Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
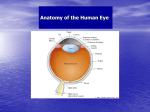
CLINICAL REPORT Unsuccessful Pulsed Radiofrequency of the Sphenopalatine Ganglion in Patients with Chronic Cluster Headache and Subsequent Successful Thermocoagulation Damian Claudio Bendersky, MD; Santiago Matias Hem, MD; Claudio Gustavo Yampolsky, MD Department of Neurosurgery, Hospital Italiano de Buenos Aires, Buenos Aires, Argentina & Abstract: We present the results of pulsed and continuous radiofrequency (CRF) of the sphenopalatine ganglion in a case series of 3 patients with chronic cluster headache (CCH). Three patients were referred to our neurosurgical department because of CCH, which was refractory to pharmacological treatment. They underwent pulsed radiofrequency of the sphenopalatine ganglion (PRF-SPG), and the procedure was performed through an infrazygomatic approach. In the PRF procedures, we applied 2 cycles of PRF at 42°C and 45 V for 120 seconds, with a pulse frequency of 2 Hz and a pulse width of 20 ms. In those procedures where thermocoagulation was carried out, 2 CRF lesions at 80°C for 90 seconds each were performed. Following corticosteroid and local anesthetic (40 mg of methylprednisolone and 1 mL of 1% lidocaine) injection, 2 patients had no pain relief at all, whereas the third one experienced a partial response, which lasted only 1 month and his pain then returned to its baseline level. Thus, this outcome was assessed as a nonsustained partial response. Therefore, all of them underwent a CRF lesioning of the SPG, and after this procedure, they achieved complete pain relief until the end of the follow-up period. Further- n Claudio Address correspondence and reprint requests to: Damia noma de Buenos Bendersky, MD, Juan Domingo Peron 4190, Ciudad Auto Aires C1181ACH, Argentina. E-mail: [email protected]. Submitted: August 11, 2014; Revised: December 7, 2014; Revision accepted: December 9, 2014 DOI. 10.1111/papr.12288 © 2015 World Institute of Pain, 1530-7085/15/$15.00 Pain Practice, Volume 15, Issue 5, 2015 E40–E45 more, the associated autonomic manifestations disappeared. The 3 patients presented in this case series failed to achieve adequate pain relief after PRF-SPG. However, these same patients subsequently underwent a successful CRF of the SPG. & Key Words: cluster headache, sphenopalatine ganglion, pulsed radiofrequency, continuous radiofrequency, thermocoagulation INTRODUCTION Cluster headache (CH) is a trigeminal autonomic cephalalgia, a condition that is characterized by severe unilateral headache and cranial parasympathetic manifestations.1–9 Approximately 10% to 15% of patients develop chronic cluster headache (CCH).6,7,10,11 Although its treatment is essentially pharmacological, involving both prophylactic and acute measures, up to 15% to 20% of patients do not respond adequately to conservative management. In these cases, as well as those in which the side effects of the medications are intolerable a sphenopalatine ganglion (SPG) block may be indicated. Although several methods for blockade are proposed in the literature, we previously used continuous radiofrequency (CRF) of the SPG in patients with medically refractory CCH.2,5–8,10–13 However, there may be some complications following this procedure, such as hyperpathia or deafferentation pain in PRF of the Sphenopalatine Ganglion E41 theterritoryofthemaxillarybranchofthetrigeminalnerve; permanent or transient hypesthesia; hypersensitivity or dysesthesia in the palate; maxilla;, gums; cheek or posterior pharynx; in addition to dryness of the eye and reflex bradycardia during radiofrequency lesioning.2–4,7,10,11,14 Thus, we decided to try pulsed radiofrequency (PRF), a nondestructive method which was found to be effective in other studies for this and other pain conditions, to avoid complications due to neural tissue damage.3,4,11,14,15 We present a case series of 3 patients with CCH who underwent pulsed radiofrequency of the sphenopalatine ganglion (PRF-SPG) without obtaining adequate pain relief. Finally, these patients achieved complete pain relief following CRF plus SPG block. CASE SERIES Between January and May 2013, 3 patients were referred to our neurosurgical department because of unbearable headache. All of them fulfilled the diagnostic criteria of the International Headache Society (IHS) for CH (Table 1). The subjects were evaluated and treated by a neurologist who specialized in headaches. These patients tried several pharmacological treatments before being referred to our department, but the results were poor. The 3 patients suffered from CCH, as their headache presented remission periods, which lasted < 1 month, or they did not have remission periods, depending on each case.1 After giving written consent for the procedure, they underwent PRF-SPG without a previous diagnostic block of this ganglion. The intensity and frequency of the pain attacks were measured before and after the procedure. The former variable was evaluated with the visual analog scale (VAS). We Table 1. Diagnostic criteria of the International Headache Society for cluster headache (ICHD-3)1 A. At least 5 attacks fulfilling criteria B to D B. Severe or very severe unilateral orbital, supraorbital, and/or temporal pain lasting 15 to 180 minutes (when untreated) C. Either or both of the following: At least one of the following symptoms or signs, ipsilateral to the headache: Conjunctival injection and/or lacrimation Nasal congestion and/or rhinorrhoea Eyelid edema Forehead and facial sweating Forehead and facial flushing Sensation of fullness in the ear Miosis and/or ptosis A sense of restlessness or agitation D. Attacks have a frequency between one every other day and 8 per day for more than half of the time when the disorder is active E. Not better accounted for by another ICHD-3 diagnosis assessed the outcome of the procedure as follows: complete response (complete pain relief); partial response (≥ 50% reduction of intensity and frequency of the pain attacks); and poor response (not reaching the criteria for partial response or no pain relief at all). In case of pain relapse, we would have repeated the PRFSPG if there was a sustained complete or partial response following the first procedure. However, we would have performed a CRF lesioning of the SPG in the event of a poor response. Procedural Technique The procedure was performed through an infrazygomatic approach, as described in the literature.2–4,7,10,11,13– 17 It is carried out under fluoroscopic guidance, with the patient in supine position. The pterygopalatine fissure is visualized with lateral fluoroscopy. Although the needle may also be inserted anterior to the mandible, we use a point in the coronoid notch just below the inferior edge of the zygomatic arch as the entry point. Following subcutaneous injection of 2 mL of 1% lidocaine, a 20-g, 10-cm needle with 5-mm active tip is introduced using lateral fluoroscopy. It must be noted that the usage of a curved cannula may facilitate the procedure. The needle tip must be located within the pterygopalatine fossa, just lateral to the nasal wall. Next, an anteroposterior view is obtained to check the needle position, which should be at the level of the middle turbinate. If it is properly placed, we can pass to the next step, or else we must correct its position. Then, its location is neurophysiologically verified by sensory stimulation at 50 Hz. Paresthesia should be elicited at the roof of the nose. If paresthesia is felt in the upper teeth, cheek, and/or upper lip, the electrode is stimulating the maxillary nerve or its branches and the needle must be repositioned caudally and medially. If paresthesia is present in the hard palate, the greater and lesser palatine nerves are being stimulated and thus, the tip of the electrode must be moved posteriorly, medially, and superiorly.10,11,13,17 When the surgeon believes that the cannula is in the target, PRF or CRF is performed. In PRF procedures, we applied 2 cycles of PRF at 42°C and 45 V for 120 seconds, with a pulse frequency of 2 Hz and a pulse width of 20 ms. In those procedures in which thermocoagulation was carried out, 2 CRF lesions at 80°C for 90 seconds each were performed. Corticosteroid and local anesthetic (40 mg of methylprednisolone and 1 mL of 1% lidocaine) injection within the pterygopalatine fossa was carried out only when CRF was used. E42 BENDERSKY ET AL. RESULTS The demographic variables and pain characteristics of the 3 patients are shown in Table 2. Following PRF-SPG, 2 patients had no pain relief at all, whereas the third one experienced a partial response, which lasted only 1 month. His pain then returned to its baseline level. Thus, this outcome was assessed as a nonsustained partial response. Therefore, all patients underwent a CRF lesioning of the SPG. After this procedure, they achieved complete pain relief until the end of the follow-up period. Furthermore, the associated autonomic manifestations disappeared. There were no complications in this case series, including PRF and CRF procedures. The first patient was a 53-year-old woman who started with right episodic CH 15 years before being referred to our department. She was initially treated with verapamil as prophylaxis, while sumatriptan and oxygen inhalation were used for acute episodes. Nine years after the diagnosis, her episodic headache evolved to CCH. She had remission periods, which lasted < 1 month. Other drugs were tried (ergotamine and topiramate) but had little to no effect. Finally, she was referred to us 14 months ago. She underwent right PRF-SPG without response. Three months later, the patient accepted to undergo a CRF of the SPG and following the thermoco- agulation, she achieved complete pain relief until the end of the 11-month follow-up period. Currently, she remains on verapamil for prophylactic therapy. The second patient was a 37-year-old woman with right CCH since age 33. Her headache arose de novo and was associated with several autonomic signs and symptoms. She never had remission periods. At the beginning, verapamil was used for prophylactic treatment. It was useful for < 2 years, when the headache became refractory to pharmacological treatment despite using not only first-tier drugs, but also second-tier ones: lithium, topiramate, carbamazepine, pregabalin, and amitriptyline. First, she had good response to corticosteroids, but then her pain became unresponsive to it. Given her refractory pain, right PRF-SPG was carried out, but she did not achieve any pain relief. Four months following this first procedure, CRF of the same ganglion was performed. Thereafter, she has suffered no headache for the next 8 months. She is receiving only topiramate for prophylaxis. The last patient was a 36-year-old man who started with left CCH 7 years before the PRF-SPG. He did not present remission periods, and his major complaints were pain as well as eyelid edema and lacrimation. All prophylactic drugs used (i.e., verapamil, lithium, Table 2. Demographic variables and pain characteristics Patient 1 Patient 2 Patient 3 Age Gender Location of pain Type of cluster headache Associated autonomic manifestations 53 Female Supraorbital/temporal Chronic Conjunctival injection, lacrimation, nasal congestion, and rhinorrhoea Mechanical allodynia Average frequency of attacks (before PRF-SPG) Intensity (VAS) of pain during the attacks (before PRF-SPG) Duration of each attack (before PRF-SPG) Average frequency of attacks (1 week after PRF-SPG) Intensity (VAS) of pain during the attacks (1 week after PRF-SPG) Duration of each attack (1 week after PRF-SPG) Response to PRF-SPG Associated autonomic manifestations (1 week after PRF-SPG) Response to CRF of the SPG Associated autonomic manifestations after CRF of the SPG Present 3/day 37 Female Orbital/supraorbital Chronic Conjunctival injection, lacrimation, nasal congestion, rhinorrhoea, facial sweating, and ptosis (mild) Present 4/day 36 Male Orbital/supraorbital/temporal Chronic Eyelid edema, lacrimation, conjunctival injection, nasal congestion, and rhinorrhoea Present 4/day 10 10 10 2 to 3 hours 1 to 2 hours 2 to 3 hours 3/day 4/day 1/day 10 10 5 2 to 3 hours 1 to 2 hours 2 to 3 hours Poor No improvement Poor No improvement Partial (nonsustained) Partial improvement Complete Disappeared Complete Disappeared Complete Disappeared CRF, continuous radiofrequency; PRF, pulsed radiofrequency; PRF-SPG, pulsed radiofrequency of the sphenopalatine ganglion; VAS, visual analog scale. PRF of the Sphenopalatine Ganglion E43 topiramate) were ineffective, and he needed abortive treatment of the acute attacks very frequently. The patient developed depression during the course of his treatment with topiramate. The topiramate was suspended and verapamil was restarted, since the former was unhelpful and depression is a known adverse effect of this drug. Verapamil failed again and thus, lithium was tried. He achieved minimal results with this therapy, and therefore, PRF-SPG was carried out 1 year ago. Following the intervention, he experienced a marked reduction of both intensity and frequency of the pain attacks; nevertheless, the associated autonomic manifestations diminished, but they were still present. Unfortunately, this partial response lasted only 1 month. Six weeks after the relapse, the patient was desperate for a long-term solution. At last, he underwent CRF of the SPG and since then, he had no pain attacks, despite not using prophylactic treatment currently. Almost 10 months later, he is still asymptomatic. changes.18 It is important since the pain of CH is thought to be due to activation of the ophthalmic nerve.8 CH, as well as the other identified trigeminal autonomic cephalalgias, involves the activation of the trigeminal autonomic reflex, whose afferent limb is the trigeminal nerve and the efferent one is represented by the parasympathetic fibers of the greater superficial petrosal nerve.9,20 One hypothesis about its physiopathology is that efferent parasympathetic outflow from the SPG may both initiate autonomic manifestations and activate trigeminovascular sensory afferents, which in turn may initiate the pain.18 The increased parasympathetic outflow may be originated centrally because of a hypothalamic disturbance, with likely involvement of a trigemino-hypothalamic pathway. Also, descending fibers from the hypothalamus to the trigeminal nucleus caudalis could trigger the pain.6,8,19 As mentioned previously, there may be some complications following CRF of the SPG. Almost all of DISCUSSION The SPG is located within the pterygopalatine fossa, just below the maxillary nerve. Despite being a parasympathetic ganglion, it also receives sensory, motor, and sympathetic roots (Figure 1). These connections of the SPG, as well as its anatomical location, may help in understanding the physiopathology of the CH and the complications following the ablation of this ganglion. Even though the physiopathology of CH is still unknown, the hypothalamus is thought to be the generator of this disease because of its circadian and circannual periodicity and the activation of the posterior hypothalamus found in neuroimaging studies that were undertaken during the attacks. Furthermore, activation of the parasympathetic outflow from the superior salivary nucleus via the SPG is supposed, explaining the autonomic manifestations of CH and the likely role of the SPG at least in this aspect of the disease.4–6,8–11,18,19 Indeed, it was shown that low frequency (5 Hz) SPG stimulation could induce cluster-like attacks with autonomic features. According to the explanation of the authors, this induction may be due to the release of neurotransmitters from parasympathetic efferents, which activate or at least modulate trigeminal nociceptors. On the other hand, high frequency (80 to 120 Hz) SPG stimulation may activate sensory fibers from the maxillary nerve, which converge in the trigeminal nucleus caudalis with afferents from the ophthalmic branch, leading to antinociceptive modulatory Figure 1. The parasympathetic root has its origin in the superior salivary nucleus (SSN), and these preganglionic axons pass through several neural structures before reaching the SPG: nervus intermedius (or nerve of Wrisberg) (NI), facial nerve (FN), geniculate ganglion (GG), greater superficial petrosal nerve (GSPN), and vidian nerve (VN). The parasympathetic fibers synapse in the SPG, and the postganglionic fibers innervate the nasal cavity, the mucosa of the palate, the nasopharynx, and the lacrimal gland. The sympathetic root is formed by postganglionic fibers from the superior cervical ganglion (SCG), which travel through the internal carotid plexus (ICP), the deep petrosal nerve (DPN) and the VN before entering the SPG. These axons do not synapse in the SPG, and they are distributed to the nasal cavity and pharynx. The sensory root comes from the maxillary nerve, and its fibers innervate the nose, throat, and sinuses. The motor root seems to be derived from the NI, and it may actually be a bundle of sympathetic fibers which arise in the brainstem.2,3,11,14,20 E44 BENDERSKY ET AL. them can be explained by its close proximity with the maxillary nerve and its branches. Indeed, hypesthesia of the palate may be seen as a predictable consequence of CRF of the SPG.3,4,10,11,14 Sanders and Zuurmond reported that maxillary hyperpathia was the major complication in 6.1% of 66 patients treated with CRF of this ganglion.10 The rationale for using PRF-SPG is to avoid these complications, as PRF, unlike CRF, is thought to produce its effects by creating high intensity electric fields without generating relevant thermal injury of the neural tissue surrounding the tip of the electrode. The tissue temperature rise using a certain voltage is much less for PRF than for CRF because the pulse duration is only a small percentage of the time between pulses. Thus, CRF is used for tissue destruction, whereas PRF would be useful for those cases in which CRF may produce complications or side effects due to thermal injury.3,4,10,14,21–23 The authors believe that both an accurate needle placement and the usage of electrical stimulation during the procedure are essential to decrease the occurrence of complications of CRF. We found only 3 articles in which PRF-SPG was used, and all of them achieved good results following the procedure. However, these studies included other types of facial pain than CCH.4,14,15 In the article of Bayer et al., only 27% of 30 patients were diagnosed with SPG neuralgia (entity that is now classified as CH by the IHS), while atypical facial pain was the most frequent etiology. All patients had a previous positive response to a diagnostic block of the SPG. After PRF-SPG, 14% reported no pain relief, whereas 21% and 65% had complete and mild-to-moderate pain relief, respectively.14 Chua et al. presented 2 patients with CCH and 1 patient with episodic CH who underwent PRFSPG. There was a complete response in 2 of them and a partial response in the other one. Nevertheless, the follow-up period was quite short, lasting only 4 months.4 Shah and Racz reported a case in which PRF-SPG was used to treat post-traumatic headache. Following the intervention, this patient obtained longterm pain relief.15 There are several topics that should be discussed. First, we believe that the major limitation of our case series is the small number of patients; furthermore, this is a retrospective study. Second, all of our patients had CCH, which is thought to have worse results after CRF of the SPG than episodic CH.7,10 In fact, Sanders and Zuurmond reported that 60.7% of 56 patients with episodic CH and 30% of 10 patients suffering from CCH achieved complete pain relief following CRF. Because of the small number of patient with CCH in their study, the authors concluded that CRF of the SPG is effective only for episodic CH.10 Third, regarding PRF parameters, we used the same as those of Bayer et al.14 We used the above mentioned parameters because they were effective in the previous case series, and we have used these parameters for PRF of the dorsal root ganglion. Chua et al. (4 Hz, 42°C, 10 ms, 45 V, 6 minutes), as well as Shah and Racz (2 Hz, 42°C, 20 ms, 6 minutes), used other settings.4,15 We cannot rule out that other PRF parameters may be more effective than those utilized in this study. Fourth, all patients in our series had mechanical allodynia, which may be associated with reduced response to treatment, although it was not demonstrated for CH.4,24 In the study of Chua et al.,4 the only patient who had allodynia experienced less pain relief than the other 2. Fifth, we cannot conclude if the success of the last procedure was due to the CRF of the SPG, the corticosteroid injection within the pterygopalatine fossa, or a combination of both treatments. For example, Sanders and Zuurmond achieved good results after CRF without performing corticosteroid injection in the SPG, whereas Pe~ narrocha-Diago also reported favorable results following SPG corticosteroid injection alone.5,10 Other authors, as we did in this article, carry out both treatments during the same procedure.7,11 However, anesthetic blockade, plus corticosteroid injection, seems to produce only temporary improvement.2,3,5,25 Sixth, we must comment that the only patient who achieved some improvement in autonomic manifestations also experienced at least some pain relief following PRF-SPG. Furthermore, all patients were free of autonomic manifestations after CRF of the SPG. It could be related to the interruption of the parasympathetic fibers in the SPG. It also shows the relationship between pain and parasympathetic manifestations. SUMMARY The 3 patients presented in this case series failed to achieve adequate pain relief after PRF-SPG. However, these same patients subsequently underwent a successful CRF of the SPG. Thus, we will continue to perform CRF of this ganglion for CCH patients until the availability of higher level evidence of the efficacy of PRF-SPG in this population. PRF of the Sphenopalatine Ganglion E45 REFERENCES 1. Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders, 3rd edition (beta version). Cephalalgia. 2013;33:629–808. 2. Day M. Sphenopalatine ganglion analgesia. Curr Rev Pain. 1999;3:342–347. 3. Piagkou M, Demesticha T, Troupis T, et al. The pterygopalatine ganglion and its role in various pain syndromes: from anatomy to clinical practice. Pain Pract. 2012;12:399–412. 4. Chua NH, Vissers KC, Wilder-Smith OH. Quantitative sensory testing may predict response to sphenopalatine ganglion pulsed radiofrequency treatment in cluster headaches: a case series. Pain Pract. 2011;11:439–445. 5. Pe~ narrocha-Diago M, Boronat A, Pe~ narrocha-Oltra D, Ata-Ali J, Bagan JV, Pe~ narrocha-Diago M. Clinical course of patients with episodic cluster headache treated with corticosteroids in proximity to the sphenopalatine ganglion: a preliminary study of 23 patients. Med Oral Patol Oral Cir Bucal. 2012;17:e477–e482. 6. McGeeney BE. Cluster headache pharmacotherapy. Am J Ther. 2005;12:351–358. 7. Narouze S, Kapural L, Casanova J, Mekhail N. Sphenopalatine ganglion radiofrequency ablation for the management of chronic cluster headache. Headache. 2009;49:571–577. 8. May A. Cluster headache: pathogenesis, diagnosis, and management. Lancet. 2005;366:843–855. 9. Goadsby PJ. Trigeminal autonomic cephalgias (TACs). Acta Neurol Belg. 2001;101:10–19. 10. Sanders M, Zuurmond WW. Efficacy of sphenopalatine ganglion blockade in 66 patients suffering from cluster headache: a 12- to 70-month follow-up evaluation. J Neurosurg. 1997;87:876–880. 11. Narouze SN. Role of sphenopalatine ganglion neuroablation in the management of cluster headache. Curr Pain Headache Rep. 2010;14:160–163. 12. Tepper SJ, Stillman MJ. Cluster headache: potential options for medically refractory patients (when all else fails). Headache. 2013;53:1183–1190. 13. Day M. Neurolysis of the trigeminal and sphenopalatine ganglions. Pain Pract. 2001;1:171–182. 14. Bayer E, Racz GB, Miles D, Heavner J. Sphenopalatine ganglion pulsed radiofrequency treatment in 30 patients suffering from chronic face and head pain. Pain Pract. 2005;5:223–227. 15. Shah RV, Racz GB. Long-term relief of posttraumatic headache by sphenopalatine ganglion pulsed radiofrequency lesioning: a case report. Arch Phys Med Rehabil. 2004;85:1013–1016. 16. Oomen KP, van Wijck AJ, Hordijk GJ, de Ru JA. Effects of radiofrequency thermocoagulation of the sphenopalatine ganglion on headache and facial pain: correlation with diagnosis. J Orofac Pain. 2012;26:59–64. 17. de Andres J, Dıaz L, Cid J y G omez Caro L. Bloqueo y radiofrecuencia del ganglio esfenopalatino para el tratamiento de algias faciales. Rev Soc Esp Dolor. 2011;18:303–310. 18. Schytz HW, Barløse M, Guo S, et al. Experimental activation of the sphenopalatine ganglion provokes cluster-like attacks in humans. Cephalalgia. 2013;33:831–841. 19. Pedersen JL, Barloese M, Jensen RH. Neurostimulation in cluster headache: a review of current progress. Cephalalgia. 2013;33:1179–1193. 20. Khan S, Schoenen J, Ashina M. Sphenopalatine ganglion neuromodulation in migraine: what is the rationale? Cephalalgia. 2014;34:382–391. 21. Chua NH, Vissers KC, Sluijter ME. Pulsed radiofrequency treatment in interventional pain management: mechanisms and potential indications-a review. Acta Neurochir (Wien). 2011;153:763–771. 22. Van Zundert J, Lame IE, de Louw A, et al. Percutaneous pulsed radiofrequency treatment of the cervical dorsal root ganglion in the treatment of chronic cervical pain syndromes: a clinical audit. Neuromodulation. 2003;6:6–14. 23. Bogduk N. Pulsed radiofrequency. Pain Med. 2006;7:396–407. 24. Burstein R, Collins B, Jakubowski M. Defeating migraine pain with triptans: a race against the development of cutaneous allodynia. Ann Neurol. 2004;55:19–26. 25. Felisati G, Arnone F, Lozza P, Leone M, Curone M, Bussone G. Sphenopalatine endoscopic ganglion block: a revision of a traditional technique for cluster headache. Laryngoscope. 2006;116:1447–1450.