Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Intersex medical interventions wikipedia , lookup
Human penis wikipedia , lookup
Urinary tract infection wikipedia , lookup
Interstitial cystitis wikipedia , lookup
Kidney stone disease wikipedia , lookup
Kidney transplantation wikipedia , lookup
IgA nephropathy wikipedia , lookup
Chronic kidney disease wikipedia , lookup
Autosomal dominant polycystic kidney disease wikipedia , lookup
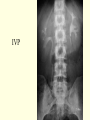
Introduction to Urology Richard E. Freeman MD MPH Curtis M. Grenoble, MS, PA-C Lock Haven University, PA Program Summer 2013 Urology The branch of medicine that focuses on the urinary tracts of BOTH females and males, and the reproductive systems of males. Anatomy of Kidney Renal cortex: outer 1 cm Renal medulla: renal columns, pyramids - papilla Lobe of kidney: pyramid and it’s overlying cortex Collecting system Calyces Pelvis Ureter Lobe of Kidney Nephron Functional unit of the kidney Each human kidney contains about 1 million nephrons A nephron consists of the glomerulus or renal corpuscle, the proximal tubule, the thin loops of Henle, and the distal tubule, all of which originate from the: metanephric blastema. Renal Function can be divided into THREE Components Filtration Excretion Secretion RENAL FUNCTION FILTRATION EXCRETION SECRETION:hormonal- Renin-angiotensin Nephron – Physiology Glomerulus Filters fluid from blood into Bowman’s capsule; Prevents passage of bloods and proteins Proximal convoluted tubule – Reabsorbs 2/3 of water & electrolytes; and all filtered bicarbonate, glucose, amino acids and vitamins Descending Loop of Henle – Reabsorbs water Delivers concentrated filtrate to ascending loop Ascending Loop of Henle – Reabsorbs Na, Cl, K, Produces a hypo-osmotic filtrate and high interstitial osmolality GLOMERULUS Nephron - Physiology Distal Convoluted tubule – Reabsorbs Na+, Cl-, water, urea Secretes H+, K+ Responds (has receptors for) to aldosterone Collecting Tubule – Reabsorption of water under influence of ADH Secretes H+ & K Renal Vasculature 20-25% of cardiac output passes through the kidney Afferent arterioles Branches of the interlobular arteries to transport blood into glomerulus Each supplies a single glomerulus (renal corpuscle) Efferent arterioles Exit the glomeruli Divide to form an intricate peritubular microcirculation Renal Function In a 70-kg person, renal blood flow (RBF) amounts to one fourth to one fifth of the resting cardiac output, or 1.2 liters per minute With one kidney removed, blood flow to the remaining kidney will nearly double within a few weeks (reserve capacity). Glomerular filtration rate Glomerular filtration rate (GFR) is the volume of fluid filtered from therenal (kidney) glomerular capillaries into the Bowman's capsule per unit time. BASED ON THREE FACTORS: Blood flow in (afferent arterioles) HEALTH OF THE GLOMERULUS Blood flow out (efferent arterioles) Juxtaglomerular Apparatus ← ← Factors Affecting GFR Decrease in RBF Decrease in glomerular hydrostatic pressure Decrease in systemic BP Afferent arteriolar constriction Efferent arteriolar dilation Increase in hydrostatic pressure in Bowman’s capsule ureteral obstruction edema of kidney inside a tight capsule Factors Affecting GFR Decrease in concentration of plasma proteins Oncotic pressure Decrease in total area of glomerular capillary bed Diseases that destroy glomeruli without destroying tubules Partial nephrectomy Factors Affecting GFR Opposite effects that decrease GFR Increased permeability of glomerular filtrate… DM Membranous nephropathy Evaluation of renal function/ Blood tests CBC Electrolytes Glucose BUN Creatinine CREATININE CLEARANCE TEST Liver function Ca, PO4 albumin cholesterol Evaluation of Kidney function URINE TESTS Urinalysis – STAY TUNED Creatinine Clearance Test 24 Urine Protein A lot of specialized tests to access metabolic/dynamic function of the kidneysNEPHROLOGY Ureter Tube between kidney and bladder Enters bladder at the ureterovesicular junction Peristalsis ‘THREE areas of narrowing Renal pelvoureterojunction Passage over iliac vessels and pelvic brim Uretervesicular junction’ – oblique angle UV junction Urinary Bladder Holds approximately 500 cc of urine Lined with Transitional cells Body of bladder – primarily detrusor muscle Neck of bladder – includes the posterior urethral sphincter AKA internal sphincter Innervation Sympathetic to body – L2 Parasympathetics to body and neck - S2 & S3 Urinary Bladder and Urethra - Female Female Urethra 3 to 4 cm long External urethral orifice between vaginal orifice and clitoris Internal urethral sphincter detrusor muscle thickened, smooth muscle, involuntary control External urethral sphincter skeletal muscle, voluntary control Male Bladder and Urethra Urethra: ~18 cm long Internal urethral sphincter External urethral sphincter •3 regions 1) prostatic urethra during orgasm receives semen 2) membranous urethra passes through pelvic cavity 3) spongy (penile) urethra Male Reproductive System Male Duct System: posterior view Testis and Associated Structures •Oval organ, 4 cm long x 2.5 cm in diameter •Tunica albuginea: white fibrous capsule •Tunica vaginalis: derived from the peritoneum •Testicular veins drain to the inferior vena cava arteries come from abd aorta •Seminiferous tubules drain into network called rete testis Male Inguinal & Scrotal Region Accessory Glands Seminal vesicles posterior to bladder empty into ejaculatory duct Prostate gland below bladder, surrounds urethra and ejaculatory duct 2 x 4 x 3 cm Bulbourethral glands near bulb of penis empty into penile urethra lubricating fluid Anatomy of the Penis Penis Internal root and visible shaft and glans external portion is ~4 in. long when flaccid skin over shaft is loosely attached allowing expansion extends over glans as prepuce or foreskin Consists of 3 cylindrical bodies of erectile tissue single corpus spongiosum along ventral side of penis encloses penile urethra ends as a dilated bulb ensheathed by bulbospongiosus muscle paired corpora cavernosa diverge like arms of a Y each crus attaches to pubic arch & is covered with ischiocavernosus muscle SECTION 2 UROLOGICAL DIAGNOSTIC STUDIES Diagnostic Studies--URINE Urinalysis Dipstick& microscopic Debate regarding Microscopic effectiveness Cultures 24 Hour specimens Creatinine Clearance Quantitate Protein Uric Acid/other metabolites Special Studies Bence Jones Protein Urine Protein electrophoresis 24 hour urine protein VMA/Metanephrines/cortisol Electrolytes and its cost Diagnostic Studies ULTRASOUND (trans-abd vs. trans rectal) Relatively non-invasive Good for sizing Prostate Good for estimating post void bladder residual Good for looking at renal or prostate mass density Good for assessing kidney size, shape, stones, hydronephrosis, solid and cystic masses Can be used to help guide biopsy Doppler may be able to evaluate renal arteries IVP- intravenous pyelogram IV contrast injected into blood and is concentrated in the renal collecting system Multiple Xray pictures taken – good assessment of function/obstruction Invasive Contrast may cause Allergic Reactions Presents significant burden on Kidney - check BUN/Creatinine before test Great test for evaluating the “plumbing” IVP IVP with contrast dye in bladder Diagnostic Studies Renal Scans (nuclear study) Great to detect blood flow (dynamic study) Mass evaluation Kidney function Evaluation for Renal Artery Stenosis Cystoscopy Retrograde cytourethrogram SECTION 3 UROLOGICAL H & P CC/HPI FOR THE UROLOGY PATIENT Urologic PAIN Pain (LOSCRATES) Most commonly from either obstruction or irritation (inflammation) Careful hx can often determine site of obstruction Small stones causing obstruction: very painful Large non-obstructing stones: no pain CVA pain and tenderness Prostate: suprapubic, perineal, low back Testicular epididymitis, torsion testicle/testicular appendices, hernia, radiating pain from kidney Penile priapism, Peyronies, phimosis, paraphimosis Other locations? RADIATION IMPORTANT CC/HPI FOR THE UROLOGY PATIENT UROLOGY TERMINOLOGY Dysuria Painful or uncomfortable urination Hematuria-RBC’s in urine Gross vs microscopic Upper or lower tract (casts vs rbcs?) True vs pseudo- things that color urine WholeCells vs Free Hemoglobin Myoglobin – muscle cells Rhabdomyolysis Pyuria – WBC’s in urine Upper versus lower tract Will discuss in UTI Lecture CC/HPI FOR THE UROLOGY PATIENT TIMING AND VOLUME Oliguria- decreased output < 500 ml day Anuria – no urine being made (versus anuresis which is the inability to pass urine) Polyuria- Large Quantities of urine- > 2.5 liters per day Frequency- more than the norm no relationship to volume Incontinence - involuntary loss of urine (Stress, Urgency Incontinence, Overflow incontinence) Nocturia - Nocturnal frequency Enuresis - Urinary incontinence at night Hesitancy- difficulty initiating a stream- straining to go DribblingDecrease force of Strain CC/HPI FOR THE UROLOGY PATIENT Miscellaneous Urological terminology Urologic Erectile Dysfunction Loss of Libido/Anorgasmia Hematospermia Gravel/Stones in urine Pneumaturia; urinating air:Fistula Urethral Discharge clear, purulent, bloody Penile/scrotal Lesions Ulcerative, painful/non-painful Raised, flat Color/texture Past Medical History Diabetes Hypertension Prostate Disease UTI’s Cancer Previous hx of calculi Psychological disorders-Depression TB: urogenital TB Peripheral Vascular Disease Multiple Sclerosis/strokes Sickle Cell Disease Previous Surgery Past Medical History: Medications Classes of medications and effects on urologic system: Decreased libido – antihypertensives (HCTZ) Erectile dysfunction – propranolol, psychotropics Ejaculatory dysfunction – α-adrenergic antagonists, psychotropics Priapism – antipsychotics, antidepressants, antihypertensives Nitric oxide (viagra) Decreased Spermatogenesis – chemo, drugs of abuse Incontinence – Acute renal failure – NSAIDs, contrast dye, antibiotics, chemo Urinary retention or obstructive voiding symptoms – smooth muscle relaxants, diuretics anticholinergics, muscle relaxants, CCB, antiparkinsonian drugs, α-adrenergic antagonists, antihistamines Family History Genetic Disease Polycystic Kidney Disease Tuberous Sclerosis Von Hippel Lindau Disease Renal tubular Acidosis Prostate Cancer Physical Examination of the Urogenital Tract MUST include Kidneys: Attempt to trap, CVA tenderness Abdominal Exam Inspect for distension- bladder Percuss bladder for distension Palpate for masses, tenderness Rectal/Prostate on all Male Rectummasses, tenderness, blood Prostate Size, texture, nodularity, tenderness Dr. Freeman’s 5th commandment “If thou hath a finger and thy patient has an anus- a rectal exam shalt thou do” Pelvic on Females Neurologic Exam Sensory Reflexes -sphincter and muscle tone Physical Examination of the Urogenital Tract GENITAL EXAM maturation Skin Inguinal masses, nodes, hernias Scrotum-Contents Testicles, epididymis, spermatic cord Abnormalities: masses, cysts, tenderness Penis circumcision status size shape tenderness Lesions discharge