Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
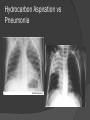
Developed By Alicia Kleinhans BSN RN CEN CCRN Objectives List 3 unique features of pediatric airway which are necessary to recognize for airway management Describe the main difference between ventilation and perfusion and list 2 ways this can cause hypoxemia Name at least 4 clinical signs of respiratory distress and respiratory failure List at least 3 causes of respiratory distress in pediatric patients and describe 2 methods of treatment Name at least 3 indicators for intubation Describe the 6 steps necessary for intubating a pediatric patient List 5 steps in a systematic approach to xray interpretation Airway is the key to success Normal Anatomy Normal Chest Anatomy Some things the same with adult vs Peds ie Tidal Volume 4.5-7ml/kg Most things different How does Pediatric airway differ from adults Narrowing of airway Anatomical Differences o Tongue proportionally larger o Epiglottis floppy, U shaped o Larynx more anterior and high – C2 in neonate, C3-4 in child, C5-6 in adult o Shorter - newborn trachea 5cm; 18 month old 7cm o Narrower – narrowest point at cricoid ring, uncuffed tubes <8 yrs functional seal Anatomical differences o Chest wall of infant weak and unstable o Heart muscle less contractile o Alveoli not fully developed until 2 years Pediatric vs Adult Physiologic Differences Infants <2 months obligate nose breathers Immune system immature Developmental – put everything in their mouths Compensate better than adults but crash faster Increase HR and RR Ventilation Defined as movement of air into and out of lungs Inspiration and Expiration Control via pons Chemoreceptors Hypoxic Drive – default control Inspiration Stimulus via pons Transmitted via phrenic nerve to diaphragm Diaphragm flattens, intercostal muscles contract, ribs elevate and expand Results in decreased intrapulmonic pressure (pressure gradient) Air is passively drawn into the lungs and alveoli expand Expiration Stretch receptors in lungs signal respiratory center via vagus nerve to inhibit inspiration (Hering-Breuer Reflex) In non-diseased lungs, natural elasticity passively expels air Chemoreceptors Located in carotids and aortic arch Stimulated by decreased PaO2, increased PaCO2 or decreased Ph Increased PaCO2 considered normal neuroregulatory control of ventilations Hypoxic Drive Default regulatory control of ventilations When changes are sensed in PaO2 Stimulants & Depressants Body temp – increase RR with fever, decreased with hypothermia Drugs/Meds – decrease Pain – usually increases RR Emotion ie Anxiety – Increases Acidosis – Increases Sleep - Decreases Perfusion Defined as process of nutritive delivery of arterial blood to a capillary bed in the biological tissue Need blood flow to alveoli for gas exchange to occur Many things can affect it – scar tissue, fluid, trauma, etc. Hypoxia vs Hypoxemia Hypoxemia is an inadequate supply of oxygen in the blood Hypoxia is inadequate supply of oxygen to the cells and tissues of the body Caused by reduction in partial pressure of oxygen (PaO2), inadequate oxygen transport, inability of tissues to use oxygen Hypoxic Hypoxia A reduction of oxygen entering the blood Reduced oxygen pressure in the lungs Reduced gas exchange area Lung disease Hypemic Hypoxia A reduction in the capacity of blood to carry oxygen Reduced hemoglobin ○ Drugs, Chemicals, Smoking, or Carbon Monoxide exposure Reduced number of red blood cells ○ Decreased production or hemorrhage Improperly formed red blood cells ○ Sickle cell Stagnant Hypoxia A deficiency in oxygen due to poor blood circulation Sitting or hanging for long periods Exposure to cold temperatures Shock states Histotoxic Hypoxia An inability of the tissues to use oxygen Carbon monoxide or Cyanide poisoning Certain narcotics Chewing tobacco and alcohol Respiratory Distress May stem from anywhere in the tracheobronchial tree, lungs/alveoli, pleura, or chest wall Body begins compensation Signs and Symptoms Tachypnea, increase WOB/retractions, nasal flaring, grunting (generates PEEP), tachycardia, tripod or sniffing position, cyanosis, AMS, stridor, wheezing, crackles Respiratory Failure Occurs when compensating mechanisms fail Signs and Symptoms Agonal respirations, bradycardia (imminent arrest), flaccid muscle tone, stuporous ALI and ARDS Acute Lung Injury Defined by PaO2:FiO2 ratio <300 with bilateral infiltrates Precursor to ARDS Acute Respiratory Distress Syndrome PaO2:FiO2 ratio<200 and bilateral infiltrates Diagram you take the PaO2 value from the Arterial Blood gas (let's say it's 100) and you take the FiO2 from the ventilator (let's say it's 30%) and then you divide the PaO2 by FiO2. Now, 30%=0.3 So PaO2/FiO2 ratio would be 100/0.3 = 333 mmHg. If it is 200 or below, you would think of ARDS ARDS Physical damage to lungs Pulmonary edema and alveolar collapse Endothelial dysfunction, fluid extravation from capillaries, impaired drainage from lungs Inflammation of lung parenchyma Impaired gas exchange and release of inflammatory mediators Hypoxia/Hypoxemia ARDS Ground glass appearance on CXR ARDS Mechanical ventilation necessary but also detrimental High FiO2 and positive pressure cause barotrauma and scarring of tissue May lead to SIRS (Systemic Inflammatory Response Syndrome) if not treated properly Break? Common Pediatric Upper Airway Emergencies Croup Epiglottitis Foreign Body Aspiration Trauma Croup Viral, cold symptoms and fever, edema of vocal cords S&S – stridor, barking cough, symptoms worse at night, increased work of breathing, steeple sign Management – Cool mist, racemic epi Epiglottitis Bacterial (haemophilus influenza B), edema of epiglottis and surrounding structures, rapid progression S&S – fever, sore throat, drooling, retractions, sniffing position Management – keep child calm, O2 as tolerated, racemic epi, rocephin IV, intubation by anesthesiologist (one shot), cricothyroidotomy if unsuccessful intubation Epiglotittis Foreign Body Aspiration Highest risk from 6 months to 5 years, object can be lodged anywhere in respiratory tract S&S – coughing, stridor in upper, wheezing in lower, increased work of breathing Management – remove foreign body only if you can see it, intubation?, bronchoscopy Trauma Trauma Many types and causes Facial fractures – most involve lower jaw(most vulnerable),falls, MVA, sports Choking – choking game, abuse Hanging – second most common method of suicide, if death not immediate, delayed airway obstruction from edema and/or trauma, intubation difficult Smoke inhalation - high temperature burns airway, edema can close airway within 30 minutes Management – maintain patent airway Common Pediatric Lower Airway Emergencies Asthma/ RAD RSV pneumonia BPD Toxins – Hydrocarbons Trauma Asthma Hyper-reactive airways (RAD), various triggers produce bronchial edema, constriction and increased mucous production S&S – wheeze (expiratory, inspiratory, or none),tachypnea, retractions Management – O2, bronchodilators/beta2agonist, methylprednisone 1-2mg/kg, magnesium 25-50mg/kg, *terbutaline, theophylline, mechanical ventilation Respiratory Syncytial Virus (RSV) Premature babies and infants more susceptible, can be life threatening S&S – cold-like symptoms, copious, thick upper airway secretions, may present with apnea Management – Supplemental O2, good pulmonary toilet, nasal suctioning Bronchopulmonary Dysplasia (BPD) Premature baby born with 10% of adult alveoli requires mechanical ventilation Prolonged exposure to high FiO2 and PPV causes barotrauma and scarring of existing alveoli Baby becomes more difficult to ventilate, provider increases pressure and/or FiO2 and new forming alveoli are scarred as well BPD Abnormal development of lung tissue, children continue to grow more alveoli until around two years of age Lungs less compliant BPD fits low to no functional reserve common tracheostomy (2/3 of resistance in upper airway) Very important to use lung protective strategies Toxins Toxins Hydrocarbon aspiration Toxic hydrocarbons, CHAMP – Camphorated, Halogenated, Aromatic, heavy Metals and Pesticides Found in lamp oil, gasoline, turpentine, furniture polish, propellants, glue, freon, liquid paper Penetrates deep into tracheobronchial tree causing inflammation, bronchospasm and air leak syndrome Rapidly progresses to pulmonary edema and respiratory failure, CNS and cardiovascular complications Hydrocarbon Aspiration Air leak syndrome Pneumothorax Tension pneumothorax Pneumomediastinum Pneumopericardium Management No antidote NO gastric emptying Lung protective strategies Trauma Pulmonary Contusions Hemothorax/pneumot horax Management – chest tubes, FOCA Tension Pneumothorax Needle decompression Steam Inhalation burns HFOV Others to consider Cystic Fibrosis – hereditary, mucous glands of lungs, liver, pancreas and intestines + weak immune system; hypoxic hypoxia Sickle Cell anemia – genetic, red blood cells sickled; hypemic hypoxia Carbon monoxide poisoning – carboxyhemoglobin has higher affinity to RBC’s; histotoxic hypoxia Apnea of Prematurity – brain not developed babies <35 weeks gestation, begins after 2 days and continues for 2-3 months Tracheomalacia – floppy airway, stridor, positional, supportive care Tracheoesophageal fistula (TEF)commonly associated with esophageal atresia, VACTER syndrome, surgical repair Diaphragmatic hernia – stomach and/or bowel in thoracic cavity, defects depend on when formed, ECMO,surgical repair Break Time Congenital Defects Fetal Circulation Fetal Circulation The placenta provides oxygenated blood from the mother to the fetus. Instead of perfusing the lungs, blood is shunted from the pulmonary artery to the aorta by way of ductus arteriosus At birth The fluid that filled the alveoli is expelled during delivery or absorbed by lung tissue, the alveoli expand with the first breath An increase in systolic blood pressure occurs when the umbilical cord is clamped, PVR falls to ½ SVR With exposure to oxygen, SVR increases, thus decreasing blood flow through ductus and increasing blood flow to lungs Problems with transition Insufficient breathing – fails to force fluid from lungs and increase oxygen Systemic hypotension – excessive blood loss, poor cardiac contractility, or bradycardia Failure of blood vessels in lungs to dilate Persistent Pulmonary Hypertension (PPHN) Hypoxemia secondary to increased pulmonary vascular resistance When transition does not occur as it should, the body shunts blood through fetal structures Blood flow through foramen ovale or ductus arteriosus occurs with unoxygenated blood entering system, can also cause right sided heart failure Present with cyanosis and SOB, treat with indomethacin, long term with viagra Why am I telling you this? High risk for altered respiratory function Presents to you as respiratory problem Categories: Acyanotic=left-to-right shunts, CHF Obstructive=restrictive blood flow Cyanotic=right-to-left shunts, pt is purple Oxygen will either do nothing or be bad 5 Most common Ventricular Septal Defect Hypoplastic Left Ventricle Coarctation of the Aorta Tetralogy of Fallot Complete Transposition of the Great Arteries Patent Ductus Arteriosus – PDA (acyanotic) Oxygen sensitive Stays anatomically patent with hypoxemia for weeks to months after birth Normally begins closing 24-36 hours after birth Ductal dependent lesion Ventricular Septal Defect Usually benign Hypoplastic Left Ventricle (obstructive/mixed) Left Ventricle did not develop Blood flows from left atrium to right atrium Right to left across PDA Signs & symptoms – CHF, tachypnea, increased WOB, grunting Management – Prostaglandin, Oxygen can be bad Surgical repair Coarctation of the aorta (obstructive) Narrowing of the aorta Usually infants > 1 week Pre or Post ductal – important S&S – cyanosis, tachypnea, tachycardia, CHF Management – Prostaglandin O2 can be Bad surgical repair Coarctation of the aorta Tetralogy of Fallot (cyanotic) Signs & Symptoms Low O2 Sats TET spells “Boot” shaped heart Right to Left shunt Management Prostaglandin O2 won’t help 2 staged surgical repair – BlalockTaussig shunt and total repair TET Spells Transposition of Great Arteries (cyanotic) Signs & Symptoms Cyanosis, Tachypnea, Retractions Poor feeding/FTT With VSD, not recognized until CHF Management Prostaglandin O2 won’t help Atrial septostomy Arterial switch Airway adjuncts Conscious patient Conscious Nasopharyngeal Airway/Nasal Trumpet Length=distance from nares to meatus of ears Unconscious patient Oropharyngeal Unconscious Airway/OPA Holds tongue out of the way Length=distance from corner of mouth to meatus of ears Oxygen delivery Nasal Cannula Venturi Mask Non rebreather (NRB) High flow Nasal Cannula Positive Pressure Delivery Basics – BVM BiPAP/ CPAP Definitive Airways LMA King Tube ETT: nasal, oral, retrograde, cricothyroidotomy Transtracheal Jet Insufflation Indicators for Intubation Ventilatory Support Tachypnea and increased WOB Inadequate rate, depth Protection/Patency of Airway GCS <8 Edema due to burns, trauma, infectious process Positive Pressure Delivery Pneumonia Pulmonary Edema Ventilatory Support Can't Maintain Ventilation/Oxygenation SaO2 <90% on High Flow O2 or PaO2<60 on FiO2>40% PaCO2 >55 if baseline is normal, or >10 increase from baseline Respiratory Rate Expected decline in Clinical Status Deterioration/Impending Compromise Transport Airway protection during procedures (ie. endoscopy) Protection patency of airway Can't Protect Airway Gag reflex is absent in up to 37% of population, so a poor predictor of airway protection Can they talk? Can they swallow and manage secretions Other Reasons: Supply/Demand imbalance of perfusion. Mechanical Obstruction, or need for Core Rewarming, Inadequate respiratory compensation for met acidosis CO2 should=(1.5 [HCO3-] + 8) ± 2 LMA Cuff device provides sufficient seal for PPV Indication for Use: Endotracheal intubation not desired Emergent mask ventilation not possible/adequate Intubation fails King Tube Supraglottic airway Proximal cuff seals nasopharynx and oropharynx Distal cuff seals esophagus Smallest tube for 12kg patient Indication for Use: Same as LMA Suspected c-spine Endotracheal Tube Made from polyvinyl chloride with radiopaque line from top to bottom Cuffed vs Uncuffed Hole at beveled, distal end Murphy’s Eye External insertion depth marks Sizes range 2.5-8, estimate pinky finger or (age/4) +4 Stylette/ Bougie Stylette Bougie Nasotracheal Intubation Indications Conscious patient Complications Esophageal Status epilepticus Anaphylaxis Anatomy Contraindications Apnea Basilar skull fracture/ facial trauma Bleeding disorders placement Epistaxis Vagal stimulation Trauma to vocal cords/paralysis Injury to nasal turbinates How do you intubate this guy? Orotracheal Intubation Indications Complications Definitive airway – Esophageal protect airway GCS<8 placement Right mainstem Vagal stimulation Trauma to vocal cords/paralysis Contraindications Semi-conscious/gag Unstable c-spine trauma Assessing airway for difficulty ASA classification Malampati scores History Obvious trauma or deformities Position patient Look for landmarks Retrograde Intubation Indications Complications Conscious patient False passage of Difficult/Unable to guidewire Bleeding/ hemoptysis larygospasm intubate Suspected c-spine Contraindications Laryngotracheal disease Anatomy Coagulopathy Retograde intubation Fiberoptic and Glidescope Trachlight Cricoidectomy – Not typically used in pediatrics Indications Complications Unable to intubate Subglottic stenosis Airway obstruction Laceration of Trauma to face/upper esophagus Injury to laryngeal structures Air leak syndrome airway Unstable c-spine Contraindications Coagulopathy Anatomy Lack of practitioner skill Transtracheal Jet Insufflation Indications Unable to intubate Contraindications Anatomy Complications Perforation of esophagus Bleeding Subcutaneous emphysema Air leak syndrome Hypoventilation Expiratory obstruction Tracheostomies – This is your airway To RSI or Not To RSI, that is the question. 6 P’s of RSI Preparation Preoxygenation Pretreatment Paralysis Placement Post-intubation Preparation Assess for difficulty Prepare drugs Patent IV Prepare Equipment ETT Miller blade/light Oxygen and Suction (on and working) Co2 detector Position patient (roll) Difficulty? Preoxygenate and Pretreat 100% O2 for 5 minutes Non-rebreather vs BVM Want sats of 100% Use of atropine? (hypoxia bradycardia, masking) Give analgesic Morphine 0.1mg/kg– not with asthma Fentanyl 1mcg/kg Give sedative Versed 0.1mg/kg Ketamine 0.5-2mg/kg Propofol 0.5-1mg/kg Paralysis Non-depolarizing neuromuscular blockade only! Vecuronium 0.1mg/kg Rocuronium 1mg/kg (Sugammadex) Gantacurium – new shorter duration Emesis cannot occur Wait until no movement Depolarizing Neuromuscular Blockade Non-Depolarizing Neuromuscular Blockade Persistent agonist at Competitive nicotinic receptor sites Fasciculations Short duration of paralysis (5-10min) Side effects are many antagonist at nicotinic receptors Longer duration of paralysis (30-40min) Virtually no side effects Depolarizing Problems associated with depolarizing neuromuscular blockade include Myalgia (muscle soreness), Hyperkalemia Increased ICP Atypical interactions in some individuals Depolarization will induce the release of potassium from skeletal muscle Malignant hyperthermia is rare but lethal Recovery cannot be accelerated by administering medications Non-depolarizing Recovery from paralysis with non-depolarizing neuromuscular blockers can be accelerated by administration of a cholinesterase inhibitor (ie Pyridostygmine). These agents cause muscle paralysis in a predicted sequence (and recovery in the opposite sequence): muscle of fine movement (eye, jaw, larynx) limbs trunk intercostals diaphragm Placement Hold all ventilations unless sats fall below 90% Watch for bradycardia Using Miller/straight blade, sweep tongue to left, go past the epiglottis and lift without rocking Sellick’s maneuver aka cricoid pressure Visualize cords and pass through Confirm placement Post intubation management Secure the tube Initiate mechanical ventilation Insert naso- or orogastric tube Monitor patient continuously Gold Standard: Clinical Exam Look for symmetrical chest rise and misting in tube Auscultation of epigastrum Auscultation of bilateral lung fields including axillae Change in Skin Color/Improvement in patient Oxygen Saturations Oxygen Saturation PaO2 90% 60 movement 75% 40 perfusion 50% 27 Sensitive to light CO2 Detectors – Depend on perfusion Capnography Many EMS have in Ambulances Useful for trending over periods of time Can lose reading Studies finds 70% accuracy in determining placement in post cardiac arrest pt Colorimetric CO2 detector Yellow=Yes Purple=Problem May take 4-6 ventilations before color change Esophageal Detector Bulb shape Squeeze then place on end of ETT If self-inflates, tracheal intubation due to rigid cricoid cartilage Studies finds 99100% accurate, more accurate than ETCO2 (70-86%) Chest xray Placement- tip of ETT should be no lower than 1-2 cm above the carina No higher than 1st rib Remember 1cm of movement in adult ok, 1cm of movement in infant or child=extubated Break for Lunch Remember in each case Proper technique- ability to see important landmarks Orientation of the film- left or right marked Good inspiratory effort Recognize film artifacts Systematic Approach Pertinent clinical history Top to bottom Determine orientation- clavicles Airway Inspiratory vs Expiratory- count ribs (10 above diaphragm) Heart – shape, size 50% or less, aortic knob Clear costo-phrenic angle/ cardiophrenic angle Pulmonary vasculature, Fluid or Air Fractures/Trauma Mnemonic A. Airway and adenopathy B. Bones and breast shadows C. Cardiac silhouette. D. Diaphgram E. Everything else F. Fields Normal Chest Trachea Midline Thymus- water dense mass in superior mediastinum. Usually wavy contour. Bilobed but not always symmetrical. Heart- water dense with apex to left. Occupies about 50% of chest at widest point. Aortic knob seen through thymus on left Pulmonary vessels- seen best on lateral view. Extend to mid lung tapering gradually Lungs- uniformly aerated. Appear black Bony structures- ribs, upper thoracic vertebral bodies, scapulae and clavicles Diaphragm- right and left equal Normal Chest Group Activity Tension Pneumothorax Pleural Effusion Pneumopericardium vs Pericardial Effusion Pneumomediastinum Hydrocarbon Aspiration vs Pneumonia 4 month old premature infant More history Ex 33 weeker. Required BVM resuscitation at birth. 48 hours of ventilator and two weeks total in NICU until feedings were adequate Hospitalized at 2 months for severe bronchiolitis Lives with mother who smokes and 4 year old sibling who attends day care Physical exam What do you want to know?? Which is the most likely diagnosis? Asthma/ RAD Bronchiolitis Bronchiolitis Although this is his second episode of wheezing, a diagnosis of asthma in a child this young is unlikely Most likely Viral bronchilotis Why is this most likely? What treatment? 15 month old Wheezing in morning and worsened throughout the day Not taking fluids or eating Physical Exam General Vitals Head to toe What is going on? Possible diagnosis What do you need to do? References Fojt, Diane F. (2008) The Advanced Airway Course. Tampa, FL: MECA Gaedeke, M.K. (1996) Pediatric and Neonatal Critical Care Certification Review. St. Louis, MO: Mosby Emergency Nurses Association (2007) Trauma Nursing Core Course (6th ed.). Des Plaines, IL: ENA Emergency Nurses Association (2004) Emergency Nurse Pediatric Course (3rd ed.). Des Plaines , IL: ENA Slota, Margaret C. (1998) Core Curriculum for Pediatric Critical Care Nursing (1st ed.). Philadelphia, PA: W.B. Saunders Waldrop, Julee (2008) Basics of Xray Interpretation in Infants and Children. www.unc.edu/courses Whitethorn, Deborah (2000) Pediatric Airway Management and Respiratory Distress. Alaska EMSC website www.ems-c.org Washington State Emergency Medical Services for Children (1990) Alaska Pediatric Prehospital Emergency Course. Seattle, WA www.ems-c.org Emergency Medicine & ED Critical Care EMCrit.org Canadian Journal of Anesthesia Cja-jca.org Center for Pediatric Emergency Medicine at NYU TRIPP (Teaching Resource for Instructors in Prehospital Pediatrics) cpem.med.nyu.edu C.S. Mott Children’s Hospital med.umich.edu/mott/chc J Trauma 2004;57(5):993-997 J Accid Emerg Med 1999:16(6):444 Lancet. 1995 Feb 25;345(8948):487-8 Clin Otolaryngol. 1993 Aug;18(4):303-7 Bozeman WP, Hexter D, Liang HK, Kelen GD: Esophageal detector device versus detection of end-tidal carbon dioxide level in emergency intubation. Ann Emerg Med. 1996 May;27(5):595-9 Takeda T, Tanigawa K, Tanaka H, Hayashi Y, Goto E, Tanaka K: The assessment of three methods to verify tracheal tube placement in the emergency setting.Resuscitation. 2003 Feb;56(2):153-7. Schaller RJ, Huff JS, Zahn A: Comparison of a colorimetric end-tidal CO2 detector and an esophageal aspiration device for verifying endotracheal tube placement in the prehospital setting: a six-month experience.Prehosp Disaster Med. 1997 Jan-Mar;12(1):57-63.