Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
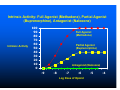
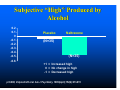
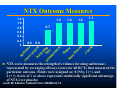
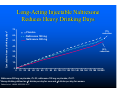
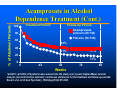
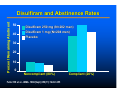
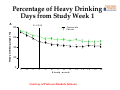
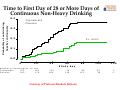
What is Addiction and How Do We Treat It? Roger D. Weiss, M.D. Professor of Psychiatry, Harvard Medical School Clinical Director, Alcohol and Drug Abuse Treatment Program, McLean Hospital, Belmont, MA DSM-IV SUBSTANCE DEPENDENCE CRITERIA A maladaptive pattern of substance use, leading to clinically significant impairment or distress, as manifested by 3 or more of the following in the same 12month period. 1. Tolerance, as defined by: a. A need for markedly increased amounts of the substance to achieve intoxication or desired effect, or b. Markedly diminished effect with continued use of the same amount of the substance. DSM-IV SUBSTANCE DEPENDENCE CRITERIA (CONT.) 2. Withdrawal, as manifested by: a. The characteristic withdrawal syndrome for the substance, or b. The same (or a closely related) substance is taken to relieve or avoid withdrawal sx 3. The substance is often taken in larger amounts or over a longer period than was intended. DSM-IV SUBSTANCE DEPENDENCE CRITERIA (CONT.) 4. A persistent desire or unsuccessful efforts to cut down or control substance use. 5. A great deal of time spent in activities necessary to obtain the substance (e.g., visiting multiple doctors), use the substance, or recover from its effects. 6. Important social, occupational, or recreational activities given up or reduced because of substance use. DSM-IV SUBSTANCE DEPENDENCE CRITERIA (CONT.) 7. Continued substance use despite knowledge of having a persistent or recurrent physical or psychological problem likely to have been caused or exacerbated by the substance. DSM-IV SUBSTANCE DEPENDENCE Tolerance and withdrawal are neither necessary nor sufficient for a diagnosis of substance dependence Physical dependence vs. drug dependence (addiction) Quantity/frequency, level of consequences not part of the DSM-IV criteria Abuse vs. Dependence No tolerance, withdrawal, compulsive use in abuse Some people remain abusers, never become dependent Not inevitably progressive Alcohol problems occur along a continuum of severity Recovery from Alcohol Dependence Over 50% recovery rate in community male samples Drinking rate: 40% after 2 years, 4% after 5 years sobriety PSYCHOTHERAPY FOR SUBSTANCE USE DISORDERS Formerly viewed as contraindicated In past 2 decades, renewed interest SUD-specific treatment Rigorous outcome studies Behavioral Therapy for Substance Use Disorders Numerous studies show positive results for various types of behavioral therapy Non-confrontational approaches, positive contingencies appear most helpful Self-help groups (e.g., AA) are commonly used and are associated with positive outcomes, lower healthcare costs PHARMACOTHERAPY OF SUBSTANCE USE DISORDERS Maintenance drugs (e.g., methadone, buprenorphine) Drugs to block euphoria (eg., naltrexone for opioids) Drugs to induce aversive consequences (disulfiram) Drugs to treat co-existing psychiatric disorders Drugs to treat substance-induced disorders, e.g., acute or protacted withdrawal, craving (naltrexone, acamprosate for alcohol) Prescribing Medication vs. Taking Medication What Are the Parameters Used to Determine Treatment Efficacy? For alcohol Percent days abstinent Percent days heavy drinking Likelihood of any drinking (abstinence rate) Likelihood of heavy drinking Drinks per drinking day Time to first drink/relapse Consequences of drinking Biological markers METHADONE MAINTENANCE Goal is rehabilitation, not abstinence Substitutes a long-acting, oral, legal, qualitycontrolled drug for a short-acting, illegal, poorquality,expensive, injectable drug Dose of >60 mg/day most successful Best results occur with concomitant psychosocial tx METHADONE MAINTENANCE ADVANTAGES Decreased illicit opioid use, crime, unemployment, HIV seroconversion, healthcare costs Randomized study of MM vs. drug-free tx showed better results for MM, but neither did particularly well METHADONE MAINTENANCE DISADVANTAGES Patients may be tied to clinic Takehomes may lead to illicit diversion Interactions with other drug users Other substance use disorders: EtOH, cocaine, BZs, marijuana Difficult to detoxify Buprenorphine A partial agonist; does not fully activate opioid receptors. Binds tightly and dissociates slowly from opioid receptors A ceiling effect on opioid activity, including respiratory depression. Result = likelihood of death from buprenorphine overdose markedly diminished. Advantage over naltrexone: has mild agonist effects; patient does not have to be detoxified to begin treatment. Intrinsic Activity: Full Agonist (Methadone), Partial Agonist (Buprenorphine), Antagonist (Naloxone) Intrinsic Activity 100 90 80 70 60 50 40 30 20 10 0 Full Agonist (Methadone) Partial Agonist (Buprenorphine) Antagonist (Naloxone) -9 -8 -7 -6 Log Dose of Opioid -5 -4 Buprenorphine Maintenance Therapy Clinical trials have established the effectiveness of buprenorphine for treatment of heroin addiction. Direct comparisons to methadone suggest that it as effective as moderate doses of methadone (e.g., up to 60 mg/day), although it is not clear whether it can be as effective as higher doses of methadone for maintenance therapy. Buprenorphine is mildly reinforcing , thus ensuring better compliance than naltrexone or “drug free” therapies. Buprenorphine-Naloxone (Suboxone) Naloxone added to maintenance formulation to deter parenteral abuse Naloxone has low bioavailability when used sublingually Safety and efficacy of buprenorphine/naloxone appear equivalent to buprenorphine alone No special safety or side effect considerations for this combination Naltrexone for Opioid Dependence Naltrexone is long-acting oral analog of naloxone (Narcan): a pure opiate antagonist (blocker) Binds to opiate receptors more strongly than opiates do Taking opiates on naltrexone leads to blockade of opiate effects Naltrexone has no opiate properties Efficacy limited by limited acceptability, except by specific populations, usually under pressure Naltrexone for Alcohol Dependence Volpicelli et al (1992) 70 VA patients, all men with alcohol dependence 12-wk double-blind, placebo controlled Naltrexone 50mg/day Day treatment (6hrs/d) for 1 month, then twice/week group therapy for 2 months Major psychiatric illness excluded 23% of NTX Ss vs. 54% placebo Ss relapsed; similar rate of drinking Subjective “High” Produced by Alcohol 0.2 0.1 0 -0.1 -0.2 -0.3 -0.4 -0.5 -0.6 Placebo Naltrexone (N=35) (N=35) +1 = Increased high 0 = No change in high -1 = Decreased high p<0.006; Volpicelli JR et al. Am J Psychiatry. 1995(April);152(4):613-615 Naltrexone forAlcohol Dependence May reduce alcohol-induced craving May reduce craving independent of drinking Differences in the experience of a slip Does not make someone a controlled drinker Helps a pt get back to abstinence faster Mostly positive studies, but some negative NTX Outcome Measures 1.2 1.0 0.8 0.6 0.4 0.2 0 1.0 1.0 1.0 1.1 0.7 Cr av Ti m Ab st in g 0.0 in en et ce o 1s tD rin #o k fD rin kin Da g Dr ys in ks /D rin kD ay Re lap se He av yD rin kin g 0.0 NTX score measures the strength of evidence favoring naltrexone, represented by averaging efficacy scores for all RCTs that measured the particular outcome. Points were assigned as: 0 (NS), 1 (+), and 2 (++). Score of 1 or above represents statistically significant advantage of NTX over placebo Leavitt SB. Addiction Treatment Forum. 2002(March):1-8 Long-Acting Injectable Naltrexone Reduces Heavy Drinking Days Cumulative heavy drinking days* 70 17% reduction Placebo 60 Naltrexone 190 mg 50 Naltrexone 380 mg 40 26% reduction 30 20 10 0 0 10 20 30 40 50 60 70 80 90 100 110 120 130 140 150 160 170 180 190 200 Naltrexone 380 mg vs placebo, P=.03; naltrexone 190 mg vs placebo, P=.07. *Heavy drinking defined as ≥5 drinks per day for men and ≥4 drinks per day for women. Garbutt et al., JAMA 2005;293:1617. Acamprosate (N-acetylhomotaurine) Mechanism: interacts with glutamate and GABA neurotransmitters systems In animal models of alcohol dependence, acamprosate reduced deprivation-induced drinking Does not cause dependence or withdrawal May reduce protracted withdrawal symptoms Acamprosate in Alcohol Dependence Treatment (Sass,1996) Study conducted in Germany/Austria 272 patients receiving routine counseling and treated with 2 g/day acamprosate or placebo for 48 weeks Sass H et al. Arch Gen Psychiatry. 1996(Aug);53(8):673-680 % of Abstinent Patients Acamprosate in Alcohol Dependence Treatment (Cont.) Treatment Period* 100 Follow-Up Period† Acamprosate calcium (N=136) Placebo (N=136) 80 60 43% 40 21% 37% 20 17% 0 0 24 48 72 96 Weeks *p=0.001; †p=0.003; 272 patients were entered into the study over 2 years; Kaplan-Meier survival analysis (survival function estimate); continuous abstinence for the treatment and follow-up periods; Sass H et al. Arch Gen Psychiatry. 1996(Aug);53(8):673-680 NIAAA COMBINE Study Studied optimal combinations of medications, behavioral Tx for alcohol dependence Patients received naltrexone, acamprosate, both, or neither Half of patients received psychotherapy in addition to medical management One patient cohort received psychotherapy alone, no pills COMBINE Study: Results For patients receiving MM, naltrexone or CBI therapy improved outcomes over placebo plus MM Acamprosate did not add benefit to naltrexone or CBI, and was no more effective than placebo plus MM Taking pills and seeing a health care professional was more effective than receiving CBI alone (possible placebo effect) Disulfiram Inhibits aldehyde dehydrogenase, an enzyme in the metabolism of alcohol Leads to acetaldehyde poisoning when alcohol is ingested Reaction occurs 10-15 min. after drinking Reaction can be quite severe, occasionally fatal; severity is related to dose and individual characteristics Percent Remaining Abstinent Disulfiram and Abstinence Rates 50 40 Disulfiram 250 mg (N=202 men) Disulfiram 1 mg (N=204 men) Placebo 30 20 10 0 Noncompliant (80%) Fuller RK et al. JAMA. 1986(Sept);256(11):1449-1455 Compliant (20%) Disulfiram ADVANTAGES: Built-in impulse control because of prolonged elimination time (up to 2 weeks) May indirectly reduce desire to drink Best used in careful, impulsive, situational drinkers May be used prn later Importance of adherence strategies Disulfiram DISADVANTAGES: Side effects, including liver toxicity Risk of unintentional or intentional alcohol reaction Possible overreliance on disulfiram, underreliance on other supports Topiramate Johnson et al., 2007 371pts at multiple sites received topiramate 50-300 mg/d (tapered upward) or placebo x 14 wks Patients were drinking heavily at study entry Topiramate pts had better drinking outcomes, beginning at 100 mg Fewer heavy drinking days Greater likelihood of abstinence Percentage of Heavy Drinking Days from Study Week 1 Heavy drinking days (%) A P=.0 0 0 6 80 To piram ate Placebo 60 40 20 0 1 2 3 4 5 6 7 8 9 S tu d y w e e k 10 Courtesy of Professor Bankole Johnson 11 12 13 14 Time to First Day of 28 or More Days of Continuous Non-Heavy Drinking heavily continuously Probability of not drinking 0 .4 T o p ira m a t e P la c e b o 0 .3 0 .2 P < .0 0 0 1 0 .1 0 .0 0 N u m b e r o f p a r t ic ip a n t s T o p ir a m a t e 179 P la c e b o 185 20 a t r is k 139 174 40 60 S tu d y d ay 80 103 164 79 139 68 121 Courtesy of Professor Bankole Johnson 100 22 39 120 0 0 Pharmacotherapy of Cocaine Dependence No reliably effective medications for cocaine dependence in general Pharmacotherapy for specific subgroups of cocaine dependent patients may be effective: Antidepressants for pts with major depressive disorder (Nunes, 1991). Amantadine for patients with severe withdrawal symptoms (Kampman,2000)