Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
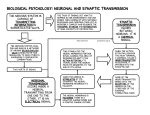
The Anatomy and Physiology of Lifting Your Arm Kelly Nicole Boden Human Anatomy and Physiology January 23, 2013 1 R6 Introduction: There are many seemingly simple actions your body makes every day that appear to be easy, effortless, and takes no thought. That would be incorrect. Even the simplest action, like lifting up your arm, is a complex feat of the finely tuned instrument that is your body. This apparently simple act of lifting up your arm begins in your brain. Your brain is the command center of your nervous system (the system in charge of telling the other systems what to do). As soon as you decide that you want to lift your arm up, your brain sends an electrical impulse through specific nerves to tell the muscles to contract and lift up your arm. A nerve cell’s membrane is made up of a lipid bilayer; this is formed with two layers of phospholipids. The external side of the membrane is slightly positive; its internal side is slightly negative. The main extracellular ion is sodium (Na+), whereas the main intracellular ion is potassium (K+). The membrane is relatively impermeable to both ions. However, there are channels in the cell membrane which allow these ions to pass through the membrane. The size, shape and charge of each channel allow only a certain type of ion to pass through. Other channels have gates that do not permit ions to pass through it unless it is stimulated. There are also sodium-potassium pumps and they work like this: I. 3 Na+ from the intracellular fluid bind to the pump II. The pump becomes phosphorylated when the 3rd phosphate on the ATP III. The Na+ are released in to the extracellular fluid and the pump changes shape IV. 2 K+ from the extracellular fluid bind to the pump V. The K+ make the pump dephosphorylate and the K+ ions are released in the intracellular fluid. A stimulus comes from the brain and is transported through the neurons and their axons to the intended destination. This stimulus changes the permeability of a “patch” of the membrane, and sodium ions diffuse quickly into the cell. This changes the polarity of the membrane so that the inside becomes more positive and the outside becomes more negative. If the stimulus is strong enough, depolarization causes membrane polarity to be completely reversed and an action potential is initiated. When the stimulus gets to be around -55 mV, the sodium gates open up and let the Na+ ions through. More of the sodium channels open because of this and the cycle of depolarization is created. This is what passes the electrical signal down the axon. Once this 2 depolarization cycle has begun, it continues until the signal reaches the end of the pre-synaptic nerve cell. Once the cell membrane reaches about +30 mV, the sodium channels close, like someone shutting their front gate. This prevents the signal from traveling backwards. After the sodium channel closes, the potassium channel opens as a delayed response to the original stimulus. The K+ ions move out of the axon and make the membrane rapidly repolarize and because the K+ channels are slower to close, the membrane is briefly hyperpolarized. In order to restore the balance of the cell to the resting state of the cell, the sodium/potassium pumps actively transport sodium ions out of the cell and potassium ions into it. Axons that are used more frequently for the same task become myelinated. Myelin sheaths are formed by Schwann cells, and Schwann cells are pretty much a lipid cell layer wrapped around the axon multiple times. Neurons that have myelinated axons transmit signals faster than neurons with unmyelinated axons. This is because the sodium, potassium, and sodium-potassium pumps are located between each Schwann cell; allowing the signal to travel farther before activating the channels. Fun fact: myelinated axons are harder to retrain. There is not a single long nerve that travels from the brain to the destination; there are many nerve cells that form a chain from the brain to the destination. A synapse is a junction formed by two neurons and allows the neurons to communicate and pass along the signals. The transmitting neuron is called the presynaptic neuron, and the receiving neuron is called the postsynaptic neuron. The axon of the presynaptic neuron ends in a synaptic knob that is practically touching the postsynaptic neuron, but is separated by the synaptic cleft. When the action potential arrives at the end of the synaptic knob, it triggers the calcium ion channels and makes them open. This allows Ca2+ to flood into the synaptic knob. The Ca2+ causes the synaptic vesicles to fuse with the presynaptic membrane. These vesicles store acetylcholine and ACh is used as the neurotransmitter molecules. The ACh neurotransmitters move across the synaptic cleft and attach themselves to the acetylcholine receptors that are in the postsynaptic neuron. These receptors are channels that have gates that are closed until activated by the ACh neurotransmitters. When the channels open, sodium and potassium diffuse through the postsynaptic membrane and change the postsynaptic membrane’s potential. The postsynaptic neuron’s membrane has potassium leak channels that allow K+ to diffuse freely out of the cell. Once the acetycholine activates the process of depolarization in the postsynaptic cell, they are then broken down by the enzyme acetylcholinesterase. The choline is absorbed back into the 3 presynaptic neuron and made into new acetycholine in the vesicles in the presynaptic cell. Once the ACh has been broken down, the gated receptors close again. The sodium-potassium pumps then work to restore the equilibrium of the postsynaptic neuron. This process is the stimulus that continues the signal from the brain to the destination site. The signal goes from neuron to neuron this way. At the neuromuscular junction, a synapse is formed by a motor neuron and sarcolemma of a muscle fiber. At this junction, the neuron passes the electrical signal to the muscle cell tells the muscle cell what to do. The transmitting neuron is called the presynaptic neuron, and the axon of the presynaptic neuron ends in a synaptic knob that is practically touching the muscle fiber at the axonal terminal, but is separated by the synaptic cleft. When the action potential arrives at the end of the synaptic knob, it triggers the calcium ion channels and makes them open. This allows Ca2+ to flood into the synaptic knob. The Ca2+ causes the synaptic vesicles to fuse with the presynaptic membrane. These vesicles store acetylcholine and ACh is used as the neurotransmitter molecules. The ACh neurotransmitters move across the synaptic cleft and attach themselves to the acetylcholine receptors that are in the muscle fiber membrane. These receptors are channels that have gates that are closed until activated by the ACh neurotransmitters. When the channels open, sodium ions diffuse through the muscle fiber’s membrane and depolarize the postsynaptic membrane. The postsynaptic action potential is made and spreads over the muscle cell membrane. Once the acetycholine activates the process of depolarization in the muscle fiber cell, they are then broken down by the enzyme acetylcholinesterase. The choline is absorbed back into the presynaptic neuron and made into new acetycholine in the vesicles in the presynaptic neuron. Once the ACh has been broken down, the gated receptors close again. This is the destination of the brain stimulus sent through the nerves to end with the chemical process of turning an electrical signal in the presynaptic neuron to an electrical signal in the muscle fiber. It is very similar to what happens between neuron synapses. All nerve paths begin in your brain then travel down your spinal cord. Your spinal cord is like a highway for the nerves. If the signal’s destination is somewhere in the arm, the nerve impulse would leave the spinal cord at any of the exits between the C4 and T2 bones. It depends exactly where in the arm the signal is going to determine what exit to take. If the signal is to tell the deltoid to contract and abduct the arm, then the signal would exit at C5 and C6, go through the C5, C6 roots to the upper trunk. From the upper trunk, the signal would move to axillary 4 nerve via the posterior division. The axillary nerve then transmits the signal to the deltoid via the neuromuscular junction. Once the signal has been passed from nerve to nerve, and nerve to muscle via the neuromuscular junction, the informed muscle cells contract. Skeletal muscle cells, myofibers, are long and narrow cells. Interesting fact: because the myofibers are so long, they have multiple nuclei. The muscle cell is surrounded by a lipid bilayer membrane (sarcolemma); this encloses the sarcoplasm and the myofibrils. Myofibrils are bundles of contractile proteins. The myofibril is made up repeating subunits called sarcomeres. The lateral boundaries of a sarcomere are made with the protein plates, Z discs. In between the Z discs, there are thin filaments and thick filaments. The thin filaments extend from the Z discs towards the center where they partially overlap with the thick filaments. The thin filaments are made up of G actin (globular actin) that attach end to end to form two twisted strands. These two strands are called F actin (fibrous actin) and nebulin span the length of the F actins and act as measuring sticks for the F actin. To prevent the F actin from unraveling, the strands are capped on the medial end by tropomodulin, and by Cap Z on the lateral end. The Cap Z is attached to the Z disc by actinin proteins. When the muscle fiber is at rest, the G actins are covered by a series of tropomyosin proteins. Assositated with each tropomyosin is a troponin molecule. This molecule is what helps the muscle contraction to take place. The thick filaments are composed of myosin molecules. These molecules are made of two heavy chain polypeptides. The tail of each myosin wrap around the tails of all the other myosins. At the other end of the heavy chains there are two globular heads that contain a binding site for actin. These heads are used for moving the thin filaments during contraction. During the contraction, the myosin heads bind to the G actins in the thin filaments and pull the thin filaments towards the center of the sarcomere. However, the tropomyosins cover the F actin binding sites. In order to uncover the binding sites, calcium (C2+) must bind to the troponin protein complex. This makes the troponin complex to change shape and move the tropomyosin away from the binding sites. The action potential passes from the neurons through the neuromuscular junction to the muscle fibers and releases the calcium ions into the sarcolemma to initiate this contraction process. The contracting muscles move the bones they are attached to and complete the desired motion, in this case, lifting your arm up from your side with your palm to the ground. The nerves 5 tell the muscles what to do, but the nerves do not give the energy or nutrients to the muscles that the muscles need to do their jobs. That is the blood’s job. Blood is made up of three basic parts. The first part is the red blood cells (RBCs), or erythrocytes. RBCs make up about 45% of the total blood volume. The second part is the white blood cells (WBCs), or leukocytes. They only make up about 1% of the blood volume. The final part is the plasma. Plasma makes up about 55% of the blood volume and is mostly water with dissolved solutes. These solutes are proteins, nutrients, electrolytes, nitrogenous wastes, respiratory gases, and regulatory compounds. The RBCs are the oxygen transporters, the WBCs are the disease fighters, and the plasma is the liquidy thing the RBCs and WBCs travel around the body through. RBCs have no nuclei or organelles; they are merely temporary hemoglobinfilled vehicles that transport the much-needed oxygen throughout the body. In order for the RBCs to do their job of exchanging oxygen and carbon dioxide, they need hemoglobin proteins. These proteins are made up of two alpha subunits and two beta subunits. Each of the subunits have a heme group surrounded by a long globin polypeptide; two histidine molecules hold the heme group in place. The hemoglobin bind and release oxygen molecules; this process is what makes the RBCs red and purple. When the hemoglobin has oxygen, the RBC is red. Once the hemoglobin releases the oxygen, it turns purple. The RBCs also create and store an enzyme called carbonic anhydrase. This enzyme converts the CO2 to HCO3. The HCO3 is water soluble and is released into the plasma until the blood goes back through the lungs where the HCO3 is converted back into CO2 and exhaled. The blood travels through arteries to get from the heart to the destination and gets back to heart through the veins. The arteries branch off and the branches become narrower arterioles. The arterioles begin branching off and become even narrower capillaries. The capillaries are one blood cell wide and tiny muscle contractions massage the cells through the capillary network. It is at the capillary networks that the exchanging of wastes, oxygen, and nutrients occur between the blood cells and the muscle cells. The blood passes from the arterial capillaries, through the endothelium, and out the venous capillaries. The venous capillaries converge into venules, and venules converge into veins which transport the blood back to the heart. There are two exceptions. They are the pulmonary artery and veins. The pulmonary artery carries unoxygenated blood from the heart to the lungs, and the pulmonary veins bring the oxygenated blood back to the heart. So while generally arteries carry oxygenated blood and veins carry unoxygenated 6 blood, the defining factor of what is an artery and what is a vein is whether the blood it carries is moving away (arteries) or towards (veins) the heart. The heart is a very complex bio-machine that mixes and controls the oxygenation of the blood. Unoxygenated blood enters the heart through the superior vena cava and inferior vena cava. The superior vena cava and inferior vena cava empty the unoxygenated blood into the right atrium. The A-V tricuspid valve opens and the unoxygenated blood passes from the right atrium to the right ventricle. From the right ventricle, the blood flows through the pulmonary artery to the lungs. The now oxygenated blood goes back to the heart through the pulmonary veins. The pulmonary veins empty the oxygenated blood into the left atrium. The A-V bicuspid valve opens and the oxygenated blood passes into the left ventricle. The oxygenated blood then leaves the heart via the aorta artery to be sent throughout the body. Once the oxygen is used up, the blood returns to the heart to repeat the cycle. 7 Summary The movement in question is the abduction of the arm (it does not matter which) from the neutral position at the side of the body to the point where the arm is pronated (palm faces the ground) and parallel to the floor. In order to do this, the muscles in ‘Table 1: Muscles’ in the Appendix must be used. A message is sent from your brain through your motor neurons to the muscles desired. In this case, the message is for the deltoid and the teres major to contract and abduct the humerus. The other muscles are used mostly for stabilization and to keep the forearm pronated. In order for the muscles to contract, they need nutrients and oxygen. The muscles get both of these things from the blood supply that flows from the heart to the muscles. The oxygenated blood flows through arteries to get to the muscles, disperses it’s cargo to the muscle and get their wastes in the capillary networks. The unoxygenated blood exits the capillary networks in veins and travels back up to heart to get oxygenated again and repeat the cycle. 8 Appendix Table 1: Muscles Muscle Name Origin Insertion Action Nerve Blood Deltoid tuberosity of humerus Abducts arm; flexion and medial rotation; extension and lateral rotation Axillary nerve C5, C6 Posterior humoral circumflex artery; deltoid branch of thoracoacromial artery Teres Major Inferior lateral margin of scapula Crest of lesser tubercle Assists in adduction of arm, assists in medial rotation of arm, assists in extension of arm from flexed position Lower subscapular nerve C5, C6 Thoracodarsal artery Teres Minor Middle half of scapula’slateral margin Lowest of 3 facets of greater tubercle of humerus Lateral rotaion of humerus; stabilizes glenohumeral joint Axillary nerve C5, C6 Scapular circumflex artery Pronator Teres Humeral head;upper portion of medial eicondyle via CFT; medial brachial intermusclar septa ulnar; coronoid process of ulna; antebrachial fascia Laterl aspect of radius at the middle of the shaft Pronates forearm Medial nerve C6, C7 Muscular branches of ulnar and radial arteries Triceps Brachii Long Head: inferior glenoid tubercle of scapula Lateral Head: upper half of posterior surface of humerus; upper half of lateral intermuscular septum Medial Head: posterior humerus Posterior surface of olecranon process of ulna; deep fascia of the antebrachium Long Head: adducts arm; extends arm at shoulder; elbow flexion Lateral Head: extends forearm at elbow Medial Head: extends forearm at elbow Radial nerve C6, C7 Muscular branches of brachial artery, superior ulnar collateral artery, profunda brachii artery Deltoid Lateral, anterior 1/3 of distal clavicle, lateral border of acromion scapular spine 9 Base of proximal phalanx of thumb Extends the proximal phalanx and 1st metacarpal of thumb Posterior interosseous nerve of radial nerve C6, C7, C8 Posterior interosseous artery Extends distal phalanx of thumb, extends proximal phalanx of thumb, assists to extend hand at wrist Posterior interosseous nerve of radial nerve C6, C7, C8 Posterior interosseous artery Extends hand at wrist Posterior interosseous nerve of radial nerve C6, C7, C8 Posterior interosseous artery Extensor Pollicis Brevis Posterior surface of radius, intrerosseous membrane, anterbrachial fascia Extensor Pollicis Longus Posterior surface of ulna, intrerosseous membrane, anterbrachial fascia Distal phalanx of thumb Extensor Carpi Ulnaris Lateral epicondyle; posterior body of ulna; antebrachial fascial Medial side of base of 5th metacarpal 10 Works Cited Mickenberg, Mike. drmikeshap.weebly.com. Web. http://www.getbodysmart.com/ap/nervoussystem/neurophysiology/menu/menu.html. Web. http://www.sumanasinc.com/webcontent/animations/content/actionpotential.html. Web. http://phet.colorado.edu/en/simulation/neuron. Web. http://www.sumanasinc.com/webcontent/animations/content/synapse.html. Web. http://msjensen.cehd.umn.edu/1135/Links/Animations/Flash/0009-swf_function_of_th.swf. Web. http://bcs.whfreeman.com/thelifewire/content/chp44/4403s.swf. Web. http://www.youtube.com/watch?v=ZscXOvDgCmQ&safety_mode=true&persist_safety_mode= 1&safe=active. Web. http://www.getbodysmart.com/ap/muscletissue/fibers/menu/menu.html. Web. http://www.sumanasinc.com/webcontent/animations/content/muscle.html. Web. http://www.youtube.com/watch?feature=fvwp&NR=1&v=NRzJjx3ANuE&safety_mode=true&p ersist_safety_mode=1&safe=active. Web. http://www.getbodysmart.com/ap/circulatorysystem/menu/menu.html. Web. 11