Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
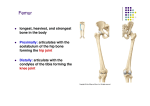
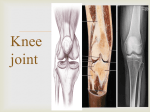
ImagIng EssEnTIals Peer reviewed Small Animal radiography Stifle Joint and CruS Danielle Mauragis, CVT, and Clifford R. Berry, DVM, Diplomate ACVR This is the fourth article in our Imaging Essentials series, which is focused on providing comprehensive information on radiography of specific areas of dogs and/or cats. The first 3 articles are available at todaysveterinarypractice.com: •Small Animal Thoracic Radiography (Sep/Oct 2011) •Small Animal Abdominal Radiography (Nov/Dec 2011) •Small Animal Pelvic Radiography (Jan/Feb 2012). Stifle RAdiogRAphy oveRview stifle radiographs are routinely needed in cases of trauma and lameness associated with common stifle joint abnormalities including: • Medialandlateralluxatingpatella • Ligamentousinstabilitysecondarytocranial cruciate injury. High-quality, correctly positioned radiographs are required in order to provide accurate assessment of the osseous and soft tissue structures of the stifle joint. This becomes even more critical when corrective osteotomies that alter joint alignment (tibial plateau leveling osteotomy or tibial tuberosity advancement) are performed. The standard of care in small animal veterinary medicine for stifle radiographic series should include straight mediolateral and caudocranial views. Following a consistent, repeatable technique for obtaining stifle radiographs helps optimize the quality of the images. T he stifle joint is one of the most common orthopedic radiographic studies. In addition to discussing new radiographic techniques for evaluation of dogs with stifle disease, this article also covers stifle anatomy, radiographic positioning, image formation, and quality control. RAdiogRAphic Stifle AnAtoMy The components of the stifle joint (Figure 1, page 54) include the: •Distalfemur •Proximaltibia •Foursesamoidbones,includingthepatella,fabellaeofthe origin of the lateral and medial gastrocnemius muscles, andfabellaoftheinsertionofthepopliteusmuscle. The patella normally articulates with the trochlear groove of the cranial distal surface of the femur. There are two femoral condyles (medial and lateral) that articulate with the medial andlateralmenisci,twoc-shapedfibrocartilagestructuresthat coverthetibialcondyleandalleviatetheincongruitybetween thetwosurfaces.Thefemoralandtibialcondylesbarelydirectly articulateinthenormalstiflebecauseofthemenisci. The fibular head forms a fibrous connective tissue joint with the proximal aspect of the lateral proximal tibia. The fibulaisalateralanatomicstructureandthetibiaislocated in a medial anatomic position. March/April 2012 Today’s Veterinary Practice 53 | small anImal PElVIc RadIogRaPHy A B Figure 1. Mediolateral (A) and caudocranial (B) radiographic images of the stifle joint of a mature dog: (A) femur; (B) tibia; (C) fibula; (D) patella; (E) fabellae of the gastrocnemius muscles; (F) fabella of the popliteus muscle withthesidetoberadiographedclosesttothetableand marked with a lead marker in the collimated area as right (R) or left (L). This radiopaque marker is placed along thecranialaspectofthelimbandshouldnotbesuperimposed over any anatomic structure (Figure 2). •The thoracic limbs should be taped together and pulled cranially to assist with restraint and ensure lateralpositionofthebody. •Placeasmallspongeunderthedorsalaspectofthepelvis to help the femoral condyles remain superimposed overeachotherintheproximaltodistaldirection. •Thepelviclimbnotbeingradiographedistapedsoitis abductedawayfromthestiflebeingradiographed.This isaccomplishedbytapingaroundthestifleandtarsus andsecuringthetapetothetable.Ifseveredegenerative joint disease of the coxofemoral joints is present, thelegmaybepulledforwardandtapedtothetable. •Asmallspongemayneedtobeplacedundertheplantar surface of the tarsus to rotate the stifle; this will assist in aligning the femoral condyles in the cranial to caudal direction. Thelateralfabella(sesamoid)oftheoriginofthehead ofthegastrocnemiusmuscleiselongatedinaproximalto distaldirectioncomparedwiththemedialfabella.Both fabellae are located at the proximal, caudal margin of the femoral condyles. The popliteal sesamoid is located along the medial Collimation aspect of the caudal •Palpate the epicondyles of the femur and place the center of the collimator light at this point. proximalmarginof •Collimatesothefieldofview(FOV)includesthedistal thetibialcondyle. thirdofthefemurandtheproximalthirdofthetibia. It is also important to include all of the soft tissues Stifle cranialtocaudaltothepelviclimbatthelevelofthe RAdiogRAphic stifle joint. expoSuRe The technique used •Caudally,itisimperativetovisualizethefascialstripe that normally runs in a proximal to distal direction for an average along the caudal aspect of the joint as well as the soft weight, medium to tissuemusculatureandpopliteallymphnode.Caudal largedogis60kVP displacementofthisfascialstripecanbeindicativeof Figure 2. A patient positioned for and 3 mAs for a lata mediolateral radiograph of the left stifle joint effusion and/or capsular thickening. eral projection and stifle joint. Note the positioning of the 66 kVP and 3 mAs •Cranially,thecollimatedFOVshouldincludetheskin sponges beneath the pelvis and the margin and the patellar ligament along the inside of for a caudal cranial tarsus to allow correct positioning theskinmargin(thinsofttissueligamentseenextendprojection, with and alignment of the femoral coning from the distal margin of the patella to the cranial the stifle placed dyles. The collimated area includes and proximal tibial tuberosity). When technique is directly on the casthe caudal and cranial skin margins correct,theskinmarginandpatellarligamentwillbe sette or detector and the distal femoral diaphysis and easily visualized along the cranial aspect of the stifle (no grid used). proximal tibial diaphysis. The limb joint (Figure 1A). not being radiographed is taped in To s et t he an abducted position. technique for a lateral projection, caudal to cranial or cranial to caudal images measure the stifle at the level of the femoral condyles in Positioning themedialtolateralplane.Forthecaudaltocranialstifle Fortheorthogonalview,thestifleshouldbeimagedina projection, measure the level of the distal femur in the caudal to cranial or cranial to caudal direction. The caucaudal to cranial plane. The cranial caudal measurement dal to cranial projection will place the stifle joint nearest will be larger than the medial lateral measurement for to the radiographic cassette or digital detector, reducing image magnification and potential geometric distortion. most dogs and cats. Averticalorhorizontalbeamradiographcanbemade; however,theabilitytotakehorizontalbeamimageswill Routine viewS of the Stifle Joint beconstrainedbythemachinebeingused.Inallcases,the Mediolateral projection radiopaqueIDmarker(RorL)shouldbeplacedalongthe Positioning Foramediolateralimageoftherightorleftstiflejoint,the lateral aspect of the stifle joint, avoiding superimposition patient is positioned on the table in lateral recumbency overanystructuresbeingradiographed. 54 Today’s Veterinary Practice March/April 2012 A B Figure 3. (A) Patient positioned for a vertical beam caudal to cranial radiograph of the left stifle joint; (B) Photograph taken from the side showing the angle of the x-ray tube head and position of the patient in sternal recumbency for the caudal to cranial radiographic projection. nial aspect of the limb and secured to allow the radiographertoleaveduringexposure. Collimation For the ventrally recumbent patient (Figure 3), palpate the femoral epicondyles at the level of the stifle joint and place the center (cross hairs) of the collimator light at this point. •CollimatesothattheFOVincludesthedistalthirdof thefemurandtheproximalthirdofthetibia. •Thex-raytubeheadshouldberotatedapproximately5 to 10 degrees caudally (angle light from caudal to cranial as seen from the dog) to prevent superimposition ofthefemurandtibiaatthelevelofthestiflejoint. •Thetubeangleisdependentonthemusclemassofthe dogwhenthelimbisinanextendedposition. For the laterally recumbent patient (Figure 4), the x-raytubeheadisrotated90degrees,positioningitpar1. Vertical Beam Positioning: Caudal to Cranial Technique allel with the tabletop and perpendicular to the pelvic •Thistechniqueworkswellforsmallerdogsandcats. limbbeingradiographed. •Thepatientcanbeplacedinventral(sternal)recum- •The x-ray beam is centered on the femoral condyles, bency with the pelvic limbs pulled caudally, placwith the horizontal line of the collimator light cross ing the affected stifle in the center of the cassette/ hairpositionedmidlinewiththefemur/tibia.Collimate detector (Figure 3A).Thepatientcanbeplacedina toincludethedistalthirdofthefemurandtheproxiV-troughtohelpkeepthethoraxandpelvisstraight. malthirdofthetibia. •The x-ray tube head is then angled toward the pes (pelviclimbdistalextremity)withthecenterofthe x-raybeamatthelevelofthejunctionbetweenthe A thigh and crural musculature (Figure 3B). •This positioning may not be possible in dogs with severe hip dysplasia, trauma, or degenerative changesofthelumbarorlumbosacralspinewithoutheavy sedation or general anesthesia. 2. Vertical Beam Positioning: Cranial to Caudal Technique NOTE: This positioning results in the greatest degree of magnification and geometric distortion due to the distance between the stifle joint and the cassette/detector. •The patient is placed in dorsal recumbency as if positioning for a pelvic ventrodorsal radiograph. Thepelviclimbsareextendedtopositionthestifle jointascloseaspossibletothetabletoporimaging cassette/digital detector. •Thex-raytubeheadisnotangled;instead,itispositioned perpendicular to the tabletop as routinely usedforverticalbeamradiography. 3. Horizontal Beam Positioning: Caudal to Cranial Technique (Figures 4A and 4B) •This technique works well for medium- to largebreeddogs. •Thepatientisplacedinlateralrecumbencywiththe stiflejointtobeimagedinanondependentposition away from the table. The affected limb is placed on sponges and pulled distally so that the limb is straight and parallel with the tabletop, being perpendicular to the pelvis. •The cassette/detector is then placed along the cra- B Figure 4. (A) Patient in lateral recumbency for a horizontal beam caudocranial radiograph of the stifle joint. Note the sponges used to keep the leg aligned with the dog’s pelvis so the stifle joint does not angle toward the table. Also note the position of the x-ray tube relative to the tabletop and the cassette. The film focal distance is maintained at 40 inches; (B) Photograph from the end of the table showing the pelvic limb across the digital detector. March/April 2012 Today’s Veterinary Practice 55 small animal Radiography: The stifle Joint and crus ImagIng EssEnTIals | | small anImal PElVIc RadIogRaPHy QuAlity contRol •Distalthirdofthefemur Forqualitycontrolofanydiagnosticimage,remember •Proximalthirdofthetibia the following 3-step approach: •Patellaandothersesamoidbones 1. Is the technique appropriate? •Softtissues,includingthemusculatureandpopli All bones should be sharply margined and clearly teal lymph node along with the cranial and caudal visualized. Enough x-ray penetration should be skin margins. present to clearly expose the normal cancellous 3. Is the positioning lateral and straight? (intramedullary) bone pattern of the distal femur •In a straight mediolateral image, the femoral and proximal tibia. However, the exposure should condyles should be superimposed over each notbesogreatthatthesofttissuesareoverexposed otherandthefibularheadshouldbeinacaudal andnotvisualizedinthefinalimage. positionalongtheproximalportionofthetibial 2. Is the appropriate anatomy present within the condyle. image? •Onthecaudocranialimage,thepatellashouldbe Giventhatthedesiredtechniquehasbeenattained, inacentralposition,withnooverlapbetweenthe make sure that the appropriate anatomy is included. femoralcondylesandthetibialcondyle. The lateral and caudal cranial projections should •Thefemoralcondylesshouldbeequalinsizeand include the: shape. RAdiogRAphic viewS foR Specific oRthopedic SuRgicAl pRoceduReS: preoperative, postoperative, & follow-up Studies tibial plateau leveling osteotomy Thetibialplateaulevelingosteotomy(TPLO)lateral is a special projection. Its purpose is to position the proximaltibiawheretheproximaltibialjointsurface is highlighted. This allows the surgeon to consistently and repeatedly determine joint orientation in order toquantitatethetibialslope.Thisassessmentisthen usedtoplantheosteotomythatwillbeperformed during surgery (Figure 5). Mediolateral Projection • Themediolateral projection includes thecrus(tibiaand fibula)fromthe stifle joint (distal femoral diaphysis) distaltotheproximal metatarsus. Boththestifle and tarsal joints areflexedata 90-degreeangle. •Thecenterofthe collimator light shouldbeplaced just distal to the center of the stifle joint(proximal third). This will allow medial and lateraltibialcondyle margin imposition. 56 A •Theintercondylareminencesneedtobesuperimposedinproximaltodistalandcranialtocaudal directions. •However,duetotheanatomyofthefemurinsome dogs,theintercondylareminencesmaybesuperimposedwhilethefemoralcondylesarenot.Forthe purpose of surgical measurements, it is more important for this view to have the intercondylar eminences superimposed rather than the femoral condyles. Caudocranial Projection •Thecaudocranialprojectionshouldincludethe distalfemur,entirestiflejoint,andcrusandextend distaltotheleveloftheproximalmetatarsi. B c d Figure 5. (A) Lateral positioning of the patient for a TPLO lateral radiograph. In this image, the dog has been placed in a similar position as seen in Figure 2A; however, the stifle and tarsal joints are flexed at 90 degrees. (B) Pre-operative, postoperative, and (C) mediolateral radiographs from a dog that has had a TPLO. The arrow in B points to the superimposed intercondylar eminences. (D) Pre-operative caudocranial image of the stifle joint and crus. In this dog there is central positioning of the patella (seen superimposed over the distal femur) as well as central positioning of the medial cortex of the distal tibial intermediate ridge or cochlea. The arrow points to the medial cortex of the calcaneous. Today’s Veterinary Practice March/April 2012 A and the stifle joint angle at a 135-degree angle. B Figure 6. (A) Lateral positioning of a patient with external goniometer for a TTA pre-operative radiograph; (B) mediolateral radiographic image of a correctly positioned limb following a TTA procedure. •Thefemoralcondylesshouldappearequalin sizeontheimage. •Thepatellashouldbesuperimposedcentrally betweenthefemoralcondylesandatamid position relative to the femoral condyles. This maynotbethecaseifthedoghaspatellar luxation(Figure 1). tibial tuberosity Advancement Thetibialtuberosityadvancement(TTA)procedure is also used for the surgical repair of cranial cruciate ligament rupture. The mediolateral radiograph projection for the TTA differs from theTPLOmediolateralprojectioninthatthe femurandtibiaarenotflexedbutremainina morenaturalextendedposition(Figure 6). Positioning •CorrectpositioningfortheTTAimagewillbe determinedbystiflejointlateralityandangleof thefemurandtibia. •Thefemoralcondylesshouldbesuperimposed as with a mediolateral stifle view. •Usinganexternallyplacedgoniometer,the stifle joint angle should measure 135 degrees (Figure 6). Specific Projections •Thecaudocranial TTA projection should includethedistalfemurthroughtheproximal metatarsalbones.Thepatellashouldbesuperimposedcentrallybetweenthefemoralcondyles,whicharenormallyequalinsize. •Forthelateral TTA projection, the center of collimatorlightshouldbeatthecenterofthe stiflejoint,withtheFOVopenedtoinclude asmuchofthefemurandtibiaaspossible Skyline of the patella The skyline patella radiographicprojectionisusedtobetter visualizethepatellaandtrochlear groove (Figure 7). This view is typically used in cases ofmedialorlateralluxating patella. As with the caudocranial view of the stifle, there are two approaches to positioning basedonahorizontalorverticalpositionofthex-raytube. Vertical Beam/X-Ray Tube Radiograph Positioning: •Thepatientispositionedinventralrecumbency withtheaffectedlimbflexedandpushedcranial and lateral. •Thetibiaispositionedunderthefemurwith the affected stifle centered in the middle of the cassette/detector. •Aspongeisplacedbetweenthebodywalland femur to help push the stifle joint away from thebody. A B Figure 7. (A) Vertical positioning of a patient to image the patella in a cranioproximal to craniodistal oblique of the patella and trochlear groove of the distal femur; (B) Correctly positioned skyline radiograph to evaluate the patella and trochlear groove. March/April 2012 Today’s Veterinary Practice 57 small animal Radiography: The stifle Joint and crus ImagIng EssEnTIals | | small anImal PElVIc RadIogRaPHy •Thepatientcanbeplacedinav-troughforstabilityandtohelpkeepthethoraxstraight. Collimation: •Withthepatientinventralrecumbencyandthe stiflejointflexed,palpatethedistalfemurand patella. •Thecenterofthecollimatorlightispositioned atthislevel(distalfemur).TheFOVshould include the distal portion of the femur. •Ifpossible,thex-raytubeshouldberotated approximately5degreescranial(towardtheanimal’s head) to prevent superimposition of the patella,femur,andtibia.Thisviewwouldthen betermedacranioproximal to craniodistal oblique projection of the patella or distal femur. FoV = field of view; TPlo = tibial plateau leveling osteotomy; TTa = tibial tuberosity advancement Suggested Reading Burk rl, feeney dA. Small Animal Radiology and Ultrasonography: A Diagnostic Atlas and Text, 3rd ed. Philadelphia: Saunders elsevier, 2003. dismukes di, tomlinson Jl, fox dB, et al. radiographic measurement of canine tibial angles in the sagittal plane. Vet Surg 2008, 37: 300-305. dismukes di, tomlinson Jl, fox dB, et al. radiographic measurement of the proximal and distal mechanical joint angles in the canine tibia. Vet Surg 2007; 36:699-704. Keely JK, McAllister H, Graham JP. Diagnostic Radiology and Ultrasonography of the Dog and Cat, 5th ed. Philadelphia: Saunders elsevier, 2011. lambert rJ, wendelburg Kl. determination of the mechanical medial proximal tibial angle using a tangential radiographic technique. Vet Surg 2010; 39:181-186. Sirois M, Anthony e, Mauragis d. Handbook of Radiographic Positioning for Veterinary Technicians. Clifton Park, nY: delmar Cengage learning, 2010. thrall de (ed). Textbook of Veterinary Radiology, 5th ed. Philadelphia: Saunders elsevier, 2008. thrall de, robertson id. Atlas of Normal Radiographic Anatomy and Anatomic Variants in the Dog and Cat. Philadelphia: elsevier Saunders, 2011. SedAtion & AnAlgeSiA although not required, sedation is recommended for any orthopedic radiographic study as it allows the patienttorelax,therebyallowingeasierpositioning (particularlyextensionforcranialcaudalimages).In addition, sedation also decreases the amount of time required for repositioning due to lack of patient cooperation. For animals with painful joints, a neuroleptanalgesic protocol provides both sedation and pain control. Horizontal Beam/X-Ray Tube Radiograph Positioning: •Thepatientispositionedindorsalrecumbency usingaV-trough;thepelviclimbsareflexed. •Thex-raytubeisrotated90degreesandplaced inahorizontalposition,situatingthepatella perpendiculartothecassetteandx-raytube head. •Asandbagisplacedoverthetarsusandpesfor stabilization. •Thecassette/detectoristhenplacedonthe abdomenjustcranialtothestiflesandsecured forexposure. Collimation: •Withthepatientindorsalrecumbency,thetube headisrotated90degreestowardtheaffectedlimb. •Thecenterofthebeamisfocusedatthepatellar level. The patella with a small portion of the femurshouldbeincluded. Duetovaryingthicknessofthelimb,keepthe collimationoftheskylineFOVofthepatellatoas smallanareaaspossible,whichreducessecondary radiation. ■ 58 Today’s Veterinary Practice March/April 2012 Danielle Mauragis, CVT, is a radiology technician at University of Florida College of Veterinary Medicine. She teaches veterinary students all aspects of the physics of diagnostic imaging, quality control of radiographs, positioning of small and large animals, and radiation safety. Ms. Mauragis coauthored the Handbook of Radiographic Positioning for Veterinary Technicians (2009) and was the recipient of the Florida Veterinary Medical Association’s 2011 Certified Veterinary Technician of the Year Award. This award recognizes an individual for the many outstanding contributions that person has made to the overall success of the veterinary practice operated or staffed by an FVMA member veterinarian. Clifford R. Berry, DVM, Diplomate ACVR, is a professor in diagnostic imaging at the University of Florida College of Veterinary Medicine. His research interests include cross-sectional imaging of the thorax, nuclear medicine applications in veterinary medicine, and biomedical applications of imaging in human and veterinary medicine. Dr. Berry has been a faculty member at North Carolina State University and University of Missouri. He received his DVM from University of Florida and completed a radiology residency at University of California–Davis.