD is the leading cause of death for men and women over 65 years of age. For men- major increases in CHD begin in 35-44 year age group. For women – marked increase is delayed until after menopause Sub- clinical CHD is more prevalent in older than younger persons. Black women die at a higher rate than white women from CHD The Asians in American have approximately half( ½) the CHD mortality than white Americans. Risk factors: Coronary risk factors are modifiable and nonmodifiable . Modifiable : Most important factors are : high blood cholesterol elevated blood cholesterol physical inactivity smoking Other modifiable include : diabetes obesity dietary factors alcohol use stress Non- modifiable risk factors are : Ethnicity. age. gender. socioeconomic status Classification of risk factors by magnitude of the risk moderate relative risk : high B.P 140/90 : cigarette smoking : elevated cholesterol ( 200mg) : diabetes FBS 140 mg Weak relative risk obesity physical inactivity environmental tobacco smoke exposure Possible relative risk : Excessive alcohol use Elevated plasma homocysteine Infectious agents Selected Risk factors: Cigarette smoking is a major cause of CHD among men and women Smokers have twice the risk of heart attack than non-smokers. Risk of sudden death from heart attack 24 times higher than the risk of nonsmokers Heavy smokers , CHD death is 23 times than non-smokers Stop smoking : rapid reduction of CHD mortality it takes 10 years to become normal. Passive smoking – increased risk of CHD than non-exposed. Arteriography of non-smoking exposed women with CHD showed number of stenotic arteries correlated with exposure. Importance of this health problem. Cholesterol : CHD increases steadily with increase of cholesterol blood level. < 200 mg : low risk of CHD 240 mg : risk doubles. Excess CHD occurs with levels 220-310 mg for people with cholesterol levels 250300 mg range. Each 1% reduction in cholesterol level results in about a 2% reduction in CHD morbidity and mortality . High levels of LDL are leading factor in progression of atherosclorosis and development of CHD. Evidence supporting the association of elevated blood triglycerides and CHD has been mounting in recent years. The level of HDL is inversely related to CHD however the lower level of HDL < 35mg increases the risk of CHD. Diabetes is considered a major CHD risk factor CHD is the most common cause of morbidity and mortality among diabetics – 2-4 times higher than non-diabetics. Risk is higher in diabetic women than diabetic men. Homocysteine , increased attention as a potential modifiable risk factor for acute CHD. Plasma levels of homocysteine , positively associated with risk of CHD. Homocysteine : an inborn metabolic error leads to extremely high levels of homocysteine people with this error, have strokes before age 30 years . People with moderately high homocysteine levels have not been shown to be at increased risk of CHD. Obesity : . Body mass index (kg/m2) BMI ( weight) ratio of weight to height > (height ) 2 Overweight : BMI > 27.8 kg/m2 in males : BMI > 27.3 kg /m2 in females prevalence of overweight increased dramatically in the USA Poverty is related to obesity in women Death from CHD is associated with obesity at the upper range of body weight BMI 30 kg/m2 . Under the age of 50 years, men and women with relative weight of 130% or more – associated with two fold increase in risk of CHD. Recent studies suggest that the distribution of fat is the body may effect CHD risk Central obesity – upper body and abdominal fat increases risk more than lower body fat. Physical Activity 6) Physical in-activity is recognized as a major risk factor for CHD. Physical activity decreases body weight blood pressure and improves insulin sensitivity . The greatest benefits appear to occur with very moderate level of activity. 7) Alcohol consumption: Moderate to heavy increases blood pressure levels and CHD mortality , however , light regular drinking has been associated with modest reduction of CHD risk through increasing HDL. 8) Psychological factors and stress : especially type A behavior pattern characterized by excessive competitiveness, hostility , impatience, fast speech and quick motor movements have been studied along with anger, job stress, anxiety and social support. 9) Risk factors for CHD tend to work in cluster than individual the patient likely to have more than one risk factor. CHD increases markedly when risk factors manifest simultaneously there is an additive contribution to CHD risk factors . "This number is much higher than 10 years ago," The prevalence of cardiovascular disease in Jordan is mostly due to diet, smoking and pollution, according to Bassam Hijjawi, director of the ministry's disease control department. He also tied the prevalence of the chronic disease to a lack of exercise, noting that over 60 percent of Jordanians suffering from heart conditions do not participate in physical exercises. In Jordan, the average life expectancy in 2002 was 72 years, and chronic diseases are becoming increasingly prevalent. Because personal behavior can influence the occurrence and progression of many chronic diseases. the Jordan Ministry of Health (JMOH) established surveillance for behavioral risk factors, particularly those related to cardiovascular diseases and diabetes. This report summarizes the key findings of the 2002 Behavioral Risk Factor Survey, the first reporting segment in Jordan's surveillance program for chronic diseases. The findings indicate that: A- Smoking B- Physical inactivity C- Obesity contribute substantially to the burden of chronic disease in Jordan and underscores the need for effective public health interventions. Reported by: F Shehab, MD, Field Epidemiology Training Program; A Belbeisi, MD, Jordan Ministry of Health. H Walke, MD, Div of International Health, Epidemiology Program Office, CDC. بسم هللا الرحمن الرحيم الحمد هلل رب العالمين والصالة والسالم على نبينا محمد خاتم األنبياء وسيد المرسلين وعلى آله وصحبه أجمعين وبعد What is diabetes? Diabetes mellitus is a group of diseases characterized by high levels of blood glucose resulting from defects in insulin production, insulin action, or both. Diabetes can be associated with serious complications and premature death, but people with diabetes can take steps to control the disease and lower the risk of complications. Types of diabetes Type 1 diabetes was previously called insulin-dependent diabetes mellitus (IDDM) or juvenile-onset diabetes.(510%). Type 2 diabetes was previously called non-insulin-dependent diabetes mellitus (NIDDM) or adult-onset diabetes. Type 2 diabetes may account for about 90 percent to 95 percent of all diagnosed cases. Gestational diabetes: After pregnancy, 5 percent to 10 percent of women with gestational diabetes are found to have type 2 diabetes. Women who have had gestational diabetes have a 20 percent to 50 percent chance of developing diabetes in the next 5-10 years. Other specific types of diabetes result from specific genetic conditions (such as maturity-onset diabetes of youth), surgery, drugs, malnutrition, infections, and other illnesses. Such types of diabetes may account for 1 percent to 5 percent of all diagnosed cases of diabetes. Risk Factors The primary risk factor for type 1 diabetes Genetics and family history. Having family members with diabetes is a major risk factor. The American Diabetes Association recommends that anyone with a first-degree relative with type 1 diabetes -- a mother, father, sister, or brother -- should get screened for diabetes. A simple blood test can diagnose type 1 diabetes. Diseases of the pancreas. Injury or diseases of the pancreas can inhibit its ability to produce insulin and lead to type 1 diabetes. Infection or illness. A range of relatively rare infections and illnesses can damage the pancreas and cause type 1 diabetes. Risk Factors for Type 2 Diabetes . Type 2 diabetes occurs when the body can't use the insulin that's produced, a condition called insulin resistance. Though it typically starts in adulthood, type 2 diabetes can begin anytime in life. Because of the current epidemic of obesity among U.S. children, type 2 diabetes is increasingly found in teenagers. Obesity or being overweight is a major risk factor for Diabetes Type 2. Diabetes has long been linked to obesity and being overweight. Research at the Harvard School of Public Health showed that the single best predictor of type 2 diabetes is being obese or overweight Obesity and diabetes are both epidemic in the U.S. The most-used measure for obesity is BMI, which stands for body mass index. BMI is a ratio, and can be determined using standard tables of height and weight (kg/m2) . A BMI of 25 to 29.9 is considered overweight. A BMI of 30 or higher defines obesity. BMI of 40 would be diagnosed with "extreme obesity" or as having “clinically severe morbid obesity”. The CDC ( Centers for Disease Control and Prevention )estimates that more than one out of every four Americans is obese, having a BMI of 30 to 39.9; 6% of Americans have clinically severe obesity. That means they have a BMI of 40 or greater. Impaired glucose tolerance or impaired fasting glucose. Prediabetes is a milder form of diabetes that's sometimes called impaired glucose tolerance. It can be diagnosed with a simple blood test. Prediabetes is a major risk factor for developing type 2 diabetes. Insulin resistance. Type 2 diabetes often starts with cells that are resistant to insulin. That means they are unable to take in insulin as it moves glucose from the blood into cells. With insulin resistance, the pancreas has to work overly hard to produce enough insulin so cells can get the energy they need. This involves a complex process that eventually leads to type 2 diabetes. Ethnic background. Diabetes occurs more often in Hispanic/Latino Americans, African-Americans, Native Americans, Asian-Americans, Pacific Islanders, and Alaska natives. High blood pressure . Hypertension, or high blood pressure, is a major risk factor for diabetes. High blood pressure is generally defined as 140/90 mm Hg or higher. Low levels of HDL "good" cholesterol and high triglyceride levels also put you at risk. History of gestational diabetes. If you developed diabetes while you were pregnant, you've had what is called gestational diabetes. Having had gestational diabetes puts you at higher risk of developing type 2 diabetes later in life. Sedentary lifestyle. Being inactive -exercising fewer than three times a week -- makes you more likely to develop diabetes. Family history. Having a family history of diabetes -- a parent or sibling who's been diagnosed with this condition -increases your risk of developing type 2 diabetes. Polycystic ovary syndrome. Women with polycystic ovary syndrome (PCOS) are at higher risk of type 2 diabetes. Age. Some doctors advise anyone over 45 to be screened for diabetes. That's because increasing age puts you at higher risk of developing type 2 diabetes. It's important to remember, though, that people at any age can develop diabetes. If you're over 45 and overweight or if you have symptoms of diabetes, talk to your doctor about a simple screening test. Gestational Diabetes Risk Factors Obesity or being overweight. Being obese or overweight puts women at risk of gestational diabetes. Polycystic ovary syndrome Previous glucose intolerance. A history of glucose intolerance or previous gestational diabetes increases the risk of gestational diabetes in a current pregnancy. Family history. A family history of diabetes -- a parent or sibling who's been diagnosed with diabetes -increases the risk of gestational diabetes. Age. The older a woman is when she becomes pregnant, the higher her risk of gestational diabetes. Prevention Whatever your risk factors for diabetes may be, there's a lot you can do to delay or prevent diabetes. To manage your risk of diabetes, you should: manage your blood pressure keep your weight within or near normal ranges get moderate exercise on most days eat a balanced diet Prevention Lifestyle interventions included diet and moderate-intensity physical activity (such as walking for 2 1/2 hours each week). In the Diabetes Prevention Program, a large prevention study of people at high risk for diabetes, the development of diabetes was reduced 58 percent over 3 years. Prevention or Delay of Diabetes Research studies have found that lifestyle changes can prevent or delay the onset of type 2 diabetes among high-risk adults. These studies included people with IGT and other high-risk characteristics for developing diabetes. Prevention of Diabetes Complications Diabetes can affect many parts of the body and can lead to serious complications such as blindness, kidney damage, and lower-limb amputations. Working together, people with diabetes and their health care providers can reduce the occurrence of these and other diabetes complications by controlling the levels of blood glucose, blood pressure, and blood lipids and by receiving other preventive care practices in a timely manner. Total Prevalence of Diabetes in the United States, All Ages, 2002 Total: 18.2 million people--6.3 percent of the population--have diabetes. Diagnosed: 13 million people Undiagnosed: 5.2 million people Diabetes in Jordan An increase in prevalence of diabetes mellitus in Jordan over 10 years. The age-standardized prevalence of diabetes and impaired fasting glycemia IFG was 17.1% and 7.8%, respectively, with no significant differences between women and men. Journal Diabetes Complications. 2008 SepOct;22(5):317-24. Epub 2008 Apr 16. Ajlouni K, Khader YS, Batieha A, Ajlouni H, ElKhateeb M. The prevalence of type 2 diabetes and impaired fasting glycemia (IFG) is high in Jordan and is increasing. More than half of the patients with diabetes have unsatisfactory control. Therefore, they are likely to benefit from programs aimed at encouraging behaviors toward achieving optimum weight as well as physical activity behaviors. Physicians caring for patients with diabetes may need to adopt a more vigorous approach for diabetes control. CONCLUSION: Diabetes mellitus and IGT are common among adult Jordanians. Considering the high prevalence of this sickness makes it imperative to formulate a national plan to face this disease and its complications. Global Prevalence of Diabetes Estimates for the year 2000 and projections for 2030 Sarah Wild, MB BCHIR, PHD1, Gojka Roglic, MD2, Anders Green, MD, PHD, DR MED SCI3, Richard Sicree, MBBS, MPH4 and Hilary King, MD, DSC2 RESULTS The prevalence of diabetes for all agegroups worldwide was estimated to be 2.8% in 2000 and 4.4% in 2030. The total number of people with diabetes is projected to rise from 171 million in 2000 to 366 million in 2030. The prevalence of diabetes is higher in men than women, but there are more women with diabetes than men. The urban population in developing countries is projected to double between 2000 and 2030. The most important demographic change to diabetes prevalence across the world appears to be the increase in the proportion of people >65 years of age. CONCLUSIONS These findings indicate that the “diabetes epidemic” will continue even if levels of obesity remain constant. Given the increasing prevalence of obesity, it is likely that these figures provide an underestimate of future diabetes prevalence. Deaths Among People with Diabetes, United States, 2000 Diabetes was the sixth leading cause of death listed on U.S. death certificates in 2000. This ranking is based on the 69,301 death certificates in which diabetes was listed as the underlying cause of death. Diabetes is likely to be underreported as a cause of death. Risk for death Studies have found that only about 35 percent to 40 percent of decedents with diabetes have diabetes listed anywhere on the death certificate and only about 10 percent to 15 percent have it listed as the underlying cause of death. Overall, the risk for death among people with diabetes is about two times that of people without diabetes. Complications of Diabetes Heart disease and stroke Heart disease is the leading cause of diabetesrelated deaths. Adults with diabetes have heart disease death rates about two to four times higher than adults without diabetes. The risk for stroke is two to four times higher among people with diabetes. About 65 percent of deaths among people with diabetes are due to heart disease and stroke. High blood pressure About 73 percent of adults with diabetes have blood pressure greater than or equal to 130/80 mm Hg or use prescription medications for hypertension. Blindness Diabetes is the leading cause of new cases of blindness among adults aged 20-74 years. Diabetic retinopathy causes 12,000 to 24,000 new cases of blindness each year. Kidney disease Diabetes is the leading cause of end-stage renal disease, accounting for 44 percent of new cases. In 2001, 42,813 people with diabetes began treatment for end-stage renal disease. In 2001, a total of 142,963 people with end-stage renal disease due to diabetes were living on chronic dialysis or with a kidney transplant. Nervous system disease About 60 percent to 70 percent of people with diabetes have mild to severe forms of nervous system damage. The results of such damage include impaired sensation or pain in the feet or hands, slowed digestion of food in the stomach, carpal tunnel syndrome, and other nerve problems. Amputations More than 60 percent of nontraumatic lower-limb amputations occur among people with diabetes. In 2000-2001, about 82,000 nontraumatic lower-limb amputations were performed annually among people with diabetes. Dental disease Periodontal (gum) disease is more common among people with diabetes. Among young adults, those with diabetes have about twice the risk of those without diabetes. Almost one-third of people with diabetes have severe periodontal diseases with loss of attachment of the gums to the teeth measuring 5 millimeters or more. Complications of pregnancy Poorly controlled diabetes before conception and during the first trimester of pregnancy can cause major birth defects in 5 percent to 10 percent of pregnancies and spontaneous abortions in 15 percent to 20 percent of pregnancies. Poorly controlled diabetes during the second and third trimesters of pregnancy can result in excessively large babies, posing a risk to the mother and the child. Other complications Uncontrolled diabetes often leads to biochemical imbalances that can cause acute life-threatening events, such as diabetic ketoacidosis and hyperosmolar (nonketotic) coma. People with diabetes are more susceptible to many other illnesses and, once they acquire these illnesses, often have worse prognoses. For example, they are more likely to die with pneumonia or influenza than people who do not have diabetes. Cost of diabetes in the United States, 2002 Total (direct and indirect): $132 billion Prevalence of diabetes in Arab World Diabetes Risk Factors Diabetes complications Diabetes Complications References 1-Mathers CD, Loncar D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med 2005;3(11):e442. 2-Population Division of the Department of Economic and Social Affairs of the United Nations Secretariat. World population prospects: The 2006 revision. New York (NY): United Nations; 2007. 3-Directorate of Information Studies and Research, Ministry of Health, The Hashemite Kingdom of Jordan. Mortality in Jordan 2005. Amman (JO): Ministry of Health, The Hashemite Kingdom of Jordan; 2008. 4-Mokdad AH. Health issues in the Arab American community. Chronic diseases and the potential for prevention in the Arab world: the Jordanian experience. Ethn Dis 2007;17(2 Suppl 3):S3-55-56. 5-Zindah M, Belbeisi A, Walke H, Mokdad AH. Obesity and diabetes in Jordan: findings from the Behavioral Risk Factor Surveillance System, 2004. Prev Chronic Dis 2008;5(1). http://www.cdc.gov/pcd/issues/2008/jan/06_0172.htm. 6-Projections of mortality and burden of disease to 2030. Geneva (CH): http://www.who.int/healthinfo/statistics/bodprojections2030/ en/index.html. Accessed July 16, 2008. بسم هللا الرحمن الرحيم الحمد هلل رب العالمين والصالة والسالم على نبينا محمد خاتم األنبياء وسيد المرسلين وعلى آله وصحبه أجمعين وبعد Chronic Diseases 2 Disability or chronicity may be the outcome of many of these chronic diseases and they will not be accounted for by using the mortality indicators as the only indicators for these chronic and degenerative diseases is the resulting morbidities and disabilities rates. Examples : 1- Musculo-sketelal problems Osteoporosis Artihritis and osteoarthritis which may reach in old age a prevalence of 600/1000 persons, and over 300/1000 persons in males. Rheumatoid arthritis Low back pain Foot problems in old age Scoliosis in children Congenital hip dislocation 2- Neurological disorders Cerebral palsy Mental retardation Epilepsy and o ther seizure disorders Headache and migraine Multiple sclerosis Alzheimer and dementia Parkinson disease. Psychiatric Disorders Psychosis Schizophrenia 6--Affective psychosis 4--Unspecified psychosis 3--Senile & pre-senile dementia 3--Psychosis associated with other cerebral conditions1 Neuroses. Phobias Anxiety Depression Obsessive Compulsive Neuroses. Personality disorders & other nonpsychotic mental disorders Depression Depression, a mental illness in which a person experiences deep, unshakable sadness and diminished interest in nearly all activities. People also use the term depression to describe the temporary sadness, loneliness, or blues that everyone feels from time to time. In contrast to normal sadness, severe depression, also called major depression, can dramatically impair a person's ability to function in social situations and at work. People with major depression often have feelings of despair, hopelessness, and worthlessness, as well as thoughts of committing suicide Surveys indicate that people commonly view depression as a sign of personal weakness, but psychiatrists and psychologists view it as a real illness. In the United States, the National Institute of Mental Health has estimated that depression costs society many billions of dollars each year, mostly in lost work time. Why is depression important? Projections are that by 2020, depression will be second only to heart disease in its contribution to the global burden of disease as measured disability-adjusted life years PREVALENCE Depression is one of the most common mental illnesses. At least 8 percent of adults in the United States experience serious depression at some point during their lives, and estimates range as high as 17 percent. Epidemiology of Depression Among Women In U.S. twice as many women (12.3%) as men (6.7%) are affected each year 12.4M women and 6.4M men For low-income women, the estimated prevalence doubles to 25% Most prevalent among women of childbearing and child-rearing age (16 to 53) Epidemiology of Depression Among Mothers Estimated rates of depression among pregnant and postpartum women range from 8 to 20%. For low-income women with young children, prevalence rates are commonly estimated at approximately 40%. PREVALENCE Primary Health Care Physicians are the diagnosticians at the front line of the health services, and untreated depression has come to be viewed as a major public health problem. In Arab world Communities in Arab world show depression ranging from 13% to 32%. Highest rate 32% was recorded in Lebanese women after the civil war. Urban population in Dubai and Cairo showed lower rates 12% and 16% respectively. The illness affects all people, regardless of sex, race, ethnicity, or socioeconomic standing. However, women are two to three times more likely than men to suffer from depression. Experts disagree on the reason for this difference. Some cite differences in hormones, and others point to the stress caused by society's expectations of women. Prevalence Depression occurs in all parts of the world, although the pattern of symptoms can vary. The prevalence of depression in other countries varies widely, from 1.5 percent of people in Taiwan to 19 percent of people in Lebanon. Some researchers believe methods of gathering data on depression account for different rates. A number of large-scale studies indicate that depression rates have increased worldwide over the past several decades. Furthermore, younger generations are experiencing depression at an earlier age than did previous generations.. Social scientists have proposed many explanations, including changes in family structure, urbanization, and reduced cultural and religious influences Prevalence of Depression In Jordan • A study published last year, done on Jordanian women reviewing PHC centers for different reasons showed a rate of 37% scored positively. Onset Although it may appear anytime from childhood to old age, depression usually begins during a person's 20s or 30s. The illness may come on slowly, then deepen gradually over months or years. Symptoms. A) Appetite and Sleep Changes B) Changes in Energy Level C) Poor Self-Esteem CAUSES/Risk Factors Some depressions seem to come out of the blue, even when things are going well. Others seem to have an obvious cause: a marital conflict, financial difficulty, or some personal failure. Yet many people with these problems do not become deeply depressed. Most psychologists believe depression results from an interaction between stressful life events and a person's biological and psychological vulnerabilities. A) Biological/Genetic Factors . Depression runs in families. By studying twins, researchers have found evidence of a strong genetic influence in depression. Genetically identical twins raised in the same environment are three times more likely to have depression in common than fraternal twins, who have only about half of their genes in common. In addition, identical twins are five times more likely to have bipolar disorder in common. These findings suggest that vulnerability to depression and bipolar disorder can be inherited. Adoption studies have provided more evidence of a genetic role in depression. These studies show that children of depressed people are vulnerable to depression even when raised by adoptive parents. Genetic/Biochemical Factors Genes may influence depression by causing abnormal activity in the brain. Studies have shown that certain brain chemicals called neurotransmitters play an important role in regulating moods and emotions. Neurotransmitters involved in depression include norepinephrine, dopamine, and serotonin. Research in the 1960s suggested that depression results from lower than normal levels of these neurotransmitters in parts of the brain. Support for this theory came from the effects of antidepressant drugs, which work by increasing the levels of neurotransmitters involved in depression. However, later studies have discredited this simple explanation and have suggested a more complex relationship between neurotransmitter levels and depression. An imbalance of hormones may also play a role in depression. Many depressed people have higher than normal levels of hydrocortisone (cortisol), a hormone secreted by the adrenal gland in response to stress. In addition, an under active or overactive thyroid gland can lead to depression. Medical causes A variety of medical conditions can cause depression. These include dietary deficiencies in vitamin B6, vitamin B12, and folic acid (see Vitamin); degenerative neurological disorders, such as Alzheimer's disease and Parkinson's disease ; strokes in the frontal part of the brain; and certain viral infections, such as hepatitis and mononucleosis. Many chronic diseases: Cardiovascular Diabetes Epilepsy Multiple Scleroses Rheumatoid Arthritis and others B) Psychological Factors As a secondary to psychiatric illness especially Neurotic (Obsessive Compulsive Neurosis), or Affective Schizophrenia. C) Stressful Events/Environmental Psychologists agree that stressful experiences can trigger depression in people who are predisposed to the illness. For example, the death of a loved one may trigger depression. Psychologists usually distinguish true depression from grief, a normal process of mourning a loved one who has died (Reactive Depression). Gender In the United States, women are about as twice as likely as men to be diagnosed and treated for major depression. Approximately 20-25% of women and 12% of men will experience a serious depression at least once in their lifetimes. Among children, depression appears to occur in equal numbers of girls and boys. However, as girls reach adolescence, they tend to become more depressed than boys do. This gender difference continues into older age. Other stressful experiences may include divorce, pregnancy, the loss of a job, and even childbirth. About 20% of women experience an episode of depression, known as postpartum depression, after having a baby. In addition, people with serious physical illnesses or disabilities often develop depression TREATMENT Depression typically cannot be shaken or willed away. An episode must therefore run its course until it weakens either on its own or with treatment. Depression can be treated effectively with antidepressant drugs, psychotherapy, or a combination of both. Other Treatments Electroconvulsive therapy (ECT) can often relieve severe depression in people who fail to respond to antidepressant medication and psychotherapy. Regular aerobic exercise may improve mood as effectively as psychotherapy or medication. In addition, some research indicates that dietary modifications can influence one's mood by changing the level of serotonin in the brain. Despite the availability of effective treatment, most depressive disorders go untreated and undiagnosed. Studies indicate that general physicians fail to recognize depression in their patients at least half of the time. In addition, many doctors and patients view depression in elderly people as a normal part of aging, even though treatment for depression in older people is usually very effective. Conclusion Of the estimated 17.5 million Americans who are affected by some form of depression, 9.2 million have major or clinical depression Two thirds of people suffering from depression do not seek necessary treatment. 80% Of all people with clinical depression who have received treatment significantly improve their lives. The economic cost of depression is estimated at $30.4 billion a year but the cost in human suffering cannot be estimated Women experience depression about twice as often as men By the year 2020, the World Health Organization (WHO) estimates that depression will be the number two cause of "lost years of healthy life" worldwide According to the U.S. Centers for Disease Control and Prevention (CDC) suicide was the ninth leading cause of death in the United States in 1996 Recommendations Public education. Provision of relevant posters and leaflets in waiting rooms at PHC centers helps in destigmatization of the disease. Improvements in depression screening have paralleled improvements in depression treatment and reduced stigma Encourage patients to talk about their symptoms with their Family doctors. Recognition of depression by the patient and his or her family. PCPs have embraced responsibility for screening ,recognition, and treating depression For additional efficiencies, we will need Advances in technology (e.g,computerized screening and scoring) Improved Rx outcomes Training courses for Primary Health physicians to improve their diagnostic skills in depression to improve the recognition rate of depression in Primary Health Care Settings in Jordan is also recommended Dementia Dementia is defined as global impairment of cognitive function which interferes with normal activities. Impaired short and long-term memory and other cognitive functions (abstract thinking, judgment, speech, coordination, planning or organization Alzheimer's accounts for most cases of dementia. 10-20% cases are attributed to vascular (multi-infarct) dementia Other causes-alcoholism, Parkinson, vit B12 deficiency, hypothyroidism, CNS infections, intracranial lesions Prevalence of Dementia Increases steadily with age, roughly doubling every 5 years Common among institutionalized elderly Present in ½ to 2/3 of nursing home residents Family history associated with an increased risk of Alzheimer Prevalence of Dementia disease progresses over a period of 2-20 years, causing increasing functional impairment and disability Care of the demented patient imposes an enormous psychosocial and economical factors. • Alzheimer’s burden on the family Risk factors Age: Strongest risk factor particularly for ALZ d annual incidence 0.6% for age 65-69 1% for age 70-74 2% for age 75-79 3.3 % for age 80-84 and 8.4% for above 85 1/2-2/3 of nursing home residents Risk factors Family history : Especially in relation to ALZ D First degree relatives have 10-30% increased risk for the disease Apolipoprotein E epsilon 4 genotype predisposes to development of ALZD Risk factors History of head trauma especially with the epsilon 4 allele History of low educational achievement Organic solvent exposure Female gender 16%/6% Relationship to blood pressure : a U shape association Hypercholesterolemia /role of statins Diabetes Screening Tests Dementia is easily recognized in advanced stages, often overlooked in early stage Clinicians fail to detect 21-72% of patients with dementia esp. in early stages Routing physical examination and patient history not sensitive for dementia, especially if family members not present to corroborate patient self-report Alzheimer Warning Signs Top Ten Alzheimer Association 1. Recent memory loss affecting job 2. Difficulty performing familiar tasks 3. Problems with language 4. Disorientation to time or place 5. Poor or decreased judgment 6. Problems with abstract thinking 7. Misplacing things 8. Changes in mood or behavior 9. Changes in personality 10. Loss of initiative AD is Under-diagnosed Early Alzheimer’s disease is subtle, the diagnosis continues to be missed it is easy for family members to avoid the problem and compensate for the patient physicians tend to miss the initial signs and symptoms Less than half of AD patients are diagnosed Estimates are that 25% to 50% of cases remain undiagnosed Diagnoses are missed at all levels of severity: mild, moderate, severe Evans DA. Milbank Quarterly. 1990; 68:267-289 Undiagnosed AD patients often face avoidable social, financial, and medical problems Early diagnosis and appropriate intervention may lessen disease burden Early treatment may improve overall course substantially No definitive laboratory test for diagnosing AD exists Efforts to develop biomarkers, early recognition by brain scan Prevalence of Alzheimer Alzheimer’s disease (AD) is the most common form of dementia. It represents a worldwide medical challenge affecting more than 18 million people; estimated to reach 34 million by the year 2025 . PREVALENCE of AD Estimated 4 million cases in US (2000) • (2000 - 46 million individuals over 60 y/o) Estimated 500,000 new cases per year Increase 1% 2% 4% 8% with age of 60 - 65 of 65 - 70 of 70 - 75 of 75 - 80 • 16% of (prevalence) (10.7m) ( 9.4m) ( 8.7m) ( 7.4m) 80 - 85 ( = 107,000 = 188,000 = 350,000 = 595,000 5.0m) = 800,000 With over 1.5 million cases in the Arab world. Alzheimer’s disease is a devastating illness which can affect all members of society Conclusions and Recommendations Next to Cancer and AIDS, the highest medical budgets are allocated to Alzheimer’s research. The Arab Conference on AD 2005 seeks to develop a regional and national plan to raise the level of awareness on AD and reach patients, caregivers, specialists, doctors, nurses, specialized international agencies and governmental and non-governmental organizations Multiple Sclerosis Epidemiology and Prevalence Onset Geographic Distribution Population Studies Genetic Factors Who Has MS In the United States, about 400,000 people have the disease, which is twice as common in women as men. Approximately 2.5 million people may have MS worldwide. Most people with MS are diagnosed between the ages of 20 and 40. Onset Geographic Distribution Population Studies Genetic Factors Onset There are about 300,000 patients suffering from Multiple Sclerosis in the North America today. The age of onset peaks between 20 and 30 years. Almost 70% of patients manifest symptoms between ages 21 and 40. Disease rarely occurs prior to 10 or after 60 years of age. However, patients as young as 3 and as old as 67 years of age have been described. Like other immuno- mediated diseases, females are affected more frequently than males (1.4 to 3.1 times as many women than men affected.) Geographic Distribution There is a very specific geographic distribution of this disease around the world. A significantly higher incidence of the disease is found in the northernmost latitudes of the northern and the southern hemispheres compared to southernmost latitudes. This observation is based on the incidence of the disease in Scandinavia, northern United States and Canada, as well as Australia and New Zealand. The data from migration studies shows that if the exposure to a higher risk environment occurs during adolescence (before 15 years of age,) the migrant assumes the higher risk of the environment.. What Is MS? Multiple sclerosis (MS) is a disease that attacks the central nervous system—the brain and the spinal cord. Depending on which nerves are damaged, people with MS may experience problems with balance, muscle coordination, vision, speech, thinking, or other physical and mental abilities. Population Studies There are also population studies that show difference in susceptibility to MS between different populations. Lapps in Scandinavia appear to be resistant to the disease, contrary to the expectations based on their geographic distribution. Native Americans and Hutterites very infrequently suffer from MS, as opposed to other residents of the North America. MS is uncommon in Japan, China and South America. It is practically unknown among the indigenous people of equatorial Africa and among native Inuit in Alaska. When the racial differences are correlated, White populations are at greater risk than Asian or African populations. We can not yet explain these obvious inconsistencies in disease distribution, but the knowledge of them may be helpful in assessing specific patients. Prevalence of MS Prevalence data imply that racial and ethnic differences are important in influencing the worldwide distribution of MS and that its geography must be interpreted in terms of the probable discontinuous distribution of genetic susceptibility alleles. Racially and ethnically influenced differences in the risk of MS, however, can be modified by environment. Genetic Factors The incidence of MS in first degree relatives is 20 times higher than in general population, suggesting the influence of genetic factors on the disease. Monozygotic twin studies show the concordance rate of 30%. Dizygotic twins show concordance rate of less than 5%. These results suggest that both the genetic factors and environmental exposure are important in disease expression. Symptoms Symptoms associated with MS vary widely. There is not yet a way to predict what symptoms people with MS may experience. MS symptoms are divided into three types: . Primary symptoms are those caused directly by the disease process including immune system activity, destruction of myelin or the ensuing nerve damage. The most common include problems with walking or maintaining balance, visual impairment (optic neuritis), lapses in memory, inability to solve problems or pay attention for long periods of time, pain, sexual dysfunction, dizziness, depression or mood swings, and disturbances in bladder or bowel function. Less common symptoms include speech and swallowing disorders, tremors and seizures Secondary symptoms are complications that occur as a result of primary symptoms. For instance, a person with MS may have urinary burning, which could be a sign of a urinary tract infection, resulting from lack of bladder control caused by nerve damage. Tertiary symptoms may include lowered self-esteem, which could affect a person's family or social life. Multiple sclerosis in Arabs in Jordan . Department of Biochemistry and Microbiology, Faculty of Medicine, Jordan University, Amman. In a 2-year hospital-based study (1992 and 1993), there were 131 multiple sclerosis patients attending 2 large referral hospitals in Jordan. There were 126 Arabs of whom 84 were Palestinians and 36 indigenous Jordanians. Comparison of these subgroups, which had a similar age distribution revealed that the disease was twice as frequent in Palestinians (estimated 42.0/100,000) among Jordanians (estimated 20.0/100,000). Clinical presentation, pattern of disease, disability associated with the disease were similar to that in the disease reported in Caucasians in the West. All investigations including neurophysiology and imaging were also very similar to Western reports 6- Genetic disorders – Down’s syndrome Autosomal recessive defect chromosome 7 mutations are thought to be responsible for that disease . Cystic fibrosis : is the most lethal in Northern European descent (1/3500 births) in USA( 1/14,000 births in Blocks) in Asian Americans 1/25,500 births , Median survival age for C.F. improved between 1938 and 1998 from 5 y to almost 30 y . تم بحمد هللا