Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Heart failure wikipedia , lookup
Electrocardiography wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Aortic stenosis wikipedia , lookup
Jatene procedure wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Ventricular fibrillation wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
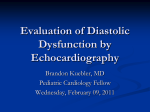
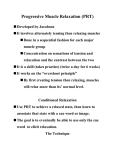
Am J Physiol Heart Circ Physiol 281: H2002–H2009, 2001. MRI assessment of LV relaxation by untwisting rate: a new isovolumic phase measure of SHENG-JING DONG, PAUL S. HEES, CYNTHIA O. SIU, JAMES L. WEISS, AND EDWARD P. SHAPIRO Division of Cardiology, Johns Hopkins University School of Medicine, Baltimore, Maryland 21224 Received 7 December 2000; accepted in final form 18 July 2001 Dong, Sheng-Jing, Paul S. Hees, Cynthia O. Siu, James L. Weiss, and Edward P. Shapiro. MRI assessment of LV relaxation by untwisting rate: a new isovolumic phase measure of . Am J Physiol Heart Circ Physiol 281: H2002–H2009, 2001.—Most noninvasive measures of diastolic function are made during left ventricular (LV) filling and are therefore subject to “pseudonormalization,” because variation in left atrial (LA) pressure may confound the estimation of relaxation rate. Counterclockwise twist of the LV develops during ejection, but untwisting occurs rapidly during isovolumic relaxation, before mitral opening. We hypothesized that the rate of untwisting might reflect the process of relaxation independent of LA pressure. Recoil rate (RR), the velocity of LV untwisting, was measured by tagged magnetic resonance imaging and regressed against the relaxation time constant (), recorded by catheterization, in 10 dogs at baseline and after dobutamine, saline, esmolol, and methoxamine treatment. RR correlated closely (average r ⫽ ⫺0.86) with and was unaffected by elevated LA pressure. Multiple regression showed that , but not LA or aortic pressure, was an independent predictor of RR (P ⬍ 0.0001, P ⫽ 0.99, and P ⫽ 0.18, respectively). The rate of recoil of torsion, determined wholly noninvasively, provides an isovolumic phase, preloadindependent assessment of LV relaxation. Use of this novel parameter should allow the detailed study of diastolic function in states known to affect filling rates, such as aging, hypertension, and congestive heart failure. diastole; hemodynamics; magnetic resonance imaging; imaging (LV) relaxation is difficult to assess by noninvasive means, because imaging methods cannot directly measure cavity pressure. Echocardiographic, Doppler, and radionuclide parameters of diastolic function are derived from rates of inflow of blood or outward movement of the myocardium. However, the process of relaxation occurs mostly during the diastolic isovolumic period of the cardiac cycle, before blood flow or wall motion begins. Indexes measured later in the cycle examine only the final stages of relaxation (33). Furthermore, these parameters are subject to “pseudonormalization,” because variation in left atrial (LA) pressure profoundly affects filling dynamics and thus confounds attempts to indirectly estimate the relaxation rate (22, 31, 40, 41). New echocardiographic LEFT VENTRICULAR Address for reprint requests and other correspondence: E. P. Shapiro, Div. of Cardiology, Johns Hopkins Univ. School of Medicine, 4940 Eastern Ave., Baltimore, MD 21224 (E-mail: [email protected]). H2002 methods that are less sensitive to LA pressure (7, 16, 21, 39) or “adjust” for an estimated LA pressure (2, 3, 24, 37) are in clinical use, but novel noninvasive ways of directly assessing relaxation are needed. LV torsion is the wringing motion, or twist, of the heart imparted by contraction of its obliquely spiralling fibers. Counterclockwise torsion develops during ejection, but the clockwise recoil of torsion, or untwisting, is a deformation that occurs largely during isovolumic relaxation, before mitral valve opening (6, 10, 23, 29, 34, 46). This recoil is associated with the release of restoring forces that had been accumulated during systole and is thought to contribute to diastolic suction (17, 29, 34, 46). The extent of torsion is correlated with cavity pressure (14), and its recoil rate (RR) may thereby be related to the rate of pressure fall. This deformation can be quantified using magnetic resonance imaging (MRI) with tagging, a noninvasive method for marking and tracking specific myocardial sites (5, 47). In this study, we explored the relationship between the rate of untwisting (RR) and the relaxation time constant () using various interventions to alter in intact canine hearts. The influence of LA pressure on RR was assessed. The strength of the relationship between and RR was compared with that between and isovolumic relaxation time (IVRT), a standard index of relaxation that is known to be highly sensitive to preload. We suggest that RR may provide a new isovolumic phase measure of relaxation that is preload independent and can be determined noninvasively. METHODS Terminology. In this paper, the term “LV relaxation” refers to the time course of LV pressure decline, a process that depends on both deactivation of actin-myosin cross-bridges and the release of restoring forces due to chamber and myocardial deformation (45). The term “preload” refers to LA pressure, which constitutes the preload to ventricular filling. Animal preparation. Ten adult mongrel dogs (9 males and 1 female, weighing 24 ⫾ 3 kg) were anesthetized with intravenous pentobarbital sodium (25–35 mg/kg). After intubation, the dogs were mechanically ventilated (model 613, Harvard Apparatus). The left jugular vein was cannulated for fluid and drug administration, and the right jugular vein was The costs of publication of this article were defrayed in part by the payment of page charges. The article must therefore be hereby marked ‘‘advertisement’’ in accordance with 18 U.S.C. Section 1734 solely to indicate this fact. 0363-6135/01 $5.00 Copyright © 2001 the American Physiological Society http://www.ajpheart.org ASSESSMENT OF RELAXATION BY LV RECOIL cannulated for placement of a right atrial pacing lead. Each dog was instrumented with magnetic-compatible micromanometer-tipped catheters (Millar Instruments) to measure LA, LV, and aortic pressures as follows. A left thoracotomy was performed, and a small transverse incision (⬃3 cm) was made at the ventrolateral pericardium along the base of the heart for the placement of a LA catheter through the LA appendage with a purse-string suture. A LV catheter was placed through cannulation of the left internal carotid artery. An aortic catheter was inserted through cannulation of the left femoral artery. After surgical preparation, the animal was allowed to stabilize for 30 min. Throughout the experiments, body temperature was maintained by a heating pad, the chest was left open, and the electrocardiogram (lead II) was monitored and also used as a trigger for MRI. At the end of experiment, the animal was euthanized using intravenous KCl. If hemodynamic instability or arrhythmias precluding further MRI developed, the protocol was terminated without additional interventions. All procedures were approved by the institutional Animal Care and Use Committee. Experimental protocol. Interventions were planned with the main goal of recording hemodynamic and MRI data (during steady-state conditions) over a wide range of values of and with variations of LA and aortic pressures. The conditions studied were as follows: 1) first baseline, 2) dobutamine infusion, 3) dobutamine infusion plus volume loading, 4) second baseline (stopping dobutamine infusion), 5) esmolol infusion, 6) third baseline (stopping esmolol infusion), and 7) methoxamine infusion. Dobutamine (Eli Lilly) was diluted (250 mg in 500 ml saline) and infused to increase systolic LV pressure by at least 15%. Volume load was performed by infusing saline at 10–12 ml/kg body wt (range, 200–300 ml) in each individual experiment. Esmolol (Ohmeda) was diluted (2,500 mg in 500 ml saline) and infused to decrease systolic LV pressure by at least 15%. Methoxamine (Burroughs-Wellcome) was diluted (20 mg in 500 ml saline) and infused to increase systolic LV pressure by at least 15%. Solutions were mixed immediately before infusion. After stabilization of each condition, hemodynamic and MRI data were acquired. Hemodynamic analysis. All signals were amplified (Gould Instrument) and digitized at sampling frequencies of 250 Hz for 5 s under each condition. was calculated by measuring LV pressure every 4 ms from the point of the minimal instantaneous rate of change of LV pressure with respect to time (dP/dt) until its upturn and fitting the curve to the following equation: p(t) ⫽ p0e⫺t/ ⫹ p⬁ (20), where p is pressure, p0 is pressure at minimal dP/dt, t is time thereafter, p⬁ represents the pressure asymptote. IVRT was measured from the LA, LV, and aortic pressures as the interval from the crossover of the LV and aortic pressures to the crossover of the LV and LA pressures. MRI image acquisition. Myocardial tagging was used in these experiments to measure torsion and its rate of recoil. Tags are noninvasive markers that are imprinted on the myocardium by selective radiofrequency saturation of planes perpendicular to the imaging planes; they change the magnetization of the protons in the tagged plane compared with the neighboring nontagged regions, resulting in a difference in signal intensity. When placed at end diastole and then imaged throughout the cardiac cycle, tags reveal the deformation and displacement of the myocardium on which they are placed (Fig. 1). Tags may be positioned in a radial pattern (47), which is ideal for the measurement of torsion, or in a Fig. 1. Magnetic resonance basal and apical short-axis images of a canine heart, with radial tags at end diastole, end ejection, and mitral valve opening. At end ejection, there has been rotation of the cardiac portion of the tags (particularly at the apex), which are no longer continuous with the portions that pass through nonmoving structures such as the chest wall. Arrows mark the initial positions of two tags. Note that the cavity is smaller at end ejection. By the end of isovolumic relaxation, tags have recoiled almost completely to their starting position despite the fact that cavity size is unchanged and filling has not yet begun. The measurement of torsion is derived from the difference in tag position between basal and apical slices. Torsion is counterclockwise when viewed from apex to base but appears clockwise when viewed from base to apex (as shown here). This figure illustrates the concept that recoil is largely an isovolumic event. AJP-Heart Circ Physiol • VOL H2003 281 • NOVEMBER 2001 • www.ajpheart.org H2004 ASSESSMENT OF RELAXATION BY LV RECOIL grid pattern (5), which is commonly used for calculation of a full strain field. Tagged MRI was performed on a Resonex 0.38-T iron-core resistive magnet (Sunnyvale, CA). The image acquisition technique used in these experiments was similar to that reported in detail in previous studies from this laboratory and others (5, 9, 14, 34, 47). Briefly, image acquisition includes a gradient echo sequence modified to include tissue tagging, with temporal resolution of 16 ms, time to echo of 10 ms, and time to repeat of two R-R intervals, 128 phase- and 256 frequency-encoding steps, two averages of excitation, and field of view of 20–25 cm. After serial scout images, two (basal and apical) short-axis images, 3.0 cm apart, with eight radial tags perpendicular to the image planes were acquired (14). Tagging and imaging were triggered by the R wave of the electrocardiogram: tags were placed at end diastole, and 19–22 images were acquired thereafter. The image slice thickness was 1.0 cm and tag thickness was 0.3 cm. Heart rate was kept constant by pacing at the right atrium (mean heart rate was 159 ⫾ 7 beats/min). MRI image analysis. The digital MRI data were processed using a special software package (Cardiology Image Processing System, Johns Hopkins University). The tag-endocardium intersection points on both basal and apical short-axis images were identified manually and digitized (8 points/ slice). Torsion at each tag-endocardium intersection point was calculated as an angle between the tag line of the apical slice and the projection of the basal tag line on the apical slice at end systole, as previously reported (Fig. 2) (9, 14). With the use of this method, clockwise rotation of the base and counterclockwise rotation of the apex are combined to yield a measure of the total base-to-apex deformation. Mean torsion was then calculated as the average of eight values for the eight tag-endocardial intersection points. Recoil, the directional reversal of systolic counterclockwise torsion during diastole, was expressed as the percentage of maximum systolic torsion: recoil ⫽ Tort/Tormax ⫻ 100, where Tort is torsion at time t and Tormax is the maximum systolic torsion. [Normalization to maximum torsion was performed as the primary analysis here because , the gold standard for relaxation, is based on the time required for a percentage of pressure fall (1/eth) rather than an absolute pressure drop in mmHg. However, analyses were repeated using the nonnormalized torsion values.] RR was defined as the slope of the linear regression of recoil versus time, which is similar to the method used by DeAnda et al. (13), during the first 64 ms after peak torsion (i.e., using data from five images). Statistical analysis. The overall effect of each intervention (dobutamine, volume, esmolol, and methoxamine) on hemodynamic and MRI parameters was assessed by paired t-tests. A value of P ⬍ 0.05 was considered statistically significant. The relationships between and RR, and likewise between and IVRT, were initially explored by simple linear regression analysis. In each individual animal, correlations (r and r2) were determined for both relationships. To compare the significance of these two relationships (-RR vs. -IVRT), paired t-tests were applied based on the derived r2 for each relationship; to compare the consistency of the two relationships, the test for correlated variances was applied to SD2 (38). Overall correlations of and RR, and of and IVRT, were derived using linear regression analysis adjusting for effects in individual dogs (20). Finally, multiple regression analysis was performed to determine the significance of the -RR and -IVRT relationships in the presence of other hemodynamic variables and to test whether the other variables were independent determiAJP-Heart Circ Physiol • VOL Fig. 2. Measurement of the angle of torsion from tagged images. Tags are placed at end diastole, intersecting the base at point a and the apex at point b. By end ejection, there has been clockwise rotation of the basal tag to point c and counterclockwise rotation of the apical tag to point d. Systolic torsion is the angle () between the apical tag position (point d) and the basal tag position (reflected onto the apex as point e). Torsion therefore combines the opposite rotations of base and apex into a single deformation. Arrows show the direction of torsion and recoil. nants of RR and IVRT using the Generalized Estimating Equation (GEE) method for repeated-measures data (25). The independent, or explanatory, variables in the GEE model included LA pressure, aortic pressure, LV systolic pressure, , and peak ⫹dP/dt. The dependent variables were RR for the -RR relationship and IVRT for the -IVRT relationship. The correlations among the repeated observations for individual dogs were modeled as exchangeable correlations. A value of P ⬍ 0.05 was considered statistically significant. These analyses were all repeated for the non-normalized RR. RESULTS Effects of interventions. Ten dogs were instrumented and studied. All 10 dogs had hemodynamic and MRI measurements at first baseline, during dobutamine infusion, and after volume loading. Seven dogs had additional measurements at second baseline and during esmolol infusion, and four dogs had additional measurements made at third baseline and during methoxamine infusion. The average effects of catecholamine stimulation, volume infusion, -blockade, and increased afterload on the variables of interest are detailed in Table 1. Of note, the predominant effect of dobutamine was a re- 281 • NOVEMBER 2001 • www.ajpheart.org H2005 ASSESSMENT OF RELAXATION BY LV RECOIL Table 1. Effects of interventions on hemodynamic and imaging parameters First baseline Dobutamine Dobutamine ⫹ volume Second baseline Esmolol Third baseline Methoxamine LA Pressure, mmHg Aortic Pressure, mmHg , ms IVRT, ms Torsion, ° RR, %/ms 9.8 ⫾ 14 9.0 ⫾ 9.5 14.6 ⫾ 4.9‡ 16.7 ⫾ 7.5 22.2 ⫾ 9.0 20.3 ⫾ 4.3 34.8 ⫾ 9.9* 81.1 ⫾ 21 93.3 ⫾ 4.5* 103.2 ⫾ 22* 93.6 ⫾ 18 77.4 ⫾ 17† 83.1 ⫾ 21 123.2 ⫾ 19‡ 34.0 ⫾ 7.3 27.2 ⫾ 8.2‡ 24.0 ⫾ 5.9* 35.1 ⫾ 5.8 37.9 ⫾ 7.8 37.0 ⫾ 6.7 47.3 ⫾ 4.6* 70 ⫾ 13 59 ⫾ 14‡ 49 ⫾ 11‡ 67 ⫾ 9.7 69 ⫾ 15 58 ⫾ 6.0 68 ⫾ 6.0 14.7 ⫾ 7.4 19.9 ⫾ 4.9 16.0 ⫾ 4.8† 13.0 ⫾ 4.2 7.1 ⫾ 4.6* 11 ⫾ 5.3 8.1 ⫾ 4.8* 0.69 ⫾ 0.33 0.81 ⫾ 0.33* 0.81 ⫾ 0.30 0.67 ⫾ 0.30 0.62 ⫾ 0.22 0.52 ⫾ 0.18 0.36 ⫾ 0.09 Values are means ⫾ SD. LA, left atrial; , relaxation time constant; IVRT, isovolumic relaxation time; RR, recoil rate. The following conditions were studied: 1) first baseline, 2) dobutamine infusion, 3) dobutamine infusion ⫹ volume loading (dobutamine ⫹ volume), 4) second baseline (stopping dobutamine infusion), 5) esmolol infusion, 6) third baseline (stopping esmolol infusion), and 7) methoxamine infusion. For dobutamine, esmolol, and methoxamine effects, comparisons are made with the respective baselines. For volume effect, dobutamine ⫹ volume is compared with dobutamine alone. * P ⬍ 0.05; † P ⬍ 0.01; ‡ P ⬍ 0.001. duction in (from 34 to 27 ms, P ⫽ 0.0007); there was a concomitant increase in RR (from 0.69 to 0.81 %/ms, P ⫽ 0.02), and IVRT shortened. The predominant effect of volume infusion was an increase in LA pressure (from 9.0 to 14.6 mmHg, P ⫽ 0.0001); RR was unchanged, whereas IVRT shortened significantly. Esmolol reduced aortic pressure without having a significant effect on , RR, or IVRT. Methoxamine greatly increased LA and aortic pressures and caused to increase, but did not significantly change RR or IVRT. The average time to peak torsion was at 200 ⫾ 29 ms after the R wave, whereas end systole occurred at 227 ⫾ 30 ms after the R wave, that is, recoil began 27 ms before aortic valve closure. Our measurement of RR spanned 64 ms and was completed before the end of isovolumic relaxation during all interventions. Correlation of and RR. The correlations of RR with in each individual dog for which at least five measurements were available (7 of 10 dogs) are detailed in Table 2. For comparison purposes, the correlations of IVRT with are also shown. The -RR correlations are high in each individual animal studied, with an average r of ⫺0.86 (ranging from ⫺0.77 to ⫺0.93) and with similar slopes. The -IVRT relationships have less consistent slopes and lower r2 values. The correlation of RR with is significantly better (P ⫽ 0.026 based on r2) and less variable (P ⬍ 0.001 based on SD2) than the correlation of IVRT with . The relation between RR and is plotted in Fig. 3. When data from all 10 dogs were pooled and adjusted for individual dog effects using an indicator variable, r was 0.92 and r2 was 0.85, with P ⬍ 0.0001. The relation between and IVRT was also significant, with r ⫽ 0.81, r2 ⫽ 0.65, and P ⬍ 0.0001. Multiple regression of hemodynamic parameters against RR and against IVRT. Multiple regression using GEE was performed to assess the correlation of individual hemodynamic parameters with RR and IVRT, accounting for the potential confounding effect of other variables (Table 3). was the only independent predictor of RR (P ⬍ 0.0001); there was no independent relation between RR and LA pressure (P ⫽ 0.817), aortic notch pressure (P ⫽ 0.287), LV peak systolic pressure (P ⫽ 0.604), or peak ⫹dP/dt (P ⫽ 0.060). In contrast, IVRT was closely related to LA pressure (P ⬍ 0.0001) and aortic pressure (P ⫽ 0.015) as well as to (P ⬍ 0.0001). When the RR based on nonnormalized values of torsion (expressed as °/ms rather than %/ms) was used in these analyses, the results were similar with respect to average effects of interventions and linear regressions. Multivariate regression by GEE also showed a close independent relation between and absolute RR (P ⫽ 0.004, coefficient ⫽ ⫺0.0273). There was a weak but significant relation between LA pressure and absolute RR (P ⫽ 0.02, coefficient ⫽ ⫺0.0001), probably due to the preload dependence of absolute values of torsion (14). The nonnormalized RR at baseline was 0.084 ⫾ 0.038 (SD) °/ms. Table 2. Linear regression of against RR and IVRT in individual experiments Versus RR Dog 1 Dog 2 Dog 3 Dog 4 Dog 5 Dog 6 Dog 7 mean SD Versus IVRT slope SEE r r2 ⫺38.8 ⫺54.1 ⫺41.4 ⫺20.0 ⫺41.1 ⫺42.3 ⫺48.3 ⫺40.9 10.6 15.1 14.4 12.7 5.5 15.1 9.4 8.5 11.5 3.77 ⫺0.83 ⫺0.91 ⫺0.82 ⫺0.85 ⫺0.77 ⫺0.93 ⫺0.93 ⫺0.86 0.06 0.69 0.82 0.68 0.72 0.60 0.87 0.86 0.75 0.10 slope SEE r r2 ⫺0.20 0.43 0.36 0.88 0.70 0.49 0.48 0.45 0.34 0.32 0.14 0.21 0.39 0.37 0.61 0.23 0.32 0.16 ⫺0.35 0.87 0.60 0.71 0.65 0.98 0.67 0.59 0.44 0.12 0.76 0.36 0.50 0.42 0.96 0.45 0.51 0.27 IVRT and were measured in milliseconds and RR was measured in percentages per millisecond. SEE, standard error of the estimate. AJP-Heart Circ Physiol • VOL 281 • NOVEMBER 2001 • www.ajpheart.org H2006 ASSESSMENT OF RELAXATION BY LV RECOIL Fig. 3. Correlation of the relaxation time constant () with recoil rate in 10 dogs. Symbols are different for each of the 10 dogs. Each individual point represents one intervention. DISCUSSION LV relaxation begins when myofiber tension starts to decline during late ejection (8), proceeds rapidly as pressure falls during isovolumic relaxation, and continues through the period of early filling. Relaxation is best quantified by measuring the rate of LV pressure decay, which can be expressed as a time constant (), based either on a monexponential model with a zero (44) or nonzero asymptote (30) or on a “logistic” model (27). The greatest portion of the pressure decline occurs during isovolumic relaxation. The process of LV filling, which begins at the time of mitral valve opening, profoundly alters the rate of LV pressure decline; pressure changes that occur after mitral valve opening do not reliably reflect the process of relaxation itself (15, 30). Noninvasive methods can detect the extent and velocity of motion of the myocardium or blood. However, standard measurements provide little information about the isovolumic period (other than its duration), during which most of the relaxation process occurs (19), because deformations that are routinely studied (e.g., myocardial lengthening or thinning, cavity volume increase, and blood inflow) are dependent on changes in LV volume. These deformations do not begin until after the mitral valve opens, when most of the relaxation process has already been completed. Like invasive measurement of pressure, these noninvasive parameters tend to be strongly influenced by factors other than relaxation that contribute to the early diastolic atrioventricular pressure gradient [i.e., LA pressure, passive myocardial stiffness (4), and viscoelasticity (15)]. Torsion mechanics. Torsion and its diastolic recoil display a unique behavior that is, in part, volume independent and therefore can be observed during the isovolumic periods. With the use of implanted markers (6, 29, 46), MRI tagging (34), and guidewire rotation during angioplasty (23), it has been clearly shown that during isovolumic relaxation, when cavity volume is fixed, there is a rapid recoil of ⬃40% of the torsion that had accumulated during systole. In addition, volume independence has been shown in a completely isovolumic beating heart preparation, in which there is conAJP-Heart Circ Physiol • VOL siderable torsion and recoil, despite the absence of thickening or circumferential or longitudinal shortening (26). Therefore, in contradistinction to other noninvasive indexes of diastolic function, recoil of torsion is largely an isovolumic event, as is the gold standard for relaxation, . Recently, Dong et al. (14) found that during conditions of fixed cavity volume in an isolated perfused heart model, the extent of torsion depended on cavity pressure. We therefore hypothesized that the rate of recoil might reflect the rate of pressure fall during isovolumic relaxation and that its measurement might provide a more physiological and direct noninvasive method for quantification of relaxation than has heretofore been available. In this study, RR was indeed found to correlate closely and reproducibly with . This finding is consistent with prior studies of torsion during diastole in humans. Moon et al. (29) altered load and contractility in transplant recipients with radiopaque markers and reported a close relationship of early diastolic untwist with both peak ⫺dP/dt and LV end-systolic volume, both of which are closely related to . Yun et al. (46) noted that early diastolic rapid recoil was markedly diminished during cardiac transplant rejection, which would be expected to slow relaxation: the time to 50% of peak twist was prolonged by 40%. This phenomenon was a sensitive predictor of rejection. Knudtson et al. (23) found that, whereas recoil of the apex was 37% complete by the end of isovolumic relaxation in nonischemic human hearts, recoil during isovolumic relaxation was essentially absent during acute ischemia induced by angioplasty balloon inflation, a condition known to prolong . Studies in dogs have been less consistent. Rademakers et al. (34) reported that inotropic stimulation caused an increase in the extent of recoil during isovolumic relaxation, whereas Gibbons Kroeker et al. (18) reported a decrease, but was not measured in those studies. Mechanistic significance of recoil. In addition to providing a means to measure the rate of LV pressure fall, the untwisting deformation may itself contribute to the pressure decay. Relaxation is dependent on the rate of deactivation of cross-bridges within the sarcomere but is also associated with the release of restoring forces Table 3. Results of multiple regression using the GEE method, showing the relation of independent variables with RR and with IVRT, controlling for the influence of the other variables RR IVRT Independent Variables P Coef LA pressure Aortic notch pressure LV systolic pressure Peak ⫹dP/dt ⬍0.0001 0.817 0.287 0.604 0.060 ⫺0.0309 ⫺0.0007 0.0017 0.0013 ⫺0.0001 P Coef ⬍0.0001 1.228 ⬍0.0001 ⫺0.898 0.015 0.278 0.012 ⫺0.221 0.510 0.0004 RR and IVRT are dependent variables. GEE, Generalized Estimating Equation; Coef, coefficient; LV, left ventricular; dP/dt, instantaneous rate of change of LV pressure with respect to time. 281 • NOVEMBER 2001 • www.ajpheart.org ASSESSMENT OF RELAXATION BY LV RECOIL from the ventricular wall. These forces are stored when systolic contraction of the cavity to volumes below an “equilibrium volume” results in the stretch or compression of cellular and extracellular proteins such as titin (11) and collagen (29, 34, 46). The development of counterclockwise torsion during systole leads to transmural equilibration of fiber shortening (4) and allows a greater deformation of elements within the wall for any given ventricular volume (14). This is particularly true in the endocardium, where the counterclockwise torque is in the direction opposite to the alignment of fibers, and considerable deformation of the connective tissue matrix must occur (35, 43). This may permit more energy to be stored within the wall. The release of this repository of force during isovolumic relaxation creates ventricular suction, returning the stored energy to the circulation (45). Preload independence. As expected, IVRT shortened significantly with volume loading and proved highly dependent on LA pressure in the multivariate analysis. In contrast, RR was unchanged with fluid loading (which increased LA pressure from 9 to 14.6 mmHg), and, in the multivariate analysis, there was no contribution of LA pressure toward RR. This demonstration of preload independence suggests that RR may not be subject to “pseudonormalization” in situations where LA pressure rises or to overestimation of diastolic abnormalities in situations where LA pressure is low, for example, during dehydration. The influence of other factors not directly related to relaxation, such as mitral inertance and atrial contractility, on RR could not be assessed by this study but is likely to be less for this isovolumic phase index than for indexes of diastolic function measured during filling. Two new Doppler measurements have also been shown to reflect relaxation with only minimal preload dependence. Color M-mode Doppler detects the velocity of propagation of the filling wave between the mitral valve and LV apex during early filling (7, 39). This velocity is dependent on the presence of intraventricular gradients, which appear to be more closely related to the ventricular relaxation process than to the atrial driving force. Tissue Doppler echocardiography (16, 21) detects myocardial long-axis lengthening velocity during early (E wave) and late (A wave) diastole. The preload independence of this method could relate to a preferential effect of ventricular relaxation on base-toapex dimension changes, whereas atrial driving force might affect lengthening in the circumferential direction. However, both of these new echocardiographic methods depend on measurements made after most of the relaxation process has already been completed, which reduces their sensitivity. More importantly, they are recorded after filling begins so some influence of load is therefore to be expected (1, 32, 42). A third type of Doppler method has been described, which can be measured during isovolumic relaxation; the rate of decay of a mitral regurgitation jet (12) or rate of acceleration of an aortic regurgitation jet (36) is interrogated. However, this measure requires the presence of a regurgitant jet that is large enough to produce a AJP-Heart Circ Physiol • VOL H2007 continuous signal, and this method is not load independent, because mitral regurgitation is determined by atrial as well as ventricular pressure and aortic regurgitation is closely related to aortic diastolic pressure. The current study utilized only MRI and hemodynamic variables and could not compare the utility of RR with these new echocardiographic parameters. However, we were able to compare RR with IVRT, an older index of relaxation that can be measured by echocardiography (28). IVRT was significantly affected by volume loading, and its correlation with was less consistent and more variable than that of RR, probably due to its greater dependence on LA pressure. Limitations. Several limitations exist in the interpretation of these data. First, as noted above, our study did not allow comparison of the relative value of this new index of relaxation with newer echocardiographic techniques. We also did not assess the effects of regional wall motion abnormalities. Such studies will be important in defining the role that this method will ultimately play. Second, correlation of RR with was high (⫺0.86 for individual experiments, ⫺0.92 for pooled data), but the corresponding r2 values (0.75 and 0.84, respectively) indicate that there are components of the variation of RR that are not entirely explained by . Note that the SD of RR is higher than that of . Errors in defining the endocardial-tag intersections (which was done by hand), limitations in image resolution due to pixel size (which averaged 1.5 mm), and image times of several minutes in the absence of respiratory gating may have contributed to this variation. Automatic tag-tracking algorithms and improved speed and pixel resolution in newer magnetic resonance systems will reduce these problems in the future. Third, the heart rates in the dogs studied were high due to anesthesia and the need for atrial pacing at a constant rate (to assure accurate gating); this prevented us from studying the rate dependence of RR. It also raises the question of whether our results are generalizable to slower rates. We suspect that rate is not an important confounder here because studies of human transplant recipients (28, 45) at physiological rates yielded results consistent with ours. Fourth, RR was determined using a linear regression of recoil versus time, whereas pressure is known to decline in an exponential fashion starting at peak ⫺dP/dt (44). We tested an exponential model as well and found similar correlations, but chose the more simple linear model because our temporal resolution was not adequate to define an appropriate starting point (i.e, peak ⫺dP/dt) for an exponential relationship. Higher temporal resolution is now available using the latest magnetic resonance scanners, and future studies might attempt various exponential fits. The pioneering works in this field by Yun et al. (46) and Moon et al. (29) also used linear models. Finally, we used tagged MRI for these experiments. The availability of this technique is currently limited, and specialized software is required for analysis. However, cardiac magnetic resonance is recognized as an excellent research tool and is growing in popularity and accessibility for clinical care. Fur- 281 • NOVEMBER 2001 • www.ajpheart.org H2008 ASSESSMENT OF RELAXATION BY LV RECOIL thermore, there may be potential for visualizing LV apical rotation and recoil using tissue Doppler echocardiography, a widely available technology. In summary, the rate of recoil of LV torsion, which can be determined wholly noninvasively, provides an isovolumic phase, preload-independent assessment of LV relaxation. Use of this novel parameter should allow the detailed study of diastolic function in states known to affect filling rates, such as aging, hypertension, and congestive heart failure, and may provide an estimate of the function of the relaxation process in individual patients, allowing serial measurements to follow therapeutic interventions. We are grateful to Dr. Edward G. Lakatta for thoughtful critiques of these concepts and to Stephanie Bosley for superb technical operation of the MRI scanner and processing of the image data. This study was supported by National Heart, Lung, and Blood Institute Grant RO1 HL-46223 (to E. P. Shapiro). This paper was presented in part at the 70th Annual Scientific Sessions of the American Heart Association, Orlando, Florida, November 1997. REFERENCES 13. 14. 15. 16. 17. 18. 19. 1. Agmon Y, Oh JK, McCarthy JT, Bailey KR, and Seward JB. Are diastolic velocities of the mitral annulus load-dependent? A tissue-Doppler study in hemodialysis patients (Abstract). J Am Coll Cardiol 2, Suppl A: 429A, 1999. 2. Appleton CP. Hemodynamic determinants of Doppler pulmonary venous flow velocity components: new insights from studies in lightly sedated normal dogs. J Am Coll Cardiol 30: 1562– 1574, 1997. 3. Appleton CP, Galloway JM, Gonzalez MS, Gaballa M, and Basnight MA. Estimation of left ventricular filling pressures using two-dimensional and Doppler echocardiography in adult patients with cardiac disease. Additional value of analyzing left atrial size, left atrial ejection fraction and the difference in duration of pulmonary venous and mitral flow velocity at atrial contraction. J Am Coll Cardiol 22: 1972–1982, 1993. 4. Arts T and Reneman RS. Measurement of deformation of canine epicardium in vivo during cardiac cycle. Am J Physiol Heart Circ Physiol 239: H432–H437, 1980. 5. Axel L and Dougherty L. MR imaging of motion with spatial modulation of magnetization. Radiology 171: 841–845, 1989. 6. Beyar R, Yin FCP, Hausknecht M, Weisfeldt ML, and Kass DA. Dependence of left ventricular twist-radial shortening relations on cardiac cycle phase. Am J Physiol Heart Circ Physiol 257: H1119–H1126, 1989. 7. Brun P, Tribouilloy C, Duval AM, Iserin L, Meguira A, Pelle G, and Dubois-Rande JL. Left ventricular flow propagation during early filling is related to wall relaxation: a color M-mode Doppler analysis. J Am Coll Cardiol 20: 420–432, 1992. 8. Brutsaert DL, Rademakers FE, Sys SU, Gillebert TC, and Housmans PR. Analysis of relaxation in the evaluation of ventricular function of the heart. Prog Cardiovasc Dis 28: 143– 163, 1985. 9. Buchalter MB, Weiss JL, Rogers WJ, Zerhouni EA, Weisfeldt ML, Beyar R, and Shapiro EP. Noninvasive quantification of left ventricular rotational deformation in normal humans using magnetic resonance imaging myocardial tagging. Circulation 81: 1236–1244, 1990. 10. Burgess MJ, Lux RL, Ershler PR, and Menlove R. Determination of transmural location of onset of activation from cardiac surface electrograms. Circulation 82: 1335–1342, 1990. 11. Cazorla O, Freiburg A, Helmes M, Centner T, McNabb M, Wu Y, Trombitas K, Labeit S, and Granzier H. Differential expression of titn isoforms and modulation of cellular stiffness. Circ Res 86: 59–67, 2000. 12. Chen C, Rodriguez L, Lethor JP, Levine RA, Semigran MS, Fifer MA, Weyman AE, and Thomas JD. Continuous wave Doppler echocardiography for noninvasive assessment of AJP-Heart Circ Physiol • VOL 20. 21. 22. 23. 24. 25. 26. 27. 28. 29. 30. 31. left ventricular dP/dt and relaxation time constant from mitral regurgitant spectra in patients. J Am Coll Cardiol 23: 970–976, 1994. DeAnda A Jr, Komeda M, Nikolic SD, Daughters GT, Ingels NB, and Miller DC. Left ventricular function, twist, and recoil after mitral valve replacement. Circulation 92, Suppl 9: II458–II466, 1995. Dong SJ, Hees PS, Huang WM, Buffer SA, Weiss JL, and Shapiro EP. Independent effects of preload, afterload, and contractility on left ventricular torsion. Am J Physiol Heart Circ Physiol 277: H1053–H1060, 1999. Fraites TJ Jr, Saeki A, and Kass DA. Effect of altering filling pattern on diastolic pressure-volume curve. Circulation 96: 4408–4414, 1997. Garcia MJ, Rodriguez L, Ares M, Griffin BP, Klein AL, Stewart WJ, and Thomas JD. Myocardial wall velocity assessment by pulsed Doppler tissue imaging: characteristic findings in normal subjects. Am Heart J 132: 648–656, 1996. Gibbons Kroeker CA, Ter Keurs HEDJ, Knudtson ML, Tyberg JV, and Beyar R. An optical device to measure the dynamics of apex rotation of the left ventricle. Am J Physiol Heart Circ Physiol 265: H1444–H1449, 1993. Gibbons Kroeker CA, Tyberg JV, and Beyar R. Effects of load manipulations, heart rate, and contractility on left ventricular apical rotation. An experimental study in anesthetized dogs. Circulation 92: 130–141, 1995. Gilbert JC and Glantz SA. Determinants of left ventricular filling and of the diastolic pressure-volume relation. Circ Res 64: 827–852, 1989. Glantz SA and Slinker BK. Primer of Applied Regression and Analysis of Variance. New York: McGraw-Hill, 1990, p. 381–390. Isaaz K, Thompson A, Ethevenot G, Cloez JL, Brembilla B, and Pernot C. Doppler echocardiographic measurement of low velocity motion of the left ventricular posterior wall. Am J Cardiol 64: 66–75, 1989. Ishida Y, Meisner JS, Tsujioka K, Gallo JI, Yoran C, Frater RW, and Yellin EL. Left ventricular filling dynamics: influence of left ventricular relaxation and left atrial pressure. Circulation 74: 187–196, 1986. Knudtson ML, Galbraith PD, Hildebrand KL, Tyberg JV, and Beyar R. Dynamics of left ventricular apex rotation during angioplasty: a sensitive index of ischemic dysfunction. Circulation 96: 801–808, 1997. Kuecherer HF, Muhiudeen IA, Kusumoto FM, Lee E, Moulinier LE, Cahalan MK, and Schiller NB. Estimation of mean left atrial pressure from transesophageal pulsed Doppler echocardiography of pulmonary venous flow. Circulation 82: 1127– 1139, 1990. Liang KY and Zeger SL. Longitudinal data analysis using generalized linear models. Biometrics 73: 13–22, 1986. MacGowan GA, Burkhoff D, Rogers WJ, Salvador D, Azhari H, Hees PS, Zweier JL, Halperin HR, Siu CO, Lima JA, Weiss JL, and Shapiro EP. Effects of afterload on regional left ventricular torsion. Cardiovasc Res 31: 917–925, 1996. Matsubara H, Takaki M, Yasuhara S, Araki J, and Suga H. Logistic time constant of isovolumic relaxation pressure-time curve in the canine left ventricle. Better alternative to exponential time constant. Circulation 92: 2318–2326, 1995. Mattheos M, Shapiro E, Oldershaw PJ, Sacchetti R, and Gibson DG. Non-invasive assessment of changes in left ventricular relaxation by combined phono-, echo-, and mechanocardiography. Br Heart J 47: 253–260, 1982. Moon MR, Ingels NB, Daughters GT, II, Stinson EB, Hansen DE, and Miller DC. Alterations in left ventricular twist mechanics with inotropic stimulation and volume loading in human subjects. Circulation 89: 142–150, 1994. Nikolic S, Yellin EL, Tamura K, Vetter H, Tamura T, Meisner JS, and Frater RWM. Passive properties of canine left ventricle: diastolic stiffness and restoring forces. Circ Res 62: 1210–1222, 1988. Nishimura RA and Tajik AJ. Evaluation of diastolic filling of left ventricle in health and disease: Doppler echocardiography is the clinician’s Rosetta Stone. J Am Coll Cardiol 30: 8–18, 1997. 281 • NOVEMBER 2001 • www.ajpheart.org ASSESSMENT OF RELAXATION BY LV RECOIL 32. Pai PY, Oh JK, Ommen SR, Lusk JL, and Tajik AJ. Acute preload alteration affects mitral annulus velocities measured by tissue doppler. Circulation 100: I–777, 1999. 33. Pearson AC, Gudipati CV, Labovitz AJ. Effects of aging on left ventricular structure and function. Am Heart J 121: 871– 875, 1991. 34. Rademakers FE, Buchalter MB, Rogers WJ, Zerhouni EA, Weisfeldt ML, Weiss JL, and Shapiro EP. Dissociation between left ventricular filling and untwisting: accentuation by catecholamines. Circulation 85: 1572–1581, 1992. 35. Rademakers FE, Rogers WJ, Guier WH, Hutchins GM, Siu CO, Weisfeldt ML, Weiss JL, and Shapiro EP. Relation of regional cross-fiber shortening to wall thickening in the intact heart. Three-dimensional strain analysis by NMR tagging. Circulation 89: 1174–1182, 1994. 36. Rombaut E, Abergel E, Delouch A, Raffoul H, Diebold H, Augusseau M, Ledru F, and Diebold B. Noninvasive measurement of the LV tau constant: a doppler echocardiographic approach of the left ventricular relaxation (Abstract). J Am Coll Cardiol 31: 295A, 1998. 37. Rossvoll O and Hatle LK. Pulmonary venous flow velocities recorded by transthoracic Doppler ultrasound: relation to left ventricular diastolic pressures. J Am Coll Cardiol 21: 1687– 1696, 1993. 38. Snedecor GW and Cochran WG. Statistical Methods. Ames, IA: Iowa State University Press, 1967. 39. Takatsuji H, Mikami T, Urasawa K, Teranishi J, Onozuka H, Takagi C, Makita Y, Matsuo H, Kusuoka H, and Kitabatake A. A new approach for evaluation of left ventricular diastolic function: spatial and temporal analysis of left ventric- AJP-Heart Circ Physiol • VOL 40. 41. 42. 43. 44. 45. 46. 47. H2009 ular filling flow propagation by color M-mode Doppler echocardiography. J Am Coll Cardiol 27: 365–371, 1996. Thomas JD, Flachskampf FA, Chen C, Guererro JL, Picard MH, Levine RA, and Weyman AE. Isovolumic relaxation time varies predictably with its time constant and aortic and left atrial pressures: implications for the noninvasive evaluation of ventricular relaxation. Am Heart J 124: 1305–1313, 1992. Thomas JD and Weyman AE. Echocardiographic Doppler evaluation of left ventricular diastolic function. Physics and physiology. Circulation 84: 977–990, 1991. Van Dantzig JM, Dassen WRM, Lucas CMHB, and Cheriex EC. Propagation velocity of mitral inflow is load-dependent in congestive heart failure. Circulation 100: I–295, 1999. Waldman LK, Nosan D, Villarreal F, and Covell JW. Relation between transmural deformation and local myofiber direction in canine left ventricle. Circ Res 63: 550–562, 1988. Weiss JL, Frederiksen JW, and Weisfeldt ML. Hemodynamic determinants of the time-course of fall in canine left ventricular pressure. J Clin Invest 58: 751–760, 1976. Yellin E. Concepts related to the study of diastolic function: a personal commentary. J Cardiol 33: 223–236, 1999. Yun KL, Niczyporuk MA, Daughters GT, II, Ingels NB, Stinson EB, Alderman EL, Hansen DE, and Miller DC. Alterations in left ventricular diastolic twist mechanics during acute human cardiac allograft rejection. Circulation 83: 962– 973, 1991. Zerhouni EA, Parish DM, Rogers WJ, Yang A, and Shapiro EP. Human heart: tagging with MR images–a method for noninvasive assessment of myocardial motion. Radiology 169: 59– 63, 1988. 281 • NOVEMBER 2001 • www.ajpheart.org