Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
History of invasive and interventional cardiology wikipedia , lookup
Heart failure wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Cardiac surgery wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Electrocardiography wikipedia , lookup
Myocardial infarction wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Coronary artery disease wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
Atrial septal defect wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Right Axis Deviation, Clockwise QRS Loop, and
Signs of Left Ventricular Underdevelopment in
a Child with Complete Type of Persistent
Common Atrioventricular Canal
BY DAVID BAUMT,lM.D., GILBFBfI J. P0-For, NI ED,
lar aiioi-nalies,";
T HE electrocardiogram has proved to sup-
ply relialle iniformation for clliical
AN-) S. ALLISON
"
CHREIGHTON-, 1.D.
iincluiding instances of the
ostium sceciiunduiim type of atrial defect.1 2,
ree-
Downloaded from http://circ.ahajournals.org/ by guest on April 28, 2017
1-lowever, aniatomically proved cases of complete persistent common atrioventricular canal
uincattendeld I)y the clharacteristic electrocar-
ognition of cardiac defects of the type known
as complete form of persisteint comlmmIon atrioventrictular canal." 2The electrocardiographlic
findinig.s conisistently associated witlh these de~
fects hax e b)een left axis deviationi and Q1S
vectors in the frontal plane which (lescril)e a
counterclockwise lo0 above the isoelectric
point, or a figture-of-eight loop alonig the lorizontal liniie. These patternis are thought to be
a resuilt of an abnormality inlvolving the venltricuilar c oniduiiction pathxxways.4 These clectrocardiograph ic findings have been described
with varying frequiency in other ctrdiovascui-
(liotgram
are rare."', 11 The case to be presented ler.e is suichl a onie, but includes two
uinuisuial feattures, naiely, left veintrictilar hypoplasia aid ol)struction to left ventricular
outflow. The electrocardiogram revealed right
axis deviationi anlid a clockwtise inscription of
the QRS vector loop in the fronital plane. Of
additional interest in this case were features
that stiggested iiunderdevelopment of the left
ventricle.
Case Report
A 2-vear-o el girl a\\as adnitted to the Childr en's Orthopedic Hospital at the age of
6 moniths. A heart iulimnrn wvas first (letected ini
FP aomi tlhe Departments of Pediatries and Patlology, tJiniversity of Waishinigtoni School of Medicine,
and Children's Orthiopedlic f-lospital, Seattle, W ashingtoll.
4F
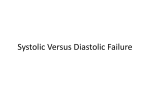
Figure 1
I eft. Posteroanterior roc ntg r n of f/ic elicit reucaino" carr/iooegaht, prominence of thle
pulmonarty artery segment, andt] iincrcased pulm/toiarIj vascnlarity. Riglht. Fl onltal mie2w of
the leart and great cessels at autopslm. 1T/i attm.ows point to the iitervcntriCular s/leCs, lwlhich1
LV., left rcntrich
is disp/acc scperioly/ and l/atrafihl. lEX., riglit Len ic/c,;
( aidation,
V
in
\ \ ',
Notti,er
1)0
t)65
9
7,'? 5
756
B6fAUNt' FT AI.
earl,' infancy aiid chioiic conigestixe h]eart faillire became manifest at 5) ml]oIIths. Phvisical eanimiation r evealed a relativelvx ci nourished
child xw ho had tanchvc dia and mlikld r-espiraltorx
distress. She had a left precor(Iial 1)bilge, lhvpeactive pilecoi)diuiiol, loud secondlheadtlt souiid, sxStolic thrill, and a grade-IV/VI lbolg, harsh sS-
tolic murirnti. l)est heard along the left sternal
a mid-diastolic ruimbling miurnmur localized betwveen the apex and the lower left
l)ordcr, and
Table 1
Data Obtained at Car.diac Cathieterization Demonstrating Lef t-o-Right Shunting at Atrial annd
Ventricular Levelts, Pulmonary Hypertension, and
AMild Systemic Arterial Desaturation
Downloaded from http://circ.ahajournals.org/ by guest on April 28, 2017
o ('Content
c ( )2
vol). 1,7
Satirt ation
It ttnili
Superior vena c iva
Rig(Jht atrium, midl
Right atrium, loxxRigrht venitriclc, inf-llo,x
Right vcntrilcle, ouitflo,xx
Pulmonarx arterv
Ptolmoinary artery x ( (lgc
Systeimiie artery
5.4
9.5
11.4
11.6
13.6
34
56
62
63
60
13.3
78
perisistenit comm-1i11on0 aitriovemitricutilar caneial (fig. 1,
r ight, anl fig. 3) \Iodcerate hepatomegalx xw as
presenit. The Ilungs on1 gross examiiina1itioni xxere
62/8
50)/20
4/2
15.3
90
Palmrooiary 1)100(1 flow-6.2 L,./mim./NI.2
floxxIs1.9 L.--- \il
/1.2
Syst'rMi_ lo)]
Et ssule,
lg
111111.
steinal )0o1der. The chlest roenitgeniogria.ts provide(1 evidleice (fig. 1, left) of cardiomiegax
ad
mlc reased )liliiion,a,r xascularvitx Criac catheterizati)i data (table 1) indicated the preseiice
of left-to- ighit slhuniitinig at atrtil tiiand x e(,iit ic-u
lar levels, atind1l
lix, pertensioii. \lild
sxvsteimiic arterial (lesatiniaoti xixs tholught to lbe
dule to respiratorx dlepressioin. Becse of the
character of the electrocardiogi-aphie evi(lejicWe, a
diagniosis wVas i--iadle of entriular septail d3efect
aid coexistent ostitiuim seciiciuidid-ty pe atrial septal defect rather thani of per.sistent commonil atriovenitricular canail (fig. 2) Becauise the child's
heart failtire ecoldnlot he eontrolled lxv miedical
xir asen ltakent
measuires, smrgical treatment
xvhein the patien -tx as 2 emrs of age. The patienit lied early in the postope-mative perlioil.
Postmortem Cexain1in ationll revealedl
poplasia
of the left vemiti-iele, fibrolls bllmds olb.stlrluctilg
the left ventrictlar. ouitfloxv tract, andl comiplete
72/50
relativelv niormal. \Iicroscopic examinatiolln,
ever, revxaled m1]ild hemorrhage ad edicl
oxsa al
early- pulmon()ambl vs ascidar (lisease.
Discussion
In the case presented herc complhte persisteuit coniniioni atrtiox eutricenlar canal exi sted
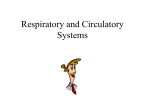
Figure 2
Twelhe-lead scalar /'etrOeadiogra (Ilmlnstrating rig/it axis (ldeciation and right rentrictl/ar
overl1load. Note the aipparctt clockwise direct on of the QR.S insciptitn in the frontal plane.
Circ i/i/ton V
XXXtut
\'\. \196ii n
I
04
7.O7
CONI-\ION ATRIOVENTIIICTLAR (CA'NA L
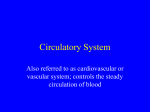
Figure 3
Downloaded from http://circ.ahajournals.org/ by guest on April 28, 2017
Anatonm ic deton.stration of the conml)lete persistent atrioven2triicilat canal tied ftrout the right
ventricle (left) and the left wertiticle (right). Filbrous bands obstrutctingr the If t tentricnlat
remoced. V, oitijontrflitticutlar valve; AD, ritrial potiion of dlefeci; VD,
otttflotv tract have buttei
ventricilar 1)pottiort of cIt favt.
unattended bgy electrocardiographic findings
typical of suich a lesion. Awareness of this
possil)ility is of importance when considering
suirgical treatmenet for a paticnit wxxho has leftto-right shunting at both atrial anid ventricuilar levels. Of ad(litionial interest xvas the exist('fcle of left venitricuilar hylpoplasia anid dominant left-to-right shlutnting at ventricular level
in tie al)sence of electr-ocaridiographic evidence of left xventricular overload. Finally, as
a r-esu.lt of underdevelopmienit of the left
ventricle, evidence of posterior, suiperior, and
letwtvard displacement of the interventricular
slicris xas observed on the clhest roentgenogram. Recognition of the latter txwo circumstances in a patient with congenital heart disease should alert the physician to the need
for angiocardiographic study of the left ventricle.
Summary
C1nlical data and finidings at necropsy are
presented on a 2-year-old girl xxlho had persistenit complete commoni atrioventricular can-al, hypoplastic left ventricle, and obstruction
to tlhe left venitricular otutflow tract. Electrocardiographic findings xxere atypical of common atrioventricular canial in that right axis
deviationi and a clockvise inscription of the
QRS loop in the frontal planie vere presenit.
Findings in this case suggest that under(levelopment of the left ventricle should be
Vaul
t rculat:ot,
Yoln,
XXXJ No! embeo b964
stuspected xvhei ( 1) displacement of the interventricuilar sni.cuis is noted on roenitgenographic examiniationis and (2) predomninanit left-torighit shuntinig at ventricular level is fouind
in the absence of electrocardiographic evidence of left ventrietular oxerloaid.
Acknowledgment
1)rs. jack
Doctor, Stanley Staniit, and Dean Cr)vstal of the
Chlildren's Ortlhopelic llospitzl for permiissioni to pre~
WAe Xi.sh
senit tlhis
to express mnr appreciation to
ease.
Refereiiees
1.
2.
Bu'CHELL, I1. B., DuSilA\Ez, J. WX., xiu) BRADEN-3ULG, R. 0.: TF e electrocardiogram of patients with atrioox enitricular cushion defects
(defects of tlhe atrioxventricular canal). Ami. J.
Cardiol. 60: 575, 1960.
LIEBMIAN-, j., AD-i) NADAS, A. S.: The vectorcardiogramn in the differential diagnosis of
atrial septal defect in children. Circulation 22:
956, 1960.
3.
ToSCANXo-BARB(/)A,
E.,
BRA-NDE\-BURG, R. 0., AM-3)
BiCe ILELIL, 1i. B.: Eleetroecardiogrraphie studies of eases vitth intracardiac malformations
of tde atriox-eiiti-liculair canal. Proc. Staff Meet.,
Iavo Cliii. 31: 513t, 1956.
4.
5.
LEXO, NM.: The architecture of the conduction
system in congeniital hleart disease. 1. Colmiimon
atrioveiitrietilnhr orifice. Arch. Patlh. 65: 174,
1958.
NELUFELI), H. N., TIitus, J. L., DuSiu v, _1. W.,
BvncwEi,i 11. 13., AND EDWARDS, J. E.: Isoatveextrictlar septal dlefect of the persistent
ed
COfiiilioi) atrioventricilar canial type. Circulation 23: 685, 1961.
BAUM ET AL.
758
6. TOSCANO-BARBOZA, E., AND DUSHANE, J. W.:
Ventricular septal defect: Correlation of electrocardiographic and hemodynamic findings
in 60 proved cases. Am. J. Cardiol. 3: 721,
1959.
7. DuSHANE, J. W., AND KIRKLIN, j. W.: Selection for surgery of patients with ventricular
septal defect and pulmonary hypertension.
Circulation 21: 13, 1960.
8. NEUFELD, H. N., DUSHANE, J. W., WooD, E.
H., KIRKLIN, J. W., AND EDWARDS, J. E.:
Origin of both great vessels from the right
ventricle. I. Without pulmonary stenosis. Circulation 23: 399, 1961.
9. DuSi-iANE, J. W., WEIDMAN, W. H., BRANDENBURG, R. 0., AND KIRKLIN, J. W.: Differentiation of interatrial communications by clinical methods: Ostium secundum, ostium primum, common atrium, and total anomalous
pulmonary venous connection. Circulation 21:
363, 1960.
10. CASTLEMAN, B., AND KIBBEE, B. V.: Case records of the Massachusetts General Hospital.
Weekly clinicopathological exercises. Case
43401. New England J. Med. 257: 672, 1957.
1 1. KEITH, J. D., ROWE, R. D., AND VLAD, P.:
Heart Disease in Infancy and Childhood. New
York, The Macmillan Company, 1958, p. 271.
Downloaded from http://circ.ahajournals.org/ by guest on April 28, 2017
Pathology of Angina Pectoris
The association of coronary disease with angina was first recognized by Edward
Jenner from post-mortem examination, though it is possible that John Hunter, on
whose account, as his anginal symptoms dated from 1773, Jenner kept silence, knew
or suspected it in 1776 when John Fothergill published a fatal case of angina in
which at the post-mortem Hunter found that "the two coronary arteries from origin to
many of their ramifications on the heart were become one piece of bone." Jenner, who
is said to have diagnosed angina in Hunter in 1777, never directly published anything
on this subject, but he communicated his opinions to C. H. Parry, who in 1788 read a
paper, "An Inquiry into the Symptoms and Causes of the Syncope Anginosa, Commonly
called Angina Pectoris; illustrated by Dissections," to a small medical society in Gloucestershire of which Jenner was a member, and came to the conclusion that coronary
disease was the cause. In this paper, not published until eleven years later, he quoted
the case of ossification of the coronary arteries published by Black of Newry in 1795
and pointed out that he and Jenner had independently come to the same opinion in
1788.-Sm HUMPHRY DAVY ROLLESTON. The Harveian Oration. Great Britain, Cambridge University Press, 1928, p. 88.
Circulation, Volume XXX, November 1964
Right Axis Deviation, Clockwise QRS Loop, and Signs of Left Ventricular
Underdevelopment in a Child with Complete Type of Persistent Common
Atrioventricular Canal
DAVID BAUM, GILBERT J. ROTH and S. ALLISON CREIGHTON
Downloaded from http://circ.ahajournals.org/ by guest on April 28, 2017
Circulation. 1964;30:755-758
doi: 10.1161/01.CIR.30.5.755
Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231
Copyright © 1964 American Heart Association, Inc. All rights reserved.
Print ISSN: 0009-7322. Online ISSN: 1524-4539
The online version of this article, along with updated information and services, is
located on the World Wide Web at:
http://circ.ahajournals.org/content/30/5/755
Permissions: Requests for permissions to reproduce figures, tables, or portions of articles
originally published in Circulation can be obtained via RightsLink, a service of the Copyright
Clearance Center, not the Editorial Office. Once the online version of the published article for
which permission is being requested is located, click Request Permissions in the middle column of
the Web page under Services. Further information about this process is available in the Permissions
and Rights Question and Answer document.
Reprints: Information about reprints can be found online at:
http://www.lww.com/reprints
Subscriptions: Information about subscribing to Circulation is online at:
http://circ.ahajournals.org//subscriptions/