Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
History of invasive and interventional cardiology wikipedia , lookup
Heart failure wikipedia , lookup
Cardiothoracic surgery wikipedia , lookup
Artificial heart valve wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Remote ischemic conditioning wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Coronary artery disease wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Jatene procedure wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
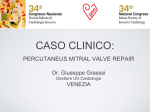
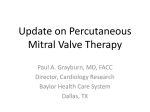
Medtech in Transition: Where are we now and what lies ahead? – State of the industry ©2017 Abbott. All rights reserved. SE2943747 Rev A. Deepak Nath, Ph.D. President, Abbott Vascular Disclosure ©2017 Abbott. All rights reserved. SE2943747 Rev A. Agenda REDUCING THE MEDICAL DEVICE “CLINICAL TRIAL BURDEN” – Least burdensome approach – Clinical trial innovation – Use of Real-World Evidence OPPORTUNITIES WITH MARKET ACCESS FOR MEDICAL DEVICES – A Paradigm Shift – Coverage with Evidence Development – Local Coverage Determinations – IDE Clinical Trial Coverage ©2017 Abbott. All rights reserved. SE2943747 Rev A. Least burdensome approach to evaluate effectiveness Excerpt from the FD&C Act (Statute 360c(a)(3)D): ii) Any clinical data, including one or more well-controlled investigations, specified in writing by the Secretary for demonstrating a reasonable assurance of device effectiveness shall be specified as result of a determination by the Secretary that such data are necessary to establish device effectiveness. The Secretary shall consider, in consultation with the applicant, the least burdensome appropriate means of evaluating device effectiveness that would have a reasonable likelihood of resulting in approval. Language demonstrates FDA’s commitment to working with the industry to reduce clinical trial burden while continuing to meet requirements for safety and effectiveness ©2017 Abbott. All rights reserved. SE2943747 Rev A. Clinical trial innovation Medical Device Innovation Consortium (MDIC) Clinical Trial Science: – Alternative, innovative trial designs – Different models of data collection that consider data at multiple points in the development of a new product – Simplification of clinical trials design FDA’s active engagement to working with stakeholders to reduce clinical trial burden while continuing to meet requirements for safety and effectiveness ©2017 Abbott. All rights reserved. SE2943747 Rev A. Use of real-world evidence to support regulatory decision-making to reduce clinical trial burden Proposed use of real-world evidence derived from real-world data (the collection and use of data generated in the postmarket setting (e.g., EHRs, registries) may: – Improve patient access to new therapies through efficient collection of data – Evaluate the “real-world” safety and/or effectiveness of products – Generate data to support coverage, reimbursement, and value analysis Alternate methods to monitor the performance of technologies reducing pre- and post-market burden for data collection ©2017 Abbott. All rights reserved. SE2943747 Rev A. Market access is no longer just about regulatory approval MARKET AUTHORIZATION /APPROVAL R&D/REGULATORY/CLINICAL Safety Efficacy ©2017 Abbott. All rights reserved. SE2943747 Rev A. Quality MARKET PLACE CHALLENGES Reimbursement/ HTA/Economic Evaluation Budgeting Protocols and Restrictions / Hospital VACs Patient Cost-Sharing Value-Based Pricing Transitioning to a value based model OLD PARADIGM Clinical innovation was sufficient for trial and increased adoption INNOVATION MODEL Innovation Safety & Efficacy Product Experience Adoption NEW PARADIGM • Decision making shifted from purely clinical decision to balance between clinical, economic value and patient value • Requires medical device manufacturers to demonstrate economic and patient value to gain access VALUE-BASED MODEL ©2017 Abbott. All rights reserved. SE2943747 Rev A. Innovation Safety & Efficacy Economic & Patient Value Market Access Abbott: Establishing value across CV portfolio • MitraClip® Transcatheter Mitral Valve Repair CardioMEMS™ Heart Failure System OPTIS™ (FFR/OCT) System 2.9 88% 73% Low Hospital Length of Stay1,2 88% of patients discharged to home1,2 73% reduction in HF hospitalization rate1,2 days COST QUALITY • 2.3 more days alive outside the hospital vs. SOC1 • Lowers patient hospitalization rates2 • $8,506 reduction in comprehensive HF care cost5 Multivessel Disease: FFR-guided PCI vs Angiography • 28% ↓ MACE1 • Saves hospitals $2,385 per case2 ©2017 Abbott. All rights reserved. SE2943747 Rev A. • 37% ↓ HF Hospitalizations1 • 58% ↓ 30-day Readmissions3 • Patient Quality of Life improvement at 6 mos1 OUTCOMES • 37% ↓ HF Hospitalizations1 • 57% ↓ Mortality over SOC Pts on GDMT managed with PA pressures4 Stable CAD: FFR-guided PCI + OMT vs. OMT Alone FFR Guidance: Intermediate, Obstructive/Significant or Indeterminate severity Lesions • 86% ↓ risk of unplanned hospitalizations for revascularization3 • FFR meets appropriate use criteria for lesion severity4 • Documented FFR may reduce exposure to audits See Important Safety Information referenced within Coverage with Evidence Development (CED): Ensure balance burden/cost with value of data • Supports coverage approach that permits access to innovative technologies while evidence is gathered in a systematic manner • CED, when integrated with FDA post-approval commitments, can be a costeffective way to gather data on real-world use • CED should be reserved for unique technologies and circumstances. When data are robust, CED may be inappropriate • A goal of any CED program should be to cover all indicated patients and expand access to new therapies For each CED consider: • Will data collected via CED be valuable for clinicians and decision makers? • Does the CED program strike the right balance between the usefulness of data vs. cost and provider burden to collect and report? ©2017 Abbott. All rights reserved. SE2943747 Rev A. Local Coverage Determination (LCD) opportunities • Most technologies are subject to the local coverage process administered by Medicare Administrative Contractors (MACs) Opportunities to improve the process: • Technologies with New Technology Add-on Payment and/or Transitional Pass-through Payment have inconsistent coverage by MACs Medicare Administrative Contractors (MAC) map of jurisdictions • Category III CPT codes receive blanket non-coverage policies. MACs need to consider available evidence when making coverage decisions • Enhance transparency and stakeholder access in coverage process ©2017 Abbott. All rights reserved. SE2943747 Rev A. Squares/rectangles indicate A/B Mac Jurisdictions that have NOT yet transitioned to A/B MACs Circles indicate A/B MAC Jurisdictions that have transitioned to A/B MACs IDE Clinical Trial Reimbursement: Positive advances in last 2 years BEFORE 2015: Coverage was not automatic or consistent BEGINNING IN 2015: Centralized Reimbursement Process • Each clinical investigator site had to notify their local Medicare contractor (MAC) of their intent to enroll Medicare patients into the clinical study and wait for approval • Medicare coverage now determined centrally based on Sponsor application; Manufacturer applies not Investigators • Submission packet had to be prepared by Each clinical investigator and submitted as far in advance of enrolling Medicare patients • Part A (Hospital claims) and Part B (Physician services) are separate and required independent contractor approval. • Process took 3 weeks to 6 months ©2017 Abbott. All rights reserved. SE2943747 Rev A. • Most patients will be covered for standard of care treatment at current payment level • Application straight forward • CMS updates list of approved trials weekly • Currently, 106 approved studies. 2 – 6 weeks. Have been up to 3months. • Uncertainty regarding early feasibility and continued access studies Expand Use of New Data Sources for Approval, Reimbursement & Post-Market Surveillance Randomized Controlled Trials • • • • • Randomized Controlled Trials Registries Real World Registries Claims Analysis Electronic Health Records Work together to determine how to utilize expanded data sources and big data to better understand new technologies and serve patients ©2017 Abbott. All rights reserved. SE2943747 Rev A. Sources for Slide 9 MitraClip® Transcatheter Mitral Valve Repair 1. MitraClip Clip Delivery System Instructions for Use 2. Lim D.S., Reynolds M.R., Feldman T., et al. Improved functional status and quality of life in prohibitive surgical risk patients with degenerative mitral regurgitation following transcatheter mitral valve repair with the MitraClip® system. J Am Coll Cardiol. 2014;64:182– 192. CardioMEMS™ Heart Failure System 1. Abraham WT, Adamson PB, Bourge RC, et al. Wireless pulmonary artery hemodynamic monitoring in chronic heart failure: A randomized controlled trial. Lancet. 2011;377(9766);658-66. 2. Adamson PB, et al. Cost Effectiveness Assessment of Pulmonary Artery Pressure Monitoring for Heart Failure Management. HRS 2015, Boston, MA. AB36-01 3. Adamson, P. B., et al. (2014). Impact of wireless pulmonary artery pressure monitoring on heart failure hospitalizations and 30-day readmissions in Medicare-eligible patients with NYHA class III heart failure: results from the CHAMPION trial. Circulation, 133, A16744 4. Abraham, W. T., et al. (2015, March). Pulmonary artery pressure management in heart failure patients with reduced ejection fraction significantly reduces heart failure hospitalizations and mortality above and beyond background guideline-directed medical therapy. Abstract 902-04 presented at ACC 2015, San Diego, CA. 5. Medicare claims analysis from June 2014 – June 2016 OPTIS™ (FFR/OCT) System 1. Tonino PA, De Bruyne B, Pijls NH, et al. Fractional flow reserve versus angiography for guiding percutaneous coronary intervention. N Engl J Med. 2009;360(3):213-24. 2. Fearon WF, Bornschein B, Tonino PA, et al. Economic evaluation of fractional flow reserve-guided percutaneous coronary intervention in patients with multivessel disease. Circulation. 2010;122(24):2545-50. 3. De Bruyne B, Pijls NH, Kalesan B, et al. Fractional flow reserve-guided PCI versus medical therapy in stable coronary disease. N Engl J Med. 2012;367(11):991-1001. 4. Patel MR, Smith PK, Spertus JA, et al. ACCF / SCAI / STS / AATS / AHA / ASNC / HFSA / SCCT 2012 Appropriate Use Criteria for coronary revascularization: Focused update. J Am Coll Cardiol. 2012;59(9):857-81. ©2017 Abbott. All rights reserved. SE2943747 Rev A. IMPORTANT SAFETY INFORMATION MITRACLIP® NT CLIP DELIVERY SYSTEM INDICATION FOR USE The MitraClip® NT Clip Delivery System is indicated for the percutaneous reduction of significant symptomatic mitral regurgitation (MR ≥ 3+) due to primary abnormality of the mitral apparatus [degenerative MR] in patients who have been determined to be at prohibitive risk for mitral valve surgery by a heart team, which includes a cardiac surgeon experienced in mitral valve surgery and a cardiologist experienced in mitral valve disease, and in whom existing comorbidities would not preclude the expected benefit from reduction of the mitral regurgitation. CONTRAINDICATIONS The MitraClip® NT Clip Delivery System is contraindicated in DMR patients with the following conditions: • Patients who cannot tolerate procedural anticoagulation or post procedural anti-platelet regimen • Active endocarditis of the mitral valve • Rheumatic mitral valve disease • Evidence of intracardiac, inferior vena cava (IVC) or femoral venous thrombus WARNINGS • DO NOT use MitraClip® NT outside of the labeled indication. Treatment of non-prohibitive risk DMR patients should be conducted in accordance with standard hospital practices for surgical repair and replacement. • MitraClip® NT is intended to reduce mitral regurgitation. The MitraClip® NT procedure is recommended to be performed when an experienced heart team has determined that reduction of MR to ≤2+ is reasonably expected following the MitraClip® NT. If MR reduction to ≤2+ is not achieved, the benefits of reduced symptoms and hospitalizations, improved quality of life, and reverse LV remodeling expected from MitraClip® NT may not occur. • The MitraClip® NT Device should be implanted with sterile techniques using fluoroscopy and echocardiography (e.g., transesophageal [TEE] and transthoracic [TTE]) in a facility with on-site cardiac surgery and immediate access to a cardiac operating room. • Read all instructions carefully. Failure to follow these instructions, warnings and precautions may lead to device damage, user injury or patient injury. Use universal precautions for biohazards and sharps while handling the MitraClip® NT System to avoid user injury. • Use of the MitraClip® NT should be restricted to those physicians trained to perform invasive endovascular and transseptal procedures and those trained in the proper use of the system. • The Clip Delivery System is provided sterile and designed for single use only. Cleaning, resterilization and/or reuse may result in infections, malfunction of the device or other serious injury or death. ©2017 Abbott. All rights reserved. SE2943747 Rev A. PRECAUTIONS • Patient Selection: – Prohibitive risk is determined by the clinical judgment of a heart team, including a cardiac surgeon experienced in mitral valve surgery and a cardiologist experienced in mitral valve disease, due to the presence of one or more of the following documented surgical risk factors: • 30-day STS predicted operative mortality risk score of – ≥8% for patients deemed likely to undergo mitral valve replacement or – ≥6% for patients deemed likely to undergo mitral valve repair • Porcelain aorta or extensively calcified ascending aorta. • Frailty (assessed by in-person cardiac surgeon consultation) • Hostile chest • Severe liver disease/cirrhosis (MELD Score >12) • Severe pulmonary hypertension (systolic pulmonary artery pressure >2/3 systemic pressure) • Unusual extenuating circumstance, such as right ventricular dysfunction with severe tricuspid regurgitation, chemotherapy for malignancy, major bleeding diathesis, immobility, AIDS, severe dementia, high risk of aspiration, internal mammary artery (IMA) at high risk of injury, etc. – Evaluable data regarding safety or effectiveness is not available for prohibitive risk DMR patients with an LVEF < 20% or an LVESD > 60mm. MitraClip® NT should be used only when criteria for clip suitability for DMR have been met. – The major clinical benefits of MitraClip® NT are reduction of MR to ≤2+ resulting in reduced hospitalizations, improved quality of life, reverse LV remodeling and symptomatic relief in patients who have no other therapeutic option. No mortality benefit following MitraClip® NT therapy has been demonstrated. • The heart team should include a cardiac surgeon experienced in mitral valve surgery and a cardiologist experienced in mitral valve disease and may also include appropriate physicians to assess the adequacy of heart failure treatment and valvular anatomy. • The heart team may determine an in-person surgical consult is needed to complete the assessment of prohibitive risk. The experienced mitral valve surgeon and heart team should take into account the outcome of this surgical consult when making the final determination of patient risk status. IMPORTANT SAFETY INFORMATION (CONTINUED) • For reasonable assurance of device effectiveness, pre-procedural evaluation of the mitral valve and underlying pathologic anatomy and procedural echocardiographic assessment are essential. • Note the “Use by” date specified on the package. • Inspect all product prior to use. Do not use if the package is open or damaged, or if product is damaged. POTENTIAL COMPLICATIONS AND ADVERSE EVENTS The following ANTICIPATED EVENTS have been identified as possible complications of the MitraClip® NT procedure. Allergic reaction (anesthetic, contrast, Heparin, nickel alloy, latex); Aneurysm or pseudo-aneurysm; Arrhythmias; Atrial fibrillation; Atrial septal defect requiring intervention; Arterio-venous fistula; Bleeding; Cardiac arrest; Cardiac perforation; Cardiac tamponade/Pericardial Effusion; Chordal entanglement/rupture; Coagulopathy; Conversion to standard valve surgery; Death; Deep venous thrombus (DVT); Dislodgement of previously implanted devices; Dizziness; Drug reaction to antiplatelet/ anticoagulation agents/contrast media; Dyskinesia; Dyspnea; Edema; Emboli (air, thrombus, MitraClip® NT Device); Emergency cardiac surgery; Endocarditis; Esophageal irritation; Esophageal perforation or stricture; Failure to deliver MitraClip® NT to the intended site; Failure to retrieve MitraClip® NT System components; Fever or hyperthermia; Gastrointestinal bleeding or infarct; Hematoma; Hemolysis; Hemorrhage requiring transfusion; Hypotension/hypertension; Infection; Injury to mitral valve complicating or preventing later surgical repair; Lymphatic complications; Mesenteric ischemia; MitraClip® NT erosion, migration or malposition; MitraClip® NT Device thrombosis; MitraClip® NT System component(s) embolization; Mitral stenosis; Mitral valve injury; Multi-system organ failure; Myocardial infarction; Nausea/ vomiting; Pain; Peripheral ischemia; Prolonged angina; Prolonged ventilation; Pulmonary congestion; Pulmonary thromboembolism; Renal insufficiency or failure; Respiratory failure/atelectasis/pneumonia; Septicemia; Shock, Anaphylactic or Cardiogenic; Single leaflet device attachment (SLDA); Skin injury or tissue changes due to exposure to ionizing radiation; Stroke or transient ischemic attack (TIA); Urinary tract infection; Vascular trauma, dissection or occlusion; Vessel spasm; Vessel perforation or laceration; Worsening heart failure; Worsening mitral regurgitation; Wound dehiscence STEERABLE GUIDE CATHETER INDICATION FOR USE The Steerable Guide Catheter is used for introducing various cardiovascular catheters into the left side of the heart through the interatrial septum. ©2017 Abbott. All rights reserved. SE2943747 Rev A. CONTRAINDICATIONS • Patients who cannot tolerate procedural anticoagulation or post procedural anti-platelet regimen • Evidence of intracardiac, inferior vena cava (IVC) or femoral venous thrombus. WARNINGS • Read all instructions carefully. Failure to follow these instructions, warning and precautions may lead to device damage, user injury or patient injury. Use universal precautions for biohazards and sharps to avoid user injury. • Use the Steerable Guide Catheter with sterile techniques using fluoroscopy and echocardiography (e.g., transesophageal [TEE] and transthoracic [TTE]) in a facility with on-site cardiac surgery and immediate access to a cardiac operating room. • The Steerable Guide Catheter is designed for single use only. Cleaning, re-sterilization and/or reuse may result in infections, malfunction of the device or other serious injury or death. • Patients with the following considerations in whom the Steerable Guide Catheter is used may have an increased risk of having a serious adverse event which may be avoided with preoperative evaluation and proper device usage. – Previous interatrial septal patch or prosthetic atrial septal defect (ASD) closure device which could result in significant difficulty in visualization or technical challenges during transseptal puncture and/or introducing the SGC into the left atrium. – Known or suspected unstable angina or myocardial infarction within the last 12 weeks could increase the procedural morbidity and mortality, due to increased hemodynamic stress secondary to general anesthesia. – Patients with active infection have an increased risk of developing an intraoperative and/or postoperative infection, such as sepsis or soft tissue abscess. – Known or suspected left atrial myxoma could result in thromboembolism and tissue injury due to difficulty with device positioning. – Recent cerebrovascular event (CVA) may increase the procedural morbidity associated with a transcatheter intervention, such as recurrent stroke. PRECAUTIONS • NOTE the “Use by” date specified on the package. • Inspect all product prior to use. Do not use if package is opened or damaged. Prior to use, please reference the Instructions for Use at www.abbottvascular.com/ifu for more information on indications, contraindications, warnings, precautions, and adverse events. IMPORTANT SAFETY INFORMATION CARDIOMEMS Brief Summary:Prior to using these devices, please review the User’s Manual for a complete listing of indications, contraindications, warnings, precautions, potential adverse events and directions for use. CAUTION:FEDERAL LAW (USA) RESTRICTS THIS DEVICE TO SALE, DISTRIBUTION AND USE BY OR ON THE ORDER OF A PHYSICIAN. INDICATIONS AND USAGE: The CardioMEMS HF System is indicated for wirelessly measuring and monitoring pulmonary artery (PA) pressure and heart rate in New York Heart Association (NYHA) Class III heart failure patients who have been hospitalized for heart failure in the previous year. The hemodynamic data are used by physicians for heart failure management and with the goal of reducing heart failure hospitalizations. CONTRAINDICATIONS: The CardioMEMS™ HF System is contraindicated for patients with an inability to take dual antiplatelet or anticoagulants for one month post implant. POTENTIAL ADVERSE EVENTS: Potential adverse events associated with the implantation procedure include, but are not limited to the following: Infection, Arrhythmias, Bleeding, Hematoma, Thrombus, Myocardial infarction, Transient ischemic attack, Stroke, Death, and Device embolization. Refer to the User’s Manual for detailed indications, contraindications, warnings, precautions and potential adverse events. ©2017 Abbott. All rights reserved. SE2943747 Rev A. IMPORTANT SAFETY INFORMATION CARDIOMEMS BRIEF SUMMARY: Prior to using these devices, please review the User’s Manual for a complete listing of indications, contraindications, warnings, precautions, potential adverse events and directions for use. CAUTION:FEDERAL LAW (USA) RESTRICTS THIS DEVICE TO SALE, DISTRIBUTION AND USE BY OR ON THE ORDER OF A PHYSICIAN. INDICATIONS AND USAGE: The CardioMEMS HF System is indicated for wirelessly measuring and monitoring pulmonary artery (PA) pressure and heart rate in New York Heart Association (NYHA) Class III heart failure patients who have been hospitalized for heart failure in the previous year. The hemodynamic data are used by physicians for heart failure management and with the goal of reducing heart failure hospitalizations. CONTRAINDICATIONS: The CardioMEMS™ HF System is contraindicated for patients with an inability to take dual antiplatelet or anticoagulants for one month post implant. POTENTIAL ADVERSE EVENTS: Potential adverse events associated with the implantation procedure include, but are not limited to the following: Infection, Arrhythmias, Bleeding, Hematoma, Thrombus, Myocardial infarction, Transient ischemic attack, Stroke, Death, and Device embolization. Refer to the User’s Manual for detailed indications, contraindications, warnings, precautions and potential adverse events. ©2017 Abbott. All rights reserved. SE2943747 Rev A. OPTIS INTEGRATED SYSTEM BRIEF SUMMARY: Please review the Instructions for Use prior to using these devices for a complete listing of indications, contraindications, warnings, precautions, potential adverse events and directions for use. Thank you Deepak Nath, Ph.D. President, Abbott Vascular Abbott Vascular 3200 Lakeside Dr., Santa Clara, CA. 95054 USA, Tel: 1.800.227.9902 Caution: This product is intended for use by or under the direction of a physician. Prior to use, reference the Instructions for Use provided inside the product carton (when available) or at www.abbottvascular.com/ifu for more detailed information on Indications, Contraindications, Warnings, Precautions and Adverse Events. Illustrations are artist’s representations only and should not be considered as engineering drawings or photographs. Photos taken by and on file at Abbott Vascular. MitraClip, CardioMEMs, and OPTIS are trademarks of the Abbott Group of Companies. www.AbbottVascular.com ©2017 Abbott. All rights reserved. SE2943747 Rev A.